CASE REPORT | https://doi.org/10.5005/jp-journals-10029-1194 |
Ocular Prosthesis with an Art: A Case Report
1–6Department of Prosthodontics and Crown and Bridge, Army Dental Centre, Research and Referral, Delhi Cantt, New Delhi, India
Corresponding Author: Rachana Chaudhary, Department of Prosthodontics and Crown and Bridge, Army Dental Centre, Research and Referral, Delhi Cantt, New Delhi, India, Phone: +91 7023283220, e-mail: Chaudhary.rachana@gmail.com
How to cite this article Chaudhary R, Kumar D, Khattak A, et al. Ocular Prosthesis with an Art: A Case Report. Int J Experiment Dent Sci 2019;8(1):26–31.
Source of support: Nil
Conflict of interest: None
ABSTRACT
The eye is a vital organ and an important part of facial expression. Loss of one or both eyes causes social, psychological and physical distress to the patient. The aim of an ocular prosthesis is to restore the facial appearance, improve self-confidence and social acceptance. There are various materials and techniques used for the fabrication of the ocular prosthesis. Advantage of custom ocular prosthesis over stock eye prosthesis includes better movements of the eyelid, even distribution of pressure, thereby reducing the chances of trauma to the tissue bed, better fit, comfort and esthetics. With the custom ocular prosthesis size, shape, color of the iris, pupil and sclera can be properly customized making it look more natural. This article illustrates rehabilitation of the eviscerated right eye of a 28-year-old male with a custom-made ocular prosthesis with manual painting of iris and sclera with oil colors.
Keywords: Artificial, Esthetics, Eye, Paintings.
INTRODUCTION
Eyes they say are the “windows to the soul.” Loss or absence of any part of the face especially eye can cause severe physical and psychological trauma.1 Loss of eye could be because of trauma, congenital defect, painful blind eye, malignancies or sympathetic ophthalmia.2 Depending on the severity, surgical management includes one of the three approaches: evisceration, enucleation or exenteration.3 Emotional distress because of loss of eye can be improved by an ocular prosthesis, which simulates the natural eye. An artificial eye is an alloplastic prosthesis restoring a person’s identity and reintegrating him/her in society.
There are several materials and techniques in the literature for the fabrication of ocular prosthesis. It may be using a stock eye, modifying stock eye on the positive replica of the ocular defect or fully customized ocular prosthesis. In custom ocular prosthesis, sclera and iris both are custom made. First two techniques in which stock eye is used are less time-consuming but have the few disadvantages like esthetics are compromised and have unsatisfactory fit. Custom made ocular prosthesis provides better fit and improved esthetics, but they are more time-consuming and needs more patience and expertise.4 Whenever possible stock eye prosthesis should be given as interim prosthesis. This case report demonstrates an innovative technique for fabricating custom ocular prosthesis with manual scleral and iris painting using oil paints which provides esthetically satisfactory result with comfortable and better fit.
CASE DESCRIPTION
A 28-year-old male reported to the Department of Prosthodontics at Army Dental Centre Research and Referral, Delhi with chief complaint of missing right eye for 2 years. History revealed that the eye was lost after it got injured with a splinter 2 years back. He sustained multiple injuries and was given a stock eye prosthesis by the surgeon which patient was wearing for two years. On general examination, patient was moderately built and nourished, well conscious and oriented to time, place and person, and was highly motivated and had realistic expectations. There was no sign and symptom suggestive of any systemic illness, vitals were within normal limit. Routine blood and radiographic investigations were carried out to rule out any pathology. Examination of existing stock eye prosthesis was done; which patient was wearing for two years. Size of the prosthesis was very small, ill fitted and not matching with the contralateral eye. Patient was also not satisfied with the esthetics (Figs 1 and 2).

Fig. 1: Preoperative extraoral view
MATERIALS AND METHODS
Examination of socket was done, which was healed satisfactorily and mucosa was healthy. There was adequate volume and sulcus depth to retain and support the prosthesis. Ocular bed was moist and there was restriction in movement (Fig. 3).
Based on the clinical findings and history, the case was diagnosed as eviscerated right eye secondary to trauma. Various treatment options were considered and keeping in mind the advantages of custom eye over stock eye, it was decided to rehabilitate the patient with a custom made ocular prosthesis with direct impression technique. Comprehensive treatment plan was formulated and entire treatment procedure was explained to the patient with its limitations and his consent was obtained.
Impression Procedure
To provide a custom ocular prosthesis, an accurate impression of the ocular defect of the right was first obtained. Patient was made to sit comfortably on the dental chair and impression procedure was explained. An ophthalmic topical anesthesia was applied to make the comfort the impression procedure comfortable, a 10 cm of black suture was placed carefully which helped in easy retrieval of the impression. Polyvinyl siloxane impression material of the heavy body consistency was used to make the impression of the defect; because of its high viscosity material is self-supportive and mouldable.5 Impression material was injected directly into the ocular socket by a syringe without using any custom or stock tray to carry the material. Direct impression without using any type of tray eliminates interferences in the closure of lids while making an impression. Once the material completely fills the socket, patient was advised to close the eye and perform various ocular movements until material sets. After complete setting of the impression material it was carefully retrieved with a rubber suction cup and holding the suture. After the impression sets, it was ensured that all surfaces of the impression were recorded in a functional form and examined for defects and voids. Any excess impression material is trimmed off (Figs 4 and 5).
Fabrication of the Cast
Impression was poured with type IV dental stone in an acrylic mixing cup. After complete setting, it was sectioned using two halves keeping in mind the orientation of the ocular impression (Fig. 6).
Fabrication of the Wax Pattern
The two pieces of mold cavity were again joined by sticky wax and placed back in the acrylic mixing cup. A layer of Vaseline was applied all over the stone surface and molten wax was poured into stone mold to create a wax pattern of the prosthesis and allowed to set (Fig. 7).
On complete hardening, wax pattern was smoothened to remove any sharp ridges or undesirable irregularities, properly contoured and then polished (Fig. 8).

Fig. 2: Previous ocular prosthesis

Fig. 3: Intraocular view

Fig. 4: Direct ocular impression

Fig. 5: Ocular impression

Fig. 6: Two-piece mold

Fig. 7: Molten wax poured in the two-piece mold

Fig. 8: Wax pattern

Fig. 9: Iris location marked with vernier caliper

Fig. 10: Wax pattern trial
Centering of Iris
A transparent graph was used for the measurements to mark the location and position of the iris. Vertical lines coinciding with medial, middle and lateral extremities of patient’s contralateral iris were marked, similarly horizontal line coinciding with the center of the iris was marked. These lines were then transferred to the wax pattern using vernier caliper and marked (Fig. 9).
Wax Trial
Try in was done to check for proper, fit, contour and bulk. This procedure was repeated until satisfactory results were obtained matching with patient’s contralateral eye (Fig. 10).
Fabrication of Scleral Shell
Flasking, dewaxing and packing were done conventionally using clear PMMA monomer and polymer with white coloring agent which will give the sclera a characteristic white color. Long curing cycle was carried out for acrylization. After curing scleral shell was carefully removed. Trimming and polishing was done to get a smooth shiny scleral shell. Care was taken not to alter the outline of the iris on the scleral shell (Fig. 11).
Iris and Scleral Painting
Finished scleral blank was tried in the patient and position of the iris was once again verified. The initial step in painting an artificial iris is careful observation of the color, size, and morphological elements of the patient’s iris under indirect natural light and then a high-quality photograph of patient’s contralateral eye was used for iris and scleral painting. Painting was done with student oil paint and thin brushes. Painting was done in two steps: iris painting followed by scleral painting.
Iris Painting
There are five basic parts to an iris painting: the pupil, the collarette, the stroma, the background (limbus), and the individual markings or striations. Using a thin brush and artist oil paint, many strokes from the center of the iris to the periphery were painted to match the color of natural iris. Coloring was done in layers to get more lifelike appearance 1st layer, background color; 2nd layer, color around the pupil; and 3rd layer, an additional lighter striation was applied to give the painting a 3D effect. A black spot was painted in the center of the disk to represent the pupil. Each layer was allowed to completely set before applying the next coat (Fig. 12).
Scleral Painting
Basic requisites in matching the sclera with fellow eye was achieved by careful reproduction of conjunctival vascular patterns near medial, lateral canthi and circumcorneal region and location of yellow, black or brown pigments in the prosthesis similar in the sclera of the contralateral eye. Red color was used to mimic the blood vessels (Fig. 13).
Second-stage Curing
After the eye painting was complete, it was allowed to set. Painting was secured in place with monopoly syrup. Second stage curing was done by packing the painted eye back in the original mold, curing cycle was repeated. After complete curing, final prosthesis was removed and trimming was done (Fig. 14).
Finishing and Polishing
Finishing and polishing was done using finishing burs, pumice and buff to get a natural glossy appearance of the artificial eye (Fig. 15).
Insertion and Instructions
Before insertion of the finished prosthesis, 70% isopropyl alcohol and 0.5% chlorhexidine solution was used to disinfect the prosthesis. Prosthesis was thoroughly cleaned with saline solution to prevent chemical irritation, it was inserted and checked for fit, contour, and movements. Patient was demonstrated about proper insertion and removal the prosthesis. Necessary post insertion instructions were given to the patients6 (Fig. 16).

Fig. 11: Scleral shell

Fig. 12: Iris painting

Fig. 13: Scleral painting

Fig. 14: Final prosthesis
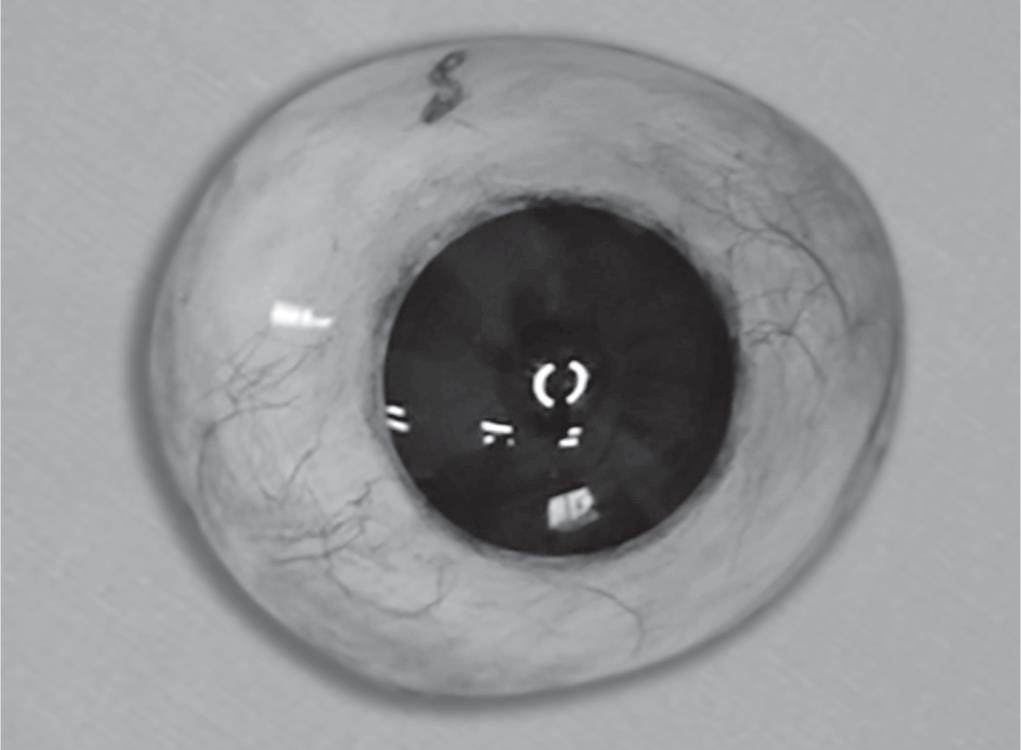
Fig. 15: Ocular prosthesis after finishing and polishing

Fig. 16: Post-insertion view
RESULTS
Patient who came to us with an ill fitted, unesthetic stock eye prosthesis, was rehabilitated with a customized ocular prosthesis with better fit, comfort and esthetics. Characterization was done by manual iris and scleral paintings with oil color which gave it more natural and lifelike appearance. It was a time-consuming and precision work with lot of artistic skills. The iris colors could match the contralateral eye and at the end we were able to meet up to his expectations. Patient was highly satisfied with his new prosthesis and he complemented that though he cannot see the world but at least he can face the world.
DISCUSSION
Every human being is created with a pair of eyes which serve as sense organs of sight and adds to the beauty of the face. It also performs various other functions including a very important role in nonverbal communication. Unexpected trauma, pathology or congenital deformity may necessitate a surgical intervention leading to the loss of eyeball.2 Ocular disfigurement can drastically lower the victim’s quality of life through its physical and psychological handicap.7
Due to the great concern about re-establishing facial balance, the art and science of fabrication of artificial eye date back to remote times, its first manifestations being in the primordial times of human history.8
In literature several techniques for fabricating artificial ocular prostheses are documented. An esthetically acceptable ocular prosthesis is one which reproduces the color, size, shape, contour of the iris and allows the patient to return to a normal lifestyle. Use of a stock eye is economical, but such a prosthesis is not perfectly adapted to the tissue bed of the eye and usually causes discomfort and does not fully satisfy the patient’s expectations. Improved esthetics can be achieved when color and position of the iris can be matched with the normal contralateral eye, and this can be made possible with ocular prosthesis which are fully customised according to patient.9 Prosthetic rehabilitation with a custom-made ocular prosthesis can yield better and more satisfactory results for the patient both esthetically and psychologically as compared to a stock eye prosthesis.
Acrylic resin for the fabrication of ocular prosthesis has following advantages like durability, biocompatibility, easy to color, economical, easy to clean, reliable mechanical retention; therefore, it is the one of the materials of choice to fabricate ocular prosthesis. For the fabrication of ocular prosthesis white pigmented (N1) and colorless acrylic resins are used to match the artificial sclera.10
Iris Painting Techniques
Various factors play an important role in determining the esthetic outcome of iris painting.
Quality of Iris Paint
Depending on the surface, different colors can be used, like varnishes and gouache, acrylic, oil, and automotive paints. Gouache and acrylic paints have been used to color the iris, but they present color alterations. Oil paint has better cooler stability and durability when exposed to environmental conditions.11
Surface on which the Irises are Painted
Iris painting can be done on ethyl cellulose discs, acetate, and the colorless acrylic ocular bottom, paper discs or directly on the acrylic resin sclera.
Colorless Acrylic Resin Covering
A layer of colorless acrylic resin is applied to cover the characterized blood vessels and artificial iris. This layer provides translucency similar to the artificial iris and gives more natural appearance to the artificial eye.
CONCLUSION
Human irises have a layered and highly complex structure which is difficult to mimic. Custom made ocular prosthesis has many advantages over stock eye prosthesis like, better color matching, contouring, more coordinated movements with the contralateral eye. Success of ocular prosthesis mainly depends on the precision, knowledge and artistic skills of the clinician.
DECLARATION OF PATIENT CONSENT
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
REFERENCES
1. Cain JR. Custom ocular prosthetics. J Prosthet Dent 1982;48(6):690–694. DOI: 10.1016/S0022-3913(82)80030-9.
2. Raflo GT. Enucleation and evisceration. In: ed. W, Tasmun E, Jaeger ed. Duane’s Clinical Ophthalmology,vol. 5 Phildelphia: Lippincott-Raven; 1995. pp. 1–25.
3. Parr GR, Goldman BM, Rahn AO. Surgical considerations in the prosthetic treatment of ocular and orbital defects. J Prosthet Dent 1983;49(3):379–385. DOI: 10.1016/0022-3913(83)90281-0.
4. Benson P. The fitting and fabrication of a custom resin artificial eye. J Prosthet Dent 1977;38(5):532–538. DOI: 10.1016/0022-3913(77)90029-4.
5. Tripuraneni SC, Vadapalli SB, Ravikiran P, et al. An innovative impression technique for fabrication of a custom made ocular prosthesis. Indian J Ophthalmol 2016;63(6):545–547. DOI: 10.4103/0301-4738.162626.
6. Parr GR, Goldman BM, Rahn AO. Postinsertion care of the ocular prosthesis. J Prosthet Dent 1983;49(2):220–224. DOI: 10.1016/0022-3913(83)90506-1.
7. Lubkin V, Sloan S. Enucleation and psychic trauma. Adv Ophthalmic Plast Reconstr Surg 1990;8:259–262.
8. Gordon B. The ancient origins of artificial eyes. Annuals of Medical History, (series 2) New York: Paul B. Hoeber; 1940; p. 58.
9. Goiato MC, Micheline D, Dds H, et al. An alternate impression technique for ocular prostheses. J Prosthodont 2013;22(4):338–340. DOI: 10.1111/j.1532-849X.2012.00945.x.
10. Raizada K, Rani D. Ocular prosthesis. Cont Lens Anterior Eye 2007;30(3):152–162. DOI: 10.1016/j.clae.2007.01.002.
11. Fernandes AU, Goiato MC, Batista MA, et al. Color alteration of the paint used for iris painting in ocular prostheses. Braz Oral Res 2009;23(4):386–392. DOI: 10.1590/S1806-83242009000400007.
________________________
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by-nc/4.0/), which permits unrestricted use, distribution, and non-commercial reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.