

Key points
- Evaluation remains a diagnostic challenge
- Selective nonoperative management is being increasingly adopted following contrast-enhanced CT scan in haemodynamically stable patients with serial clinical assessment by an experienced clinician
- Damage control laparotomy (DCL) is a key component of damage control resuscitation
Introduction
Injuries to the abdomen present a complex diagnostic challenge and continue to cause significant morbidity and mortality whether blunt or penetrating in nature. Regardless of injury type, the initial assessment and management are the same.
Motor vehicle collisions remain one of the commonest causes of blunt abdominal injury and there has been a comparative rise in the incidence of seatbelt-induced abdominal injuries, even though the incidence of head and thoracic injuries has decreased.
Penetrating abdominal trauma is commonly classified into stab wound or ballistic injuries. Both can present with an apparently minor abdominal injury, yet be associated with major intra-abdominal trauma. Ballistic injuries can be further subdivided into low-kinetic energy or high-kinetic energy wounds.
Pathophysiology
Solid organ injury
The commonest organs to be injured in blunt abdominal trauma are the spleen, liver, kidney and pancreas, in that order. In penetrating trauma, the order differs, with the liver being the most commonly affected organ, followed closely by the spleen, kidney and pancreas. Blunt trauma results in injury through two main forces: compression and shearing. Shearing forces result in disruption of the attachment points of an organ and lacerations of the organ and parenchyma. In severe road traffic collisions, this may also result in disruption of the vascular structures supplying the organ. Penetrating injuries are less frequent, but can result in considerable trauma to solid organs, especially as result of gunshot wounds.
Hollow viscus injury
The hollow organs located in the abdominal cavity can be divided into gastrointestinal and urinary viscera. The gastrointestinal viscera consist of the stomach, duodenum, jejunum, ileum, colon and rectum; the urinary viscera are the ureters and urinary bladder (the kidneys are retroperitoneal).
Blunt injury is estimated to cause bowel injury in approximately 1% of patients, with bowel or mesenteric injury resulting from compression against hard structures, from a sudden compressive rise in intraluminal pressure or from shearing forces generated by acceleration and deceleration particularly at fixed points such as the ligament of Treitz (the suspensory muscle of duodenum).
These shearing forces are exerted on the origins of small vessels resulting in avulsion, rupture and intimal injury. The consequence of this may be catastrophic haemorrhage or thrombotic occlusion of the vessel and distal necrosis.
Injuries to the diaphragm
Diaphragmatic injuries are notoriously difficult to diagnose, but should be suspected in casualties who have suffered thoracoabdominal penetrating trauma or blunt injury to the abdomen.
Clinical features
The clinical features of abdominal trauma are largely dependent on the injury pattern and the organs affected. Abdominal examination follows the basic principles of inspection, palpation, percussion and auscultation. Unfortunately, the initial assessment of patients with blunt abdominal trauma is often difficult and is notably inaccurate. Associated injuries, pain and anxiety often cause tenderness and spasm in the abdominal 2wall and make diagnosis difficult. The most reliable signs and symptoms in alert patients are pain, tenderness, haematemesis, per rectal blood loss, hypovolaemia and evidence of peritonitis. However, large amounts of blood can accumulate in the peritoneal and pelvic cavities without any significant or early changes in the physical examination findings.
A detailed knowledge of the underlying anatomy of the intra-abdominal organs is the key to successfully managing a polytrauma casualty. Bruising or the stigmata of trauma over a particular region of the abdomen may highlight which organs have suffered traumatic insult. The abdominal examination must be thorough and systematic.
Pelvic injury and instability should be assessed radiologically since examination may cause clot dislodgement and consequent haemorrhage.
The presence of a pelvic fracture indicates a raised probability of lower urinary tract injury as well as pelvic and retroperitoneal haematoma. If there is the presence or suspected presence of a urethral injury, a retrograde urethrogram will be needed. In practice, this may be difficult in an acute setting, and a suprapubic catheter may be required.
A sensory examination of the chest and abdomen must be undertaken to evaluate the potential for spinal cord injury.
If present, a spinal cord injury may interfere with the accurate assessment of the abdomen by causing decreased or absent pain perception.
A rectal and vaginal examination should be performed to search for evidence of bone fragment penetration resulting from a pelvic fracture and the stool should be evaluated for gross or occult blood. Rectal tone should be assessed to identify spinal injury and the prostate palpated to identify potential urethral injury.
Evaluation and diagnosis
A number of imaging modalities are available to assist in identifying injuries and monitoring changes in condition:
- Focus abdominal sonography for trauma (FAST) scan
- Plain radiographs
- CT scan of the abdomen
- Interventional angiography
The importance of other investigations and monitoring such as electrocardiography, conventional vital signs, oximetry, capnography and blood gas analysis should not be overlooked.
Blunt trauma
The Eastern Association of Surgery of Trauma (EAST) in the USA has systematically reviewed modalities for the evaluation of blunt abdominal trauma. Radiographs, especially of the chest and pelvis, still remain useful in determining the presence of intrathoracic or abdominal injury. If a spinal injury is suspected, then an erect chest radiograph may not be feasible, thereby limiting diagnosis of free intraperitoneal air.
The FAST scan allows the rapid examination of body cavities by appropriately trained personnel. FAST may be considered to be the initial diagnostic modality for exclusion of haemoperitoneum. In a recent prospective study of 2576 patients, FAST had a sensitivity of 87% and a specificity and negative predictive value of 98% for detecting haemoperitoneum. It will not detect or grade severity of visceral injury alone.
CT with intravenous contrast is recommended for the evaluation of patients with equivocal findings on physical examination, associated neurologic injury, or multiple extra-abdominal injuries. Under these circumstances, patients with a negative CT should be admitted for observation. CT is the diagnostic modality of choice for nonoperative management of solid visceral injuries. The advent of multislice CT has fundamentally changed the way trauma patients are managed. CT has a number of advantages including higher speed of data collection, thinner sections and reduced artifactual abnormality. CT scanning is more often undertaken in the stable patient, and has a sensitivity approaching 98% and specificity of 99%. Its advantage over other investigations is that it is the only investigation which allows imaging of retroperitoneal structures as well as grading of the severity of injury.3
Penetrating trauma
Patients with penetrating abdominal trauma are at high risk of life-threatening injuries. While many patients will be in need of emergent operative intervention, some patients may be safely managed nonoperatively.
- Haemodynamic instability, shock, evisceration and peritonitis mandate immediate laparotomy following penetrating abdominal trauma
- Thoracoabdominal stab wounds should be further evaluated with chest X-ray, ultrasonography and laparoscopy or thoracoscopy
- Wounds to the back and flank should be imaged by CT scanning
- Anterior abdominal stab wounds without peritoneal signs of evidence of haemoperitoneum on FAST examination may be followed with serial clinical assessments by an experienced clinician but with a low clinical threshold for operative intervention
- The majority of patients with gunshot wounds are best served by laparotomy, although in select patients a nonoperative approach may be adopted after a negative good quality contrast-enhanced CT scan
Management
A spectrum of modalities is available for the management of abdominal trauma, ranging from clinical observation, through selective nonoperative management to damage control procedures. Interventional angiography is playing an increasing role in the management of solid organ injury; however, in the circumstances of physiological compromise, operative intervention remains the ‘gold standard’.
Indications for emergency surgical intervention include traumatic cardiac arrest, unexplained, especially progressive shock, a rigid silent abdomen, evisceration, evidence of intraperitoneal gas or diaphragmatic rupture and gunshot injury.


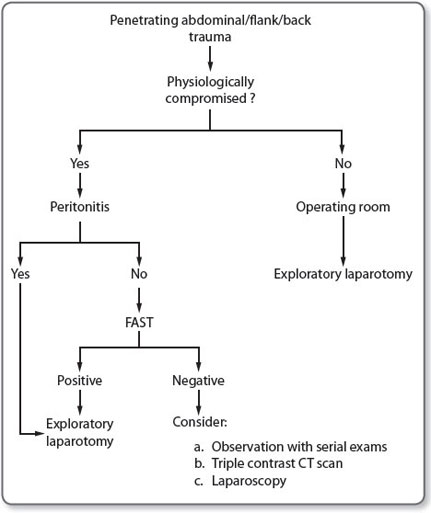
The main aim of damage control surgery, which is a component of damage control resuscitation, is to prevent the lethal triad of hypothermia, coagulopathy and acidosis from occurring, and if it has occurred to enable recovery to take place. Figures 1 and 2 illustrate potential algorithms for the management of blunt and penetrating injuries.
DCL is a physiological approach to the management of selected critically injured patients where the surgical technique is directed at minimising the metabolic insult, rather than restoring anatomic integrity. The aim is to prevent the development of, or to reverse, an established lethal triad of hypothermia, coagulopathy and acidosis. The priorities in DCL are to control haemorrhage and contamination. Manoeuvres to achieve these objectives include controlling major abdominal vascular structures by medial visceral rotations, supracoeliac aortic compression or clamping, preperitoneal pelvic packing, perihepatic packing, splenectomy, nephrectomy and bowel resection.
Laparoscopy
In the diagnosis of blunt abdominal injuries, most institutions prefer radiological imaging depending on local resources and experience. The potential benefit of diagnostic laparoscopy is that it can be both diagnostic and therapeutic. There are reported cases in the literature of laparoscopy being utilised with or without the presence of a pneumoperitoneum.
Complications
The complications of abdominal trauma can be divided into local and systemic responses to the insult (Table 1), and the time period after the insult at which they occur.5
Further reading
- Biffl WL, Moore EE. Management guidelines for penetrating abdominal trauma. Curr Opin Crit Care 2010;16:609–617.
- Hirshberg A. Chapter 27: Trauma laparotomy. In: Mattox KL, Moore EE, Feliciano DV. Trauma, 7th edn. New York: McGraw-Hill, 2013.
- Hoff WS, Holevar M, Nagy KK, et al. Practice management guidelines for the evaluation of blunt abdominal trauma: The EAST practice management guidelines work group. J Trauma 2002;53:602–615.
Related topics of interest
- Blunt and penetrating cardiac trauma (p. 45)
- Damage control resuscitation and surgery (p. 83)
- Genitourinary trauma (p. 114)
- Selective non-operative management of penetrating abdominal injuries (p. 254)