

OCULAR HISTORY
Trauma
Blunt Trauma
Blunt trauma may result in a fine tremor of the lens on eye movement (phacodonesis) due to zonular dehiscence (Fig. 1.1). In this situation a capsular tension ring may be required to stabilize the lens after hydrodissection. Higher settings of vacuum and power should be used to reduce the stress on the zonules.


Penetrating Trauma
Penetrating trauma may be associated with damage to the posterior capsule with an increased risk of a dropped nucleus during surgery.3
Refraction
High Myopia
High myopia, especially when associated with a posterior staphyloma, carries an increased risk of globe perforation during peribulbar anaesthesia. A highly myopic eye may also have an unstable anterior chamber and mobile posterior capsule. The more myopic eye may also be amblyopic.
Hypermetropia
Very hypermetropic eyes may require two intraocular lens (IOLs) implants one on top of the other (piggyback).
MEDICAL HISTORY
Diabetes
Diabetic Retinopathy
Diabetic retinopathy should be treated prior to cataract surgery, if possible (Fig. 1.2). Proliferative diabetic retinopathy and macular oedema may develop or worsen following cataract surgery.
Other Problems
Other problems in diabetic patients include small pupils, pigment dispersion, delayed wound healing, fibrinous uveitis and an increased risk of infection.

Other Considerations
Hypertension
Hypertension may rarely increase the risk of suprachoroidal (expulsive) haemorrhage.
Anticoagulants
Warfarin (INR should be less than 2.5) can be stopped three days prior to surgery in consultation with a 5haematologist. If possible, topical anaesthesia should be used to decrease the risk of bleeding.
EXAMINATION
Grading of Nucleus
One of the important factors to be considered for successful cataract surgery involves judging the hardness of the nucleus. This is particularly important for surgical training, as appropriately chosen cases reduce the risk of complications. The colour of the nucleus depends on the age of the cataract and varies from transparent–grey–yellow–amber–brown–black. The latter occupies most of the lens and is the hardest. The hardness of a mature cataract is difficult to judge because the nucleus is not visible. An important consideration is the duration of visual loss; the longer the visual loss, the harder the nucleus.
Grade 1 (Fig. 1.3)
- Soft
- Transparent
- Grey.
Example: Recent cortical or subcapsular opacity.
Grade 2
- Slightly hard
- Grey or yellowish-grey.
Example: Presenile cataract.

Grade 3 (Fig. 1.4)
- Moderately hard
- Yellow with tinges of grey.
Example: Typical senile cataract.

Grade 4
- Hard
- Yellow-amber.
Example: Cataract in an elderly patient.
Grade 5 (Fig. 1.5)
- Very hard
- Brown or amber-black.

External Features
Deep Set Eyes and Small Palpebral Fissures
Deep set eyes and small palpebral fissures are indications for a temporal incision to enhance surgical access and maneuvering of the phaco tip without being hampered by the superior orbital rim (Fig. 1.6). Annoying reflections 8from flooding by fluid can be eliminated by asking the patient to turn the head into the appropriate direction.

Hearing Aids
Hearing aids must be removed or protected from soaking during surgery (Fig. 1.7).
Staphylococcal Blepharitis
Staphylococcal blepharitis is a risk factor for postoperative endophthalmitis and must be treated prior to surgery (Fig. 1.8).


Infected Contralateral Socket
Infected contralateral socket is also a risk factor for postoperative endophthalmitis (Fig. 1.9).

Chronic Dacryocystitis
Chronic dacryocystitis should be treated before the cataract surgery (Fig. 1.10).

Cornea
Pannus and location of corneal opacities should be noted so that the incision may be planned accordingly (Fig. 1.11). A compromised endothelium (Fig. 1.12) should be protected by the judicious use of balanced salt solution plus (BSS Plus) and Viscoat.

Pupil Size
A small pupil may result in an inadequate capsulorrhexis (rhexis) with increased risk of damage to the edge of the rhexis during manipulation of the nucleus. Other problems include incomplete cortical clean-up so that small nuclear fragments may be left behind the iris because of poor visibility (Fig. 1.13). Management of a small pupil may involve one of the following:


- Injection of a viscoelastic between the iris and lens may break weak posterior synechiae.
- Blunt dissection to break strong synechiae.
Anterior Chamber Depth
Shallow Anterior Chamber
A shallow anterior chamber is associated with overall reduction of the safe zone (Fig. 1.18). Endothelial cell loss is potentially higher from surgical trauma so that the endothelium must be protected with viscoelastics. The risk of iris trauma is increased because the angle at which the instruments are inserted is more critical than in an eye with a deeper anterior chamber (Fig. 1.19).
Very Deep Anterior Chamber
A very deep anterior chamber predisposes to trauma at the site of incision because the phaco tip must be nearly vertical when removing the nucleus. Manipulation of the nucleus may also be difficult and the increased mobility of the posterior capsule may result in capsular damage.





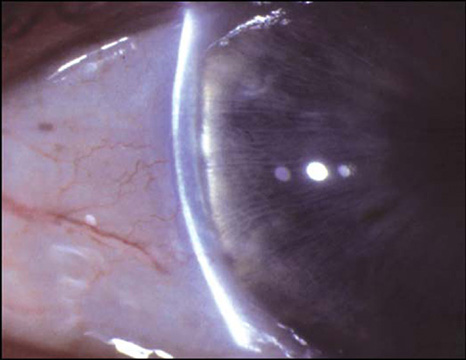
Fig. 1.19: The angle at which instruments enter the eye is more critical in an eye with a shallow anterior chamber.
ASSOCIATED OCULAR DISEASE
Uveitis
Identification of Potential Limitations
Identification of potential limitations for surgical success is important such as miosis, glaucoma band keratopathy (Fig. 1.20a), and cystoid macular oedema (Fig. 1.20b).
Control of Uveitis
Control of inflammatory activity prior to surgery is crucial to minimize complications. Ideally anterior chamber activity should be absent or minimal (+1 cells or less) for three months prior to surgery.

Fig. 1.20: Limitations for surgical success: (a) Band keratopathy and posterior synechiae (b) cystoid macular oedema.
In quiet eyes topical steroids (prednisolone acetate 1% or dexamethasone sodium 0.1%) are used six times a day, starting one week before surgery. Patients already receiving systemic steroids should have their dose increased.
Glaucoma
Filtration Bleb
A filtration bleb should be avoided when making the incision (Fig. 1.21).
Intraocular Pressure
Intraocular pressure may rise to over 60 mm Hg during surgery so that a severely damaged optic nerve head may sustain further damage. There is also a risk of postoperative steroid-induced ocular hypertension in patients with primary open-angle glaucoma.

Prior to surgery, elevated intraocular pressure should be controlled medically. Because combined trabeculectomy and cataract surgery may result in failure of the filtering procedure it is advisable to perform glaucoma surgery six months before cataract surgery.
Previous Vitrectomy
Uncertain Visual Outcome
Visual outcome may be uncertain because of pre-existing retinal pathology.
Lack of Vitreous Support
Lack of vitreous support may result in increased stress on the zonules, an excessively mobile posterior capsule and an increased risk for capsular tear.20
Other Factors
Sudden and paradoxical changes in size of pupil along with fluctuations in anterior chamber depth may put extra stress on the zonules. When the infusion is started the pupil dilates and the anterior chamber deepens; when the infusion is turned off the pupil constricts and the anterior chamber shallows.
Pseudoexfoliation
Pseudoexfoliation is associated with poor pupillary dilatation and weak zonules (Fig. 1.22). A capsular tension ring may minimize the risk of dropping the lens into the vitreous.
