



Melania Cigales
Jairo Hoyos-Chacón
INTRODUCTION
Astigmatism is a refractive error that occurs when the optical system does not have the same refractive power at all its meridians. Although it may originate in the crystalline lens, astigmatism is mostly corneal. Corneal astigmatism occurs when the curvatures of the principal meridians of the cornea at right angles to each other differ (one is steep, the other flat). Astigmatism is usually regular, which means that the principal meridians are perpendicular to each other (Fig. 1.1). Irregular astigmatism occurs when the principal meridians are not perpendicular to each other or when there are other asymmetries that are not correctable with conventional lenses or refractive surgery. This may occur in corneal pathologies such as keratoconus or pellucid marginal degeneration (Fig. 1.2). Astigmatism is described as with-the-rule, when the vertical meridian is the steepest and against-the-rule, when the meridian showing most curvature is the horizontal meridian (Fig. 1.3). Astigmatism with axes more than 30° from the horizontal and vertical meridians is referred to as oblique astigmatism.
Astigmatism is generally congenital and hereditary, developing at an early age and not usually advancing thereafter. When confronted with a late-onset progressive astigmatism, we should consider the possibility of a corneal pathology such as keratoconus or pellucid marginal degeneration.3



Fig. 1.3: Regular astigmatism with-the-rule astigmatism (top) and against-the-rule astigmatism (bottom)
A form of astigmatism that is currently acquiring greater significance, is post-surgery astigmatism, especially associated with cataract surgery and keratoplasty.
We should differentiate between refractive astigmatism (obtained through the subjective examination of the patient) and corneal astigmatism (which is measured at the anterior surface of the cornea using the keratometer or topographer). Refractive astigmatism is essentially determined by the anterior curvature of the cornea; and in smaller measure, by its posterior curvature and by that of the crystalline lens. Hence, refractive astigmatism does not fully coincide with corneal astigmatism.5
CLASSIFICATION
When a ray of light from a point image crosses an astigmatic cornea, it divides into two focal lines that are projected in front and/or behind the retina. Depending on where these focal lines are projected with respect to the retina, we can classify astigmatism as myopic, hyperopic or mixed. To understand the basis of an astigmatic ablation, we need to be clear about this classification. Figure 1.1 shows the typical topography of a corneal astigmatism of 4.5 diopters (D), where the Sim K (simulated keratoscopic reading) indicates that the steepest meridian (dioptric power 45.0 D) is at 90° and the flattest meridian (dioptric power 40.5 D) is at 180°. Using this as an example, we will explain the different astigmatism classes.
Myopic Astigmatism
Simple Myopic Astigmatism
In simple myopic astigmatism, one of the focal lines is projected in front of the retina and the other is brought to focus on the retina. Following the example described above, Figures 1.4A and B show a simple myopic astigmatism of refraction: Plano −4.5 × 180°. In this case, the steep meridian (45.0 D × 90°) has a myopic power of −4.5 D and projects an image in front of the retina; and the flat meridian (40.5 D × 180°) is emmetropic and brings an image to focus on the retina.6

To treat this astigmatism, we need to flatten the steep axis (45.0 × 90°) without modifying the flat meridian (40.5 D × 180°). To do this, the ablation is performed with a negative cylinder of −4.5 × 180° (Fig. 1.5). Ablation is started in the center of the cornea by carving a cylinder that opens onto the steep meridian such that this axis is flattened until it becomes emmetropic.

Compound Myopic Astigmatism
In compound myopic astigmatism, both focal lines are projected in front of the retina. Following the example, Figures 1.6A and B shows a compound myopic astigmatism of refraction −2 −4.5 × 180°.8

In this case, the steep meridian (45.0 D × 90°) has a myopic power of −6.5 D and projects an image in front of the retina; and the flat meridian (40.5 D × 180°) has a myopic power of −2.0 D and also projects an image in front of the retina.
To treat this astigmatism we need to flatten both meridians, but one more than the other. For this, we ablate with a negative cylinder of −4.5 × 180° to flatten the steepest axis (45.0 × 90°) from −6.5 to −2.0 D. Then, on the spherical cornea obtained, we undertake a central spherical ablation of −2.0 D that flattens both axes until emmetropy (Fig. 1.7).

Hyperopic Astigmatism
Simple Hyperopic Astigmatism
In simple hyperopic astigmatism, one focal line is projected behind the retina and the other is brought to focus on the retina. According to the example, Figures 1.8A and B show a simple hyperopic astigmatism of refraction: +4.5 −4.5 × 180°, or its transposition: Plano +4.5 × 90° (see Appendix I—cylinder transposition). In this case, the flat meridian (40.5 D × 180°) has a hyperopic power of +4.5 D and projects behind the retina; and the steep meridian (45.0 D × 90°) acts emmetropically and projects focal line on the retina.
To treat this astigmatism, we need to steepen the flat axis (40.5 D × 180°) without modifying the steep axis (45.0 × 90°), which is emmetropic. To do this we ablate using a positive cylinder of +4.5 × 90° (Fig. 1.9). Ablation is performed along the periphery of the flattest meridian, steepening it until it becomes emmetropic.
Compound Hyperopic Astigmatism
In compound hyperopic astigmatism, both focal lines are projected behind the retina. Following the example, Figures 1.10A and B show a compound hyperopic astigmatism of refraction: +6 −4.5 × 180°, or its transposition: +1.5 +4.5 × 90° (see Appendix I—cylinder transposition).11


In this case, the steep meridian (45.0 D × 90°) has a hyperopic power of +1.5 D and projects behind the retina; and the flat meridian (40.5 D × 180°) is of hyperopic power +6.0 D and also projects images behind the retina.
To treat this type of astigmatism, we need to steepen both meridians, but one more than the other. To do this, we perform the ablation using a positive cylinder of +4.5 × 90° to steepen the flat axis (40.5 × 180°) from +6.0 to +1.5 D; and, once the cornea is spherical, we undertake a spherical peripheral ablation of +1.5 D, which steepens both axes until they become emmetropic (Fig. 1.11).13
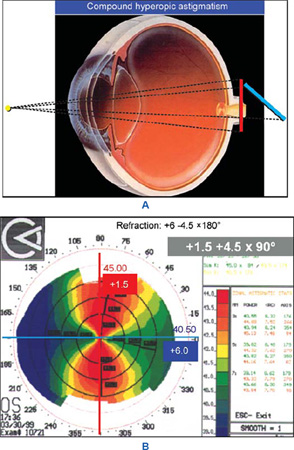

Fig. 1.11: Ablation for compound hyperopic astigmatism using a positive cylinder and a hyperopic sphere
Mixed Astigmatism
In mixed astigmatism, one focal line is projected in front of the retina and the other is projected behind the retina. Following the example, Figures 1.12A and B show a mixed astigmatism of refraction: +2 −4.5 × 180°. In this case, the steep meridian (45.0 D × 90°) has a myopic power of −2.5 D and projects an image in front of the retina; and the flat meridian (40.5 D × 180°) is hyperopic (+2.0 D) and projects an image behind the retina.
To treat this astigmatism, we need to flatten the steep axis (45.0 × 90°), which is myopic of −2.5 D and steepen the flat hyperopic axis of +2 D (40.5 D × 180°).15

This may be done according to several treatment models: negative cylinder with positive sphere, positive cylinder with negative sphere or bitoric treatment, in which positive and negative cylinders are combined. The bitoric treatment is the most physiological to treat mixed astigmatism and results in the removal of least tissue. In this case, for bitoric treatment we perform a negative cylinder ablation of −2.5 × 180° to flatten the steepest axis (45.0 × 90°) and a positive cylinder of +2 × 90° to steepen the flat axis (40.5 × 180°) (Fig. 1.13).

Fig. 1.13: Ablation for mixed astigmatism achieved through bitoric treatment, in which positive and negative cylinders are combined
SUGGESTED READING
- Atchison DA, Smith G. Refractive anomalies. In Optics of the Human Eye. Elsevier Science Limited, 2002;57–66.
- Carceles JA, Montoya MV, Salinas EM, Verdu AJ. Defectos de refraccion. In Solans T (Ed): Refraccion Ocular y Baja Vision. Spanish Ophthalmology Society Book, 2003;43–74.
- Cigales M, Hoyos JE, Hoyos-Chacon J. LASIK in mixed astigmatism. In Benjamin F Boyd, Sunita Agarwal, Athiya Agarwal, Amar Agarwal (Eds): LASIK and Beyond LASIK—Wavefront Analysis and Customized Ablation. Highlights of Ophthalmology Int'l, 2001;187–93.