

- Anesthesia in Cataract Surgery – An UpdateAshok Garg
- No Anesthesia Clear Corneal PhacoemulsificationSuresh K Pandey, Amar Agarwal, Liliana Werner, Sunita Agarwal, Athiya Agarwal
- Corneal Endothelium and its Protection in PhacoemulsificationKeiki R Mehta
- Phacoemulsification with Cryoanalgesia—A New ApproachFrancisco J Gutiérrez Carmona
- No Anesthesia Cataract SurgeryTobias Neuhann
- PhakonitAmar Agarwal, Athiya Agarwal, Sunita Agarwal
- Phakonit with Acritec IOLSunita Agarwal, Athiya Agarwal, Amar Agarwal
- Endocapsular LensectomySteve Charles
- Phaco in Subluxated CataractsNishanth Patel, Vikas Lal, Amar Agarwal, Athiya Agarwal, Sunita Agarwal
- Update on Pediatric Cataract ManagementSuresh K Pandey, M Edward Wilson, David J Apple, Liliana Werner, Jagat Ram
- Favit – A Technique for Removing Dropped Nucleus during PhacoemulsificationAmar Agarwal, Sunita Agarwal, Athiya Agarwal, Suresh K Pandey, Clement K Chan
- Management of Dislocated Implants by the Vitreoretinal ApproachClement K Chan, Gerald RS Schultz
- Air Pump to Prevent SurgeSunita Agarwal, Amar Agarwal, Athiya Agarwal
- Trypan Blue in the Management of Mature CataractsAmar Agarwal, Athiya Agarwal, Sunita Agarwal
- My Personal Technique of Vertical Hubbing PhacoemulsificationKeiki R Mehta
- The Prevention of Complications and their Management in PhacoemulsificationKeiki R Mehta, Cyres Mehta
- Laser Phaco Cataract Surgery
- Corneal Topography in PhakonitAmar Agarwal, Soosan Jacob, Athiya Agarwal, Sunita Agarwal
- Attacking Childhood Cataract Blindness in the Economically Emerging CountriesSuresh K Pandey, M Edward Wilson, Jaya Thakur, Vidushi Sharma
- Update on Capsular Dye Enhanced Cataract SurgerySuresh K Pandey, Liliana Werner, David J Apple
- Update on Ophthalmic Viscosurgical DevicesSuresh K Pandey, Liliana Werner, David J Apple, Andrea M Izak, Vidushi Sharma
- Update on Twenty First Century Cataract—Intraocular Lens SurgerySuresh K Pandey, Liliana Werner, David J Apple, Andrea M Izak, Vidushi Sharma, Amar Agarwal
- Update on Posterior Capsule Opacification: Etiopathogenesis, Clinical Manifestations, Pharmacological and Surgical PreventionSuresh K Pandey, Liliana Werner, David J Apple, Andrea M Izak
- Pediatric Cataract—IOL Surgery: Past, Present and FutureSuresh K Pandey, M Edward Wilson, Liliana Werner, David J Apple, Vidushi Sharma
- Update on Delayed Postoperative Opacification of Rigid and Foldable, Intraocular LensesSuresh K Pandey, Liliana Werner, Andrea M Izak, David J Apple
- Corneal Topography in Cataract SurgeryAthiya Agarwal, Sunita Agarwal, Amar Agarwal, Nilesh Kanjani
- INTRODUCTION
- ANESTHESIA FOR CATARACT SURGERY
- GENERAL ANESTHESIA PROCEDURE
- METHODS OF ANESTHESIA
- ANESTHESIA FOR CHILDREN
- COMPLICATIONS OF GENERAL ANESTHESIA
- COMPLICATIONS OF RETROBULBAR INJECTION
- PERFORATION OF THE GLOBE
- RETINAL VASCULAR OBSTRUCTION
- SUBARACHNOID INJECTION
- PERIBULBAR (PERIOCULAR) TECHNIQUE
- TOPICAL ANESTHESIA
- HOW TO ACHIEVE SURFACE ANESTHESIA FOR INTRAOCULAR SURGERY
- CAN ONE CONVERT HALF WAY THROUGH SURGERY UNDER TOPICAL ANESTHESIA
- NO ANESTHESIA CATARACT SURGERY
INTRODUCTION
Anesthesia for Cataract Surgery has undergone tremendous changes and advancements in last century. In 1846 general anesthesia techniques were developed which were not found suitable and satisfactory for ophthalmic surgery. In 1884 Koller discovered surface anesthesia techniques using topical cocaine for cataract surgeries which found favor with the ophthalmologists. However due to significant complications and side effects of cocaine Herman Knopp in 1884 described retrobulbar injection as local anesthetic technique for ocular surgery. He used 4 percent cocaine solution injected into the orbital tissue close to posterior part of the globe to achieve adequate anesthesia but in the subsequent injections patients experienced pain. In 1914 Van Lint introduced orbicularis akinesia by local injection to supplement subconjunctival and topical anesthesia. However this technique found favor only after 1930 when procaine (Novocaine) a safer injectable agent made it feasible.
With the development of hyaluronidase as an additive to the local anesthetic solution Atkinson (1948) reported that large volumes could be injected with less orbital pressure and improved safety injections into the cone (retrobulbar) were recommended and gained rapid favor becoming anesthetic route of choice among ophthalmologists.
In Mid 1970s, Kelman introduced an alternative technique of local anesthesia for ocular surgery known as peribulbar injection. However till 1985 this new technique was not published in ophthalmic literature. In 1985 Davis and Mandel reported local anesthetic injection outside the cone into the posterior peribulbar space (periocular). Further modifications of both retrobulbar and periocular injection techniques were made by Bloomberg, Weiss and Deichaman, Hamilton and colleagues, whitsett, Murdoch Shriver and Coworkers. These modifications consisted of more anterior deposition of anesthetic solution with shorter needles and smaller dosages.
With the introduction of small incision cataract surgery, Phaco emulsification and other microsurgical procedures in ophthalmology, use of shorter needles with smaller dosages became more common. Fukasawa and Furata et al reintroduced subconjunctival anesthetic techniques. Fichman in 1992 first reported the use of topical tetracaine anesthesia for phacoemulsification and intraocular lens implantation starting an era of topical anesthesia in ocular sugery.
With the advent of many ocular anesthetic techniques in past two decades indicates the need for the development of an ideal anesthetic and 4technique for ocular surgery. Every existing technique has its own advantages and disadvantages. General anesthesia for cataract surgery is virtually out of favor with ophthalmologists. Retrobulbar anesthesia, periocular (peribulbar, subconjunctival, orbital and epidural) and topical anesthesia or a combination of peribulbar and topical are being used in present day ocular sugery. Now with the advent of below 1 mm incision technique, foldable and Rollable intraocular lenses, no anesthesia cataract surgery is becoming popular with increased frequency.
ANESTHESIA FOR CATARACT SURGERY
Cataract extraction may be performed under general anesthesia, local anesthesia or topical anesthesia, depending upon condition of patient cataract status and surgeon choice.
General Anesthesia
Usually for cataract surgery general anesthesia is not given. It is advisable only in highly anxious/nervous patient or when cataract surgery requires a long time for completion. Patients who are extremely apprehensive, deaf, mentally retarded, unstable or cannot communicate well with the surgeon are more suitable for general anesthesia. General anesthetic facilities with expert anesthetist are mandatory.
GENERAL ANESTHESIA PROCEDURE
Preoperative Preparation
A patient who is to be given a general anesthetic needs proper preoperative assessment and examination, preferably on the day before the anesthetic is to be administered, although preparation earlier on the day of surgery may be acceptable in many cases. Patients with cataracts are often elderly and not infrequently have other medical problems that must be considered before anesthesia is induced. These are—
Chronic (Obstructive) Respiratory Disease
These patients require more careful assessment. Their condition in severe cases can be adversely affected by anesthetic drugs and muscle relaxants. On the other hand, the inability to control obstructed respiration can lead to hazardous cataract surgery and a high incidence of failure. Preoperative preparation with antibiotics, bronchodilators, and physiotherapy often enable a sick patient to undergo a safe procedure with the benefit of a general anesthetic.
Cardiovascular Disease
Because many patients with cardiovascular disease will already be on diuretic treatment, preoperative assessment to detect and treat cardiac failure or hypokalemia is most important. The adequate control of hypertension is also an essential safety requirement, especially for the middle-aged.
Diabetes Mellitus
Diabetes mellitus is commonly found in those for whom cataract surgery is indicated. Preadmission stabilization is necessary, and when this is in doubt, a longer period of preoperative inpatient assessment and management is required to eliminate any ketonuria or gross hyperglycemia. Oral diabetic medication should be omitted on the day of surgery because the effects may persist for up to 24 hours. During surgery and throughout the early postoperative period, control is effected by using 5 percent glucose intravenously and insulin as required, as shown by the blood glucose levels. When the patient resumes normal oral intake postoperatively, the normal regimen is rapidly resumed.
Dystrophia Myotonica
These patients frequently require cataract surgery while they are quite young. They are particularly sensitive to anesthetic drugs and subject to prolonged respiratory depression. Suxamethonium is contraindicated; minimal doses of other drugs such as atracurium should be used.
Premedication
The aim of premedication is to allow a smooth induction of anesthesia. Most patients appreciate some sedation to alleviate the natural anxiety associated with any eye surgery. Opiates, however, are to be avoided because of their association with respiratory depression and postoperative vomiting. For the aged and anxious, oral premedication with diazepam, 5 to 10 mg, according to fitness and size or Lorazepam, 1 to 2 mg, works well. An antiemetic can then be administered during surgery.
For the younger and more robust, one can use a combination of pethidine, promethazine hydrochloride, and atropine. This is also a helpful combination for those with established respiratory disease.
Children over 1 year of age required sedation with trimeprazine tartrate syrup (3 to 4 mg per kg) 2 hours 5preoperatively. Younger babies should not require sedation. Atropine may be given either intramuscularly (0.2 to 0.6 mg 30 minutes preoperatively) or intravenously (0.015 to 0.02 mg with induction).
METHOD OF ANESTHESIA
Induction
A smooth induction avoids the problems of increased central nervous pressure with its consequent adverse effect on the intraocular pressure.
The drug most commonly used is thiopentone, which produces a rapid loss of consciousness. When it is used in doses of 3 to 4mg per kg, the onset is relatively slow in the elderly, who frequently have a slower circulation time. For the very frail, methohexitone is useful, producing less change in blood pressure. More recently disoprofol (Diprivan) has been found to be useful; it also has a rapid onset of action and induces little nausea and vomiting.
Intubation of the trachea with a non-kinking endotracheal tube is achieved with suxamethonium. Its use is associated with a transient rise in the intraocular pressure due to choroidal expansion. Ventilation with nitrous oxide and oxygen with 0.5 to 1 percent halothane is continued until the effects of the suxamethonium have subsided.
More recently techniques have been described for rapid sequence induction with vecuronium. These methods do not seem to be associated with a significant rise in the intraocular pressure and they avoid the problems of suxamethonium.
Maintenance
A nondepolarizing muscle relaxant is used throughout the surgical procedure, dosages depending on the size, age, and health of the patient. Available drugs include tubocurarine, which is inclined to produce hypotension (occasionally severe), pancuronium, and more recently vecuronium and atracurium. Vecuronium has been demonstrated to lower intraocular pressure. Because both atracurium and vecuronium act and subside rapidly, their effectiveness must be monitored regularly by a peripheral nerve stimulator.
Intermittent positive pressure ventilation is maintained by nitrous oxide, oxygen, and an anesthetic drug. One-half percent halothane has long been considered effective and also lowers the intraocular pressure. Other anesthetic drugs include enflurane (associated with more postoperative vomiting and restlessness, though less hypotension) and isoflurane. The latter does not appear to adversely affect the stability of the cardiovascular system. Its effect on intraocular pressure has not been reported.
Throughout the procedure the pulse, blood pressure, electrocardiographic record, and arterial oxygen saturation must be regularly monitored, along with the nerve stimulation needed for the nondepolarizing muscle relaxant being used. All ventilators should be fitted with an alarm to warn of malfunction.
Completion of recovery from anesthesia after cataract surgery must be as smooth as the induction, care being taken to avoid gagging, coughing, and of course vomiting. Modern ophthalmic sutures are good but not foolproof! The neuromuscular blockade is reversed with atropine and pros-tigmine. Gentle extubation is associated with careful pharyngeal suction. Patients are encouraged to resume normal activity as soon as the effects of the anesthetic drugs have worn off.
ANESTHESIA FOR CHILDREN
Adequate premedication and careful handling should insure a calm quiet child and allow a smooth induction. Because the cataract is dealt with by using a closed system, the surgical risks of a rise in intraocular pressure are not so severe. Inhalational anesthesia using nitrous oxide and oxygen with halothane is usually sufficient.
COMPLICATIONS OF GENERAL ANESTHESIA
The complications associated with a general anesthetic range from death to the less serious but irritating nuisances of protracted nausea and vomiting or sore throats. This chapter covers only those complications producing serious morbidity or mortality and those peculiar to the patient with eye disease.
- Hypoxemia (insufficient oxygen in the arterial blood to sustain life) is the most common cause of disaster, and failure to ventilate is the most common cause of hypoxemia. Unrecognized esophageal intubation, ventilator disconnection, and, most distressing of all, inability to ventilate after unconsciousness and paralysis have been obtained are all possible causes of failure to ventilate. Delivery of an inadequate oxygen concentration is a less common cause of hypoxemia. Most but not all of the foregoing are preventable with the monitoring and fail-safe devices available today, provided a competent anesthetist is monitoring the devices.
- Aspiration of gastric contents remains a common complication despite such preventive measures as 6overnight fasting, the use of metoclopramide to enhance gastric emptying, and rapid sequence induction with cricoid pressure in emergency procedures. The two life-threatening results of aspiration are airway obstruction from large food particles and chemical pneumonitis from acidic gastric contents.
- The two most serious cardiovascular complications, aside from cardiovascular collapse secondary to hypoxemia and acute anaphylaxis, are myocardial infarction and cerebrovascular accident. Surgery performed under general anesthesia within 3 months after a myocardial infarction carries a 40 percent incidence of repeat infraction. This figure decreases to about 10 percent at 6 months, after which the incidence is approximately the same as in the general population. All elective surgery is delayed until after 3 months, and a 6 month wait is encouraged unless poor visual acuity seriously limits activities.
- Renal and hepatic toxic effects from anesthetic drugs are seldom seen in our practice. Careful preanesthetic screening identifies all patients with renal and hepatic disease. Halothane, which gained notoriety because of its hepatotoxicity, especially when administered repeatedly, is not used in adults and is usually used for induction only in children. The metabolic byproducts of methoxyflurane and enflurane are inorganic fluorides, which can produce nephrogenic diabetes insipidus. We no longer use these drugs because so many of our patients have diabetes and severe renal disease in our population.
- Failure to resume respiration at the end of the surgery occurs often enough to merit mention. The most common causes are simple respiratory depression from the anesthetic drugs or narcotics, electrolyte disturbance (i.e., hypokalemia), hypothermia (particularly in infants), and the use of the combination of mycin antibiotics and nondepolarizing muscle relaxants. It also may occur after the administration of succinylcholine when there is a pseudocholinesterase deficiency. Respirations are main-tained until the cause is found and remedied.
Cardiovascular complications are the most commonly seen events in our practice. If diagnosed and treated properly, they need not result in a disaster. Hypertension is the most prevalent problem. The usual causes are apprehension, neo-synephrine eyedrops, pain, disten-ded bladder if mannitol was given, and autonomic nervous system imbalance secondary to the general anesthetic. Apprehension can be allayed with intravenous injections of 1 to 3 mg of Valium or 0.5 to 2 mg Zolpidem. Nitropaste applied to the skin and sublingual doses of nifedipine have proved invaluable, but an intravenous line should be in place before their use. Hypotension must be treated immediately and vigorously because it is tolerated less well than hypertension. Arrhythmias are the most frequent cause of cancellation on the day of surgery in the elderly patient with eye disease. The sudden onset of atrial fibrillation is the most common arrhythmia. An electrocardiographic monitor is mandatory for eye surgery.
Extrusion of ocular contents during administration of a general anesthetic is a serious complication in eye surgery. The entire anesthetic process is geared to minimize this possibility. Once the eye is opened, patients are kept deeply anesthetized or paralyzed with non-depolarizing relaxants to insure immobility.
Local Anesthesia
Local ocular anesthesia is the mainstay of cataract surgery. Local anesthesia minimises the risk of wound rupture a complication frequently associated with coughing during extubation and postoperative nausea and vomiting (in General Anesthesia) (Fig. 1.1). Generally the use of 1:1 mixture of 2 percent Xylocaine and 0.50 percent Bupivacaine along with adrenaline and Hyaluronidase in facial, retrobulbar and peribulbar blocks achieve rapid anesthesia, akinesia and post-operative analgesia for several hours.
Care should be taken to avoid intravascular injections of anesthetic agents because refractory cardiopulmonary arrest may result from an inadvertent intravenous or intra-arterial injections.


Fig. 1.1: Diagrammatic surface distribution of sensory nerves. Note branches derived from ophthalmic nerve (V1) and maxillary nerve (V2) a division of the trigeminal nerve
Many patients express pain of facial and retrobulbar injections so proper preoperative sedation and good rapport with the surgeon make them quite comfortable.
Following techniques are used for giving local anesthesia. These include:
Orbicularis Oculi Akinesia
Temporary paralysis of the orbicularis oculi muscle is essential before making section for the cataract surgery to prevent potential damage from squeezing of the lids. Following methods are used, for getting orbicularis oculi akinesia.
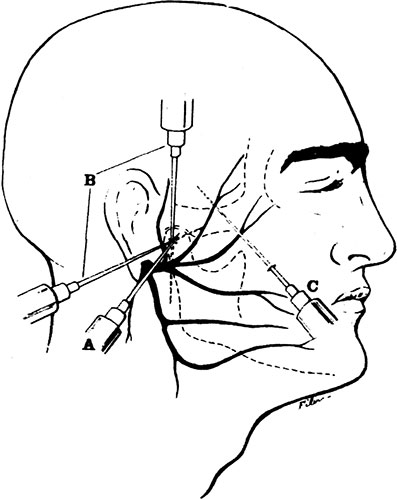
- O' Brien's technique Usually 10 ml of mixture of 2 percent Lidocaine solution (5 ml) and 0.5 percent bupivacaine solution (5 ml) with 1:100,000 epinephrine and 150 units of hyaluronidase are infiltrated for local anesthesia.O'Brien's method is the injection of above mentioned local anesthetic solution down to the periosteum covering the neck of the mandible where the temporofacial division of facial nerve passes forwards and upwards (Fig. 1.2). A 10 ml syringe with preferably No. 17 or 18 needle and 2.5 cm in length is used. The patient is asked to open his mouth and the position of the condyle and temporomandibular joint is located by the forefinger of the operators' left hand. After closing the jaw, the injection is given on a horizontal line through the junction of the upper and middle third of the distance between the zygoma and angle of the mandible. The needle should pass straight down the periosteum. 2–3 ml of local anesthetic solution is injected and after withdrawing the needle firm pressure and massage are applied. Paralysis of orbicularis oculi should occur normally within 7 minutes. The injection is unlikely to injure the external carotid artery which lies posterior and at a deeper level. However damage may be done to posterior facial vein and the transverse facial artery. Movement of jaws is sometime painful for few days after this injection.
- Van Lint's akinesia Van Lint's method is a better alternative. The injection of local anesthetic solution is made across the course of branches of the seventh nerve as they pass over the zygomatic bone (Fig. 1.3).In this technique a 5 cm in length and 25 gauge needle is passed through the wheal down to the periosteum of the zygomatic bone. The needle is than passed upward towards the temporal fossa without touching the periosteum (as it may be painful) and 4 ml of solution is injected and then forwards medially and downwards towards the infraorbital foramen to inject 2ml and downwards and backwards along the lower margin of the zygoma for 2.5 cm where 3 ml of solution is injected. It is essential to massage the infiltrated area with a gauze swab. Motor nerves are less susceptible than sensory nerves to a block with local anesthetic agents.The advantage of Van Lint's method is that it provides regional anesthesia as well as paralysis of the orbicularis muscle. After waiting for 5–7 minutes akinesia is tested by holding the eyelids open with a small swab on to a holder and asking the patient to close his eyelids. If slightest action is observed then injection may be repeated to obtain adequate akinesia.
- Atkinson block The needle enters through a skin wheal at the inferior border of the zygoma just inferior to the lateral orbital rim. The path of the needle is along the inferior edge of the zygomatic bone and then superiorly across the zygomatic arch, ending at the top of the ear.
- Spaeth block The Spaeth block avoids the inconsistencies of the O'Brien block as well as the postoperative discomfort caused by going through the parotid gland and entering the temporomandibular joint. An injection is made into the back of the mandibular condyle just below the ear, catching the facial nerve before it divides (Fig. 1.6). To locate the landmarks, the fingers are placed along the posterior border of the mandible as superiorly as possible. The needle is placed just anterior to the most superior finger. Bone should be reached shortly. If not, the needle is withdrawn and the position rechecked before a second attempt is made. After the bone is reached, the needle is pulled back slightly and suction is placed on the syringe to make sure that a vessel has not been punctured; 5 ml of anesthetic is then injected. Although rarely required, the needle can be redirected superiorly towards the outer canthus for 1.5 inches and an additional 5ml is injected. After 30 seconds, nearly complete facial palsy should be evident.
- Nadbath block An injection is made into the cavity between the mastoid process and the posterior border of the mandibular ramus. The skin is pierced, and a skin wheal is made 1 or 2 mm anterior to the mastoid process and inferior to the external auditory canal. A 12 mm, 26 gauge needle is used, with the injection of anesthetic extending from the skin wheal, passing through a taut membrane midway, to the full depth of the needle; 3 ml is injected (Fig. 1.7).The Nadbath block insures ease of performance, and there are few complaints relating to the original injection or subsequent pain in the jaw area. The most common side effect is a bitter taste as the parotid gland secretes the anesthetic. Other problems reported are dysphonia, swallowing difficulty, and respiratory distress. Judging from the fact that these complications are seen predominantly in very thin patients and most certainly are secondary to the diffusion of anesthetic to the jugular foramen, 1 cm deeper than the stylomastoid foramen, the length of the needle i.e., the depth of injection is critical.9Preexisting unilateral oropharyngeal or vocal cord dysfunction is a definite contraindication, as bilateral vocal cord paralysis could result. The Nadbath block should never be done bilaterally. If, after a unilateral Nadbath block, dysphonia or difficulty with swallowing or respiration occurs, lateral positioning will allow the paralyzed vocal cord to fall out of the way, clearing the airway.Proper administration of local anesthesia requires knowledge of orbital anatomy, various anesthetic techniques, and the properties of the drugs used. Prompt recognition of side effects and complications following injection results in the best possible patient care.
- Retro-ocular (retrobulbar) injection Anesthesia and akinesia of the eye are achieved by injecting a local anesthetic solution into the retrobulbar space within the muscle cone (Fig. 1.8).
- In this method patient is asked to look upwards and to the opposite side. A 3.5 cm length 23 gauge sharp edge round tipped needle is inserted in the quadrant between the inferior and the lateral rectus muscles and directed posteriorly until the resistance of orbital septum is encountered. After it has penetrated the orbit the needle is directed towards the apex of the orbit and advanced until it meets the resistance of the inter-muscular septum. When this structure is penetrated, the needle tip is in the retrobulbar space. About 3–4 ml of local anesthetic mixture solution is injected taking care, to minimize the needle movement to prevent possible vessels lacerations. Following the injection the globe should be intermittently compressed for several minutes for distributing the anesthetic solution and to ensure hemostasis. A properly placed retrobulbar injection is effective within seconds. It blocks all extraocular muscles except superior oblique muscle, affects the ciliary ganglion and anesthetize the entire globe (Fig. 1.9).






Gills-Loyd Modified Retrobulbar Block
Before the anesthetic is administered, the patient's vision is checked and the A scan is done. Then, prior to the first injection, 2 drops of proparacaine 0.5 percent are given topically. The eyes are either fixed in primary gaze or directed slightly superiorly, avoiding the superonasal position. With sharp 27 gauge needle, enter is effected at LE 4:00, RE 8:00, 5 mm medial to the lateral canthus. The needle is inserted parallel to the optic nerve. A preretrobulbar injection of 1.5ml of pH adjusted Xylocaine is administered subconjunctivally. After 30 seconds, a 5 ml retrobulbar injection of pH adjusted bupivacaine and hyaluronidase is injected with a 25 gauge, 1¼ inch needle. After 8 to 9 minutes, the eye is checked for akinesia.

Fig. 1.9: Needle positions for retrobulbar and peribulbar anesthesia (frontal view)(Courtesy: Ciba Geigy clinical symposia)
A 1 to 3 ml supplemental injection of full strength anesthetic is given as needed to complete the block. 1.0 ml bolus is administered subdermally into the inferolateral lid to anesthetize the distal branches of the seventh cranial nerve; this technique does not require a total seventh nerve block. Next 0.5 ml of cefazole is injected subconjunctivally, and gentle eye compression is administered for 30 to 60 minutes with a Super Pinky Decompressor prior to surgery.
COMPLICATIONS OF RETROBULBAR INJECTION
A number of complications can occur as a result of retrobulbar injection, among them retrobulbar hemorrhage, perforation of the globe, retinal vascular obstruction, and subarachnoid injection.
Retrobulbar Hemorrhage
Retrobulbar hemorrhage probably occurs in 1 to 5 percent of the cases. It seems to occur less frequently if a blunt tipped needle is used, but this has not been demonstrated in any controlled study.
Retrobulbar bleeding may occur at a number of sites. The four vortex veins leave the globe approximately 4 mm posterior to the equator and could well be subjected to the shearing forces of an inserted needle, as could the central retinal or ophthalmic vein. An arterial source of bleeding must be postulated to explain severe hemorrhages that produce the rapid onset of proptosis, hemorrhage, chemosis, and immobility of the globe. The posterior ciliary arteries supplying the choroid, the central retinal artery, and other ophthalmic artery branches are all subject to damage. Even the ophthalmic artery can be reached in the area of the optic foramen with a 1½ inch needle.
Most instances of retrobulbar hemorrhage resolve without complication, but should a complication arise, particularly during elective surgery, it is prudent to postpone the operation for at least 3 to 4 weeks and then consider general anesthesia if the patient can tolerate it.
Even when general anesthesia is employed, severe positive pressure can develop in an open eye if the operation is performed within several days after the hemorrhage.
Vision may be permanently decreased following a retrobulbar hemorrhage. This probably occurs as a result of closure of the central retinal artery or damage to the smaller vessels that supply the retrobulbar optic nerve.
If examination reveals that the central retinal artery has closed because of increased intraorbital and intraocular pressures, a lateral canthotomy should be performed. Other possible therapeutic modalities include anterior chamber paracentesis and orbital decompression. Prior of decompression of the orbit, computed tomographic scanning of the region should be undertaken to help localize the blood and rule out the possibility of bleeding within the optic nerve sheath, which also might have to be decompressed.
PERFORATION OF THE GLOBE
This is another sight threatening complications of ophthalmic surgery with retrobulbar anesthesia. Highly myopic eyes are particularly suscepticle to this complication because of their long axial lengths. General anesthesia should be considered as an alternative in such eyes.
The scleral perforation should be repaired as soon as possible. Cryopexy or laser treatment of the break(s) may suffice, although vitreous traction that develops along the needle tract through the vitreous gel is better negated by a scleral buckling procedure. If the fundus view is obscured by vitreous hemorrhage, a pars plana vitrectomy is warranted to visualize the break(s). Although double scleral perforations probably have a worse prognosis than the single variant, the latter also can be devastating. I have seen one case in which the retina in the posterior pole was partially aspirated through the needle following a scleral perforation anterior to the equator.11
Inadvertent injection of lidocaine into the vitreous cavity appears to be tolerated by the globe. However, it can cause an extreme elevation of the intraocular pressure and rapid opacification of the cornea.
RETINAL VASCULAR OBSTRUCTION
Retinal vascular obstruction has been reported after retrobulbar anesthesia. The most common types are central retinal artery obstruction and combined central retinal artery-central retinal vein obstructions. Central retinal artery obstruction seems to occur more commonly in conjunction with diseases that affect the retinal vasculature, such as diabetes mellitus and sickling hemoglobinopathies. Nevertheless, it also can be seen in people with good health. Fortunately, the condition more often than not reverses spontaneously and the central retinal artery reperfuses within several hours. The causes are uncertain, but spasm of the artery, direct trauma to the vessel from the needle, and external compression by blood or an injected solution are possible mechanisms that could cause obstruction. Ophthalmic artery obstruction also can be induced, possibly by injection and subsequent compression within the optic foramen.
Therapy is directed towards relieving the obstruction and keeping the retina viable. Anterior chamber paracentesis may help, the aim being to lower the intraocular pressure and decrease the resistance to blood through the central retinal artery. Although paracentesis widens vessels narrowed by artery obstruction, fluorescein angiography shows that the filling occurs in a retrograde fashion, via the retinal veins. Hence its value is questionable.
Combined obstruction of the central retinal artery and central retinal vein is a much more serious complication. Ophthalmoscopically a cherry-red spot is seen, as well as numerous intraretinal hemorrhages and dilated retinal veins. The Mechanisms of obstruction include direct trauma to the central retinal vessels from the needle or compression from blood or fluid injected into the nerve sheath. Blood within a dilated optic nerve sheath has been demonstrated in these cases.
The visual prognosis of these eyes is generally grim. Computed tomography of the retrobulbar optic nerve may be used to determine whether a nerve sheath hemorrhage is present. If an optic nerve sheath hematoma is discovered, decompression of the nerve sheath may be of limited benefit.
Neovascularization of the iris may develop after combined central retinal artery-central retinal vein obstruction. If the anterior chamber angle is not yet closed by a fibrovascular membrane, aggressive, full scatter panretinal photocoagulation treatment should be administered in an attempt to prevent neovascular glaucoma.
Injecting with the eye in the primary position may help prevent this complication. In contrast, injecting with the eye looking up and in, places the optic nerve and central retinal vessels more in the pathway of the needle and thus probably should be avoided.
Multiple emboli with the retinal arterial system have caused vascular obstruction following retrobulbar corticosteroid injection. No therapy is available for this visually devastating complication which likely results from injection into the central retinal or ophthalmic artery. In theory, the use of a needle shorter than 1½ inches may help to prevent the complication, as can having the patient gaze in the primary position during the injection.
SUBARACHNOID INJECTION
Among the most recently recognized complications of retrobulbar, anesthesia, inadvertent injection into the subarachnoid space may be the most serious. The subarachnoid space extends around the retrobulbar optic nerve up to the globe and can be violated with a retrobulbar needle at any point along its course.
Optic atrophy and blindness have also been reported following retrobulbar blocks but they are fortunately rare. Due to these potential complications retro-ocular injection is out of favor with eye surgeon worldwide.
PERIBULBAR (PERIOCULAR) TECHNIQUE
Since the exit of retrobulbar akinesia, peribulbar akinesia is considered a safe and effective technique of local anesthesia for cataract surgery. It is method of choice with eye surgeons for giving local anesthesia in cataract surgery. As the name indicates, peribulbar anesthesia is a technique in which a local anesthetic is injected into peribulbar space and is not aimed at blocking a perticular nerve.
Technique
Periocular anesthesia is administered at two site in lower temporal quadrant and nasal to caruncle (Fig. 1.10).
The required local anesthetics are Lidocaine 1 percent and Bupivacaine 0.75 percent with hyaluronidase. Bupivacaine is preferred as it is a longer acting anesthetic agent which can provide prolonged anesthesia and analgesia.
In the first stage, injection of 0.5 cc of 1 percent lidocaine with a 26 gauge needle is done under the skin at about 1 cm away from the lateral canthus in the lower lid, along the orbital rim.12

Fig. 1.10: Needle positions for peribulbar and retrobulbar akinesia(Courtesy: Ciba Geigy clinical symposia)
The same needle is passed deeper to inject 0.5 cc of lidocaine into the orbicularis muscle and 1.0 cc into the muscle sheath. A second injection is done in the similar fashion in the upper eyelid just below the supraorbital notch. Pressure is applied at both for a minute using gauze pieces.
In the second stage, combination of 6.0 ml of 0.75 percent bupivacaine, 3 ml of 1 percent lidocaine and 0.25 cc of hyaluronidase is filled into a 10 ml Disposable syringe fitted with a, 1–1/4 inch 23 gauge, hypodermic needle. The needle is first introduced deep into the orbit through the anesthetized site in the lower eyelid. One ml is injected just beneath the orbicularis muscle and then the needle is advanced upto the equator of the globe to inject 2 to 3 ml of the solution. The same procedure is followed in the upper nasal quadrant through the preanesthetised site to inject 1ml and another 1 ml may be injected around superior orbital fissure, by deeper penetration.
At the end of the procedure, fullness of the lids is noted due to the volume of the injected solution. Firm pressure with the flat of the hand is applied over the globe and is maintained for a minute. Then, before surgery, any pressure device as per the surgeon's choice like Honan's balloon, super pinky ball, balance weight or simple pad-bandage is applied for 20 to 30 minutes, to achieve the desire response of hypotony.
The efficacy of the anesthesia is evaluated after about 10 minutes of injection and if inadequate, 2 to 4 ml more can be injected. In case of persistent inferior or lateral movement injection lower temporal quadrant and in case of persistent movements upwards of nasally, the upper quadrant could be infiltrated in the same fashion.
Hyaluronidase is essential as it helps in the spread of the drug. Otherwise, there are chances of the eye being proptosed due to high orbital pressure induced by the large quantity of the fluid injected.
Single injection of 5 to 6 ml of anesthetic mixture injected from any site posterior to equator of the globe also achieves same results. For convenience, however, it may be done through lower lid the junction of lateral and middle one third, along the floor of the orbit.
Adequacy of akinesia is determined by the absence of ocular movements in all directions.
This technique is certainly better than retro-ocular technique and has least complications.
Advantages
The advantages reported are:
- The injection is done outside the muscle cone and so, the inherent complications of passing the needle into the muscle cone is completely eliminated.
- Since the needle is constantly kept parallel to the bony orbit, it avoids injury to globe and entry of anesthetic agents into the eyeball.
- It causes less pain on injection.
- The procedure is easier and can be performed without causing damage to vital structures.
- It does not reduce vision on table.
- No facial block is required.
Drawback
The possible drawbacks of this procedure are:
- Chemosis of conjunctiva.
- Delayed onset of anesthetic effect and
- Potential risk of orbital hemorrhage. Though it occurs rarely, the magnitude of the problem is comparable to retrobulbar hemorrhage and necessitates postponement of surgery.
Mechanism
The exact mechanism is not known but this procedure may best be described as ‘Infiltration anesthesia' where nerve endings in all tissues in the area of injection get anesthetised.
Peribulbar anesthesia is a safe and reliable technique for achieving akinesia and anesthesia of the globe. In case of inadequate anesthesia, repeat injections in the similar manner can be safely used to achieve the purpose.
Superior Rectus Injection
The induction of temporary paralysis of the superior rectus muscle is essential for any intraocular operation where the surgical field is upper half of the eye. This injection also affects the action of levator palpabrae superioris.
In this injection patient is asked to look down. The upper lid is retracted and 2.5 cm long needle is passed into Tenon's capsule at the temporal edge of the superior rectus muscle. The needle is directed posteromedially and about 1 ml of anesthetic mixture of 2 percent Xylocaine is injected around the muscle belly behind the equator. This injection can also be made through the skin of the upper orbital sulcus.
Tenon's Capsule Injection
The injection of anesthetic mixture can be given into Tenon's capsule around the upper half of the eyeball and into the belly of superior rectus muscle. It is considered safer than the retro-ocular injection across the post-ganglionic fibers of the ciliary body and may be effective in inducing extraocular muscle akinesia.


Parabulbar (Flush) Akinesia
Parabulbar (flush) administration is a new route for local anesthesia which is highly useful, safe, effective and technically easier (Figs 1.11 and 1.12). This method consists of a limbal sub-tenon administration of Retrobulbar anesthesia using a blunt irrigating cannula. This technique can be used for anterior and posterior segment surgery.14
TOPICAL ANESTHESIA
Since the advent of retrobulbar and peribulbar techniques in the early part of this century, both procedures are mainstay of local anesthesia for intraocular surgery till today. They do carry the risk of perforation of globe, optic nerve and the inadvertent injection of anesthetic at wrong places.
These accidents are mainly due to:
- Carelessness on the part of ophthalmologist who considers the procedures lightly and occurs more often with senior eye surgeons.
- Using long needles for these techniques endangers the perforation of globe, piercing the optic nerve and entering crowded retrobulbar space and even touching the intracranial space on forceful injection of copious amounts.
- Anesthetics given through local injection with little knowledge of anatomy of this area.
- Retrobulbar hemorrhage with its adverse effects on nerve and globe is very common complication of this technique.
- Injury caused by perforation of globe can lead to hole formation, retinal detachment, vitreous hemorrhage and central and branch vein occlusions.
To overcome all these practical difficulties use of topical anesthesia in intraocular surgery has been widely suggested and used at an International ophthalmic level. Topical anesthesia meaning topical application of 4 percent Xylocaine or 0.5-0.75 percent proparacaine one drop 3–4 times at regular intervals) in the eye has become increasingly popular and accepted. In present day high tech intraocular surgery specially phaco surgery topical anesthesia is the anesthesia of choice with the eye surgeons worldwide.
Indications to use Topical Anesthesia
- Its indications in intraocular surgery are mainly when performing phacoemulsification and IOL implantation through a clear corneal tunnel and corneoscleral incisions.
- Topical anesthesia is ideally suited for small incision and stitchless cataract surgery. However, it is not a advocated to perform standard/manual extracapsular cataract extraction and IOL implantation.
- Proper selection of patient is of great importance in this technique. It is important to have a patient who will comply with the instructions given during surgery.
- Patients who are non-cooperative, hard of hearing, with language problem and anxious patients are poor candidates for surgery under topical anesthesia. Capsulorrhexis requires the maximum cooperation of the patient.
- Intraocular surgery likely to be problematic in patients with rigid small pupils responding poorly to dilating drops and eyes with lenticular subluxation and high grade nuclear sclerosis are relative contraindications for topical anesthesia.
- Eye surgeon operating with topical anesthesia should be proficient and experienced at phacoemulsification.
- This procedure requires the use of foldable IOL either as a silicone lens or an acrylic lens. This is essential because corneal tunnel suture lens incision cannot be larger then 3.5mm. Otherwise corneal complications may arise and the incision would not be self-sealing.
HOW TO ACHIEVE SURFACE ANESTHESIA FOR INTRAOCULAR SURGERY
Generally 3 applications of 4 percent Xylocaine or 0.4 percent Benoxinate HCL or 0.5-0.75 percent proparacaine 10 minutes apart starting 30 minutes before surgery are recommended. A drop is thereafter instilled prior to the incision. 1 CC of 4 percent Xylocaine or 0.4 percent Benoxinate HCI or 0.5-0.75 proparacaine (from fresh vail) is drawn into sterile disposable syringe and OT staff person is asked to instil a few drops of the same prior to cauterisation of bleeders and if required during surgery conjunctival anesthesia is used (pinpoint and mini pinpoint surface anesthesia)
Apart from giving topical anesthesia one has to give systemic analgesia. Besides it, surgeon should have a commanding hypnotic voice (vocal local anesthesia).
- Most surgeons doing corneal tunnel incision under topical anesthesia prefer to do it from temporal side.
CAN ONE CONVERT HALF WAY THROUGH SURGERY UNDER TOPICAL ANESTHESIA
Intraoperative conversion from topical to peribulbar anesthesia can definitely be achieved if surgical situation. Warrants it. Since corneal tunnel incision is sutureless and self-healing a peribulbar injection can safely be given during the surgery.
Advantages of Topical Anesthesia
- It prevents the well-known complications of retrobulbar and peribulbar injections as mentioned in the early part of this chapter.
- It lessens the time of operating room use thereby lowering costs.
- There is no immediate postoperative ptosis as seen in retrobulbar or peribulbar and Van Lint, O' Brien infiltrations lasts for 6–8 hours due to temporary akinesia of the lids.
- With topical anesthesia photon laser intraocular surgery can be OPD procedure.
- In practice we have seen the anxiety of patients to peribulbar and retrobulbar injections prior to surgery. With topical anesthesia this problem is over and patient compliance will be better during intraoperative period.
- The need of qualified anesthesiologist is over in operation theater during the operation as a number of ophthalmologists have been seen to prefer anesthesiologist by their side for local anesthesia (retrobulbar and peribulbar anesthesia).
- No risk of postponement of intraocular surgery as seen in cases of retrobulbar hemorrhage.
Again its main advantage is that it provides for immediate postoperative visual recovery.
Disadvantages of Topical Anesthesia
- Only a highly experienced surgeon can operate with topical anesthesia. The eye can move which makes the operation more difficult. If the eye movement occurs when capsulorrhexis is being done, an undesirable capsular tear may take place leading to failure of this important step of the operation.
- The chances of intraoperative complications with topical anesthesia can be high if the surgeon is not highly skilled. If such complications arise surgeon should be ready to convert to other methods of local anesthesia during the intraoperative stage, because topical anesthesia along may not be adequate to handle intraoperative complications. Surgeon should be of cool temperament who can handle such a situation without anxiety.
- Topical anesthesia is not indicated in all patients specially in anxious stressed patients, people with hearing difficulties, children and very young patients.
- As in our country a large number of patients come from rural areas who are illiterate and poor. Their compliance remains very poor and they do not respond adequately to the command during surgery with topical anesthesia.
- The presence of very opaque cataract is a contraindication to the use of topical anesthesia. This is because surgeon depends on the patient ability to visually concentrate on the operating microscope light in order to avoid eye movement during the operation. Patients, who are not able to fix the eyes, may lead to complications.
- Some patients may feel pain during surgery with topical anesthesia. One patient observed a lot more pain and felt as if a sword was being used to cut him up. The pain continued postoperatively for quite sometime.
- In principle, adequate selection of patients is fundamental when considering the use of topical anesthesia.
In spite of these hurdles topical anesthesia will be a safe and common technique for local anesthesia during intraocular surgery in the near future.
NO ANESTHESIA CATARACT SURGERY
This is the latest technique of cataract surgery in which no anesthesia is required (whether local or topical). Neither the topical or intracameral anesthetics agents are used. This techniques is devised by Dr Amar Agarwal (India) and has been acclaimed and accepted worldwide and is being used routinely in phacoemulsification surgery.
FURTHER READING
- Arora R et al. Peribulbar anesthesia, J Cataract Ref Surg 1991; 17:506–08.
- Bloomberg L. Administration of periocular anesthesia. J Cataract Ref Surg 1986; 12: 677–79
- Bloomberg L. Anterior peribulbar anesthesia. J Cataract Ref Surg 1991; 17: 508–11.
- Davis DB. Posterior peribulbar anesthesia. J Cataract Ref Surg 1986; 12: 182–84.
- Fichman RA: Topical anesthesia, Slack Sanders DR, 1993; 1661–72.
- Furuta M et al. Limbal anesthesia for cataract surgery. Ophthalmic Surg 1990; 21: 22–25.
- Garg A. Topical anesthesia: Current trends in ophthalmology. Jaypee Brothers Medical Publishers (P) Ltd., New Delhi: 1997; 1–5.
- Hay A et al. Needle perforation of the globe during retrobulbar and peribulbar injection. Ophthalmology 1991; 98: 1017–24.
- Kimble JA et al. Globe perforation from peribulbar injection. Arch Ophthalmol 1987; 105:749.
- Shriver PA et al. Effectiveness of retrobulbar and peribulbar anesthesia. J Cataract Ref Surg 1992; 18: 162–65.
- Zahl K et al. Ophthalmol Clin North Am. WB Saunders, Philadelphia: 1990.