

IMAGING TECHNIQUES AND ADVANCES
In the past skull radiographs were considered an essential step in the investigative protocol of a patient suspected to have neurological disease. With the availability of CT and MRI there has been a dramatic decline in the use of plain films and the indications for skull radiographs have been redefined.1,2 Patients presenting with stroke, epilepsy, dementia or in postoperative cases, skull X-rays generally provide no useful information and CT is the investigation of choice.3 In patients of trauma, CT should be the first line investigation except in patients who suffer from facial and orbital fractures where plain films are helpful in orientation and in medicolegal cases.4–6 Occasionally skull X-rays may reveal linear fractures with more certainty than CT scan.4 The skull radiographs play a major role in the diagnosis of dysplasias, infections and tumours affecting the skull bones, metabolic conditions such as leukaemia and multiple myeloma. In patients suspected to have intracerebral tumours, PA and lateral view of skull may provide additional information like detection of hyperostosis in case of meningiomas, presence of lytic and sclerotic metastasis in neuroblastomas and tram track calcification in Sturge-Weber syndrome which may compliment the diagnosis on CT. The present chapter will describe the normal roentgen anatomy as seen in the basic views of skull followed by systematic approach to the analysis of the abnormal skull X-rays.7–9
LATERAL VIEW OF SKULL (Fig. 1.1A)
A single lateral view of the skull is the most common radiographic X-ray examination performed. A systematic approach to the examination consists of evaluation of the size and shape of the cranium, the thickness and density of the bones, the sutures, the vascular markings, the base of skull and the cranial cavity.
Size and shape of the skull is determined by examining the relative size of face and cranium. When the skull is longer and has a relatively shorter vertical diameter it is referred to as dolichocephalic. On the other hand, when the vertical diameter is greater, it is termed as brachycephalic. The outer table, the inner table and the diploic space of the bones should be carefully examined to see any erosion, sclerosis or widening.
The normal sutures in adults are surrounded by a narrow area of increased density, a fact which helps to distinguish fracture lines from sutures. Sutures are difficult to visualise in newborns but in children older than 3 years, the width of the suture should not be more than 2 mm.


Fig. 1.1A: Normal lateral view of skull demonstrates the normal coronal sutures, lambdoid sutures and the vascular grooves due to middle meningeal vessels posterior to coronal sutures. Note the two lines formed by the roof of the orbits ending posteriorly at the anterior clinoid processes. Arrow head marks the tuberculum sellae. Vertical arrows show the cribriform plate anteriorly and planum sphenoidale posteriorly. Open arrow shows the greater wing of sphenoid bone forming anterior borders of middle cranial fossa. The dorsum sellae (horizontal arrow) with posterior clinoid processes above and the clivus posteriorly are well seen
Width of the sutures can be best assessed at the top of the coronal suture in the lateral view. To see the sagittal and the lambdoid sutures, PA and Towne's views are performed. Vascular markings are seen along the coronal suture due to middle meningeal vessels. Arterial grooves become narrower as they go distally. They may be confused with fracture lines but the latter are more radiolucent whereas vascular marking have a halo of increased density around them. Posterior branch of middle meningeal artery as it ascends upwards and posteriorly sometimes causes a shadow over the temporal bone that should not be mistaken for a fracture. Enlargement of the arterial grooves may occur in meningioma and arteriovenous malformations (Fig. 1.1B).

Fig. 1.1B: Lateral view of skull shows multiple dilated vascular markings in the parieto-occipital region in a case of parasagittal meningioma
Diploic venous channels are extremely variable in position but are generally seen in the frontal and parietal bones. Venous lakes may be seen as round or oval radiolucent areas and should not be confused with destructive lesions of the bone. Besides the arterial and diploic venous channels, the dural sinuses also produce grooves on the inner table of the skull.
The structures along the base of the skull should be carefully examined, in particular the three lines which represent the floor of the anterior cranial fossa. The upper two lines are formed by the roofs of the orbits which end posteriorly at the anterior clinoid processes. The lower line is formed anteriorly by the cribriform plate of the ethmoid bone and posteriorly by planum sphenoidale ending at the tuberculum sellae which marks the superior limit of the anterior wall of the sella turcica. A depression just anterior to the tuberculum sellae is called sulcus 3chiasmaticus. The roof of the sella posteriorly is formed by the dorsum sellae which ends in the posterior clinoid processes. Sphenoid sinus is seen below the floor of the sella turcica. The pneumatisation of this sinus shows considerable variation. Floor of the middle cranial fossa is formed by the greater wings of the sphenoid on each side which appear as curvilinear shadows concave outwards. These lines serve as a point of reference for locating the temporal lobe of the brain. The dorsum sellae continues as the clivus which is followed by the occipital bone ending at the anterior margin of the foramen magnum. Clivus is seen to terminate just above the top of the odontoid process of the axis. The normal calcification may be seen in the falx cerebri, petroclinoid ligaments, tentorium, pineal body, habenular commisure and choroid plexus.
FRONTAL VIEW (Fig. 1.2)
Posteroanterior (PA) projection with 15–20° craniocaudal angulation is preferred to straight PA projection as the petrous pyramids are projected below the orbits and the superior orbital fissure as well as greater and lesser wings of the sphenoid are clearly visualised. PA view is also examined for shape of the skull, with special attention to the symmetry of the two sides. The bony landmarks which require to be carefully examined for any erosions, sclerosis or lack of continuity include crista galli in the midline, planum sphenoidale, floor of the sella, lesser and greater wings of the sphenoid and the three lines of the orbit formed by the palpable superior border of orbit, highest point of roof of the orbit and the sphenoid ridge which represents the floor of the anterior cranial fossa. The floor of the posterior cranial fossa can also be seen inferiorly. Pacchionian depressions due to arachnoid granulations can be seen in both PA and lateral views as tiny radiolucent areas usually within 2.5 to 3 cm from the midline. Their margins are well defined superiorly whereas inferiorly the margins fade away-a feature helpful in distinguishing these from destructive lesions.

Fig. 1.2: PA view with 15° caudal angulation demonstrates the dense vertical bony projection in the midline due to crista galli, lesser wings of the sphenoid on both sides joining to form the planum sphenoidale (arrow heads). Floor of sella is faintly visualised in the midline (vertical arrows). Oblique line of the orbit is formed by the greater wing of sphenoid in its lower two-thirds and by the frontal bone in its upper one-third (horizontal arrows). Foramen rotundum and superior oblique fissure are well seen on the right side. Floor of the posterior cranial fossa is marked by open arrows
TOWNE'S VIEW (Fig. 1.3)
Towne's view is performed by angling the tube 35° caudally from the orbitomeatal line. It is generally performed when pathology is suspected in the petrous pyramids.

Fig. 1.3: Towne's view shows foramen magnum in the centre with dorsum sellae projecting through it. The parallel lucencies (short arrows) on either side represent the internal auditory canals. Further laterally pneumatised mastoids air cells can also be seen
This projection also shows the occipital bone, foramen magnum, dorsum sellae, the internal acoustic canals, mastoids and the condyles of mandible.

Fig. 1.4: Basal view of skull shows the nasopharynx, sphenoid sinus and ethmoid sinuses in the midline. Posteriorly odontoid process is seen to project into the foramen magnum posterior to the arch of atlas. Laterally, the foramen ovale (open arrow) foramen spinosum, (long arrow), eustachian tube posterior to foramen spinosum and the carotid canal are well visualised. Anterolaterally, the three lines formed by the posterior wall of orbit (arrow head) maxillary sinus (S-shaped) (curved arrow) and the anterior wall of middle cranial fossa (thick arrow) (arched shadow with concavity posteriorly) should be looked for in each case. Medial and lateral pterygoid plates are well seen
BASAL VIEW (Fig. 1.4)
Basal view of the skull or the submentovertical view is an infrequent examination and is generally performed in specific situations such as looking for the skull base lesions, middle ear or inner ear lesions, nasopharyngeal masses or oropharyngeal lesions and sinus pathologies. The bony landmarks that should always be identified and carefully examined include three lines, constituted by the lateral wall of the maxillary antrum (S-shaped), the posterolateral wall of the orbit, and the anterior wall of the middle cranial fossa which is arched with concavity pointing posteriorly. The lesser wing of the sphenoid is seen just behind the anterior wall of middle cranial fossa. A transverse dense line in the centre 5represents the anterior margin of sella. The medial and lateral pterygoid processes are projected over the sphenoid ridge. Sphenoid sinuses should be carefully seen as early bone destruction in patients of nasopharyngeal carcinoma or sphenoid sinus carcinoma is well demonstrated in this view.
There are three important foramina seen in the basal view. Foramen ovale lying behind the pterygoid processes gives passage to the 3rd division of the trigeminal nerve, an accessory meningeal artery and superficial petrosal nerve. Foramen spinosum lying behind and lateral to foramen ovale transmits the middle meningeal artery. Foramen lacerum is seen anterolateral to the petrous apex and has a well defined medial margin produced by the internal carotid artery. The Eustachian canal is seen behind the foramen spinosum. The external auditory canal is seen behind the condyle of the mandible. Internal auditory canals and inner ear structures including semicircular canals should be carefully looked for. The clivus and foramen magnum are well seen through which the anterior arch of atlas and odontoid process of axis are seen to project. Jugular fossa and jugular foramen are seen laterally on each side of the junction of petrous portion of the temporal bone and occipital bone.
WATERS VIEW (Fig. 1.5)
It is one of the standard views to study the maxillary and anterior ethmoidal sinuses. Waters view is generally performed with the patient in sitting position to facilitate demonstration of any fluid level in the sinuses. Patient is instructed to keep the mouth open with nose and chin touching the cassette in order to visualise the sphenoid sinuses. It is performed by placing the orbitomeatal line at an angle of 35 degrees with the plane of film by either raising the chin or by tilting the tube. It also gives clear picture of the roof of the orbits, destruction of which may be seen in mucocele of frontal sinus and in carcinoma of lacrimal gland.
CALDWELL'S VIEW
Caldwell's view is best projection for examining the frontal and ethmoid sinuses. Patient is positioned directly facing the cassette in either sitting or prone position with midsagittal plane and orbitomeatal line perpendicular to the film with nose and forehead touching the cassette. Central ray is directed 15 degrees caudally to the nasion.
The various abnormalities that can be detected on the plain skull X-rays can be categorised in the following groups:
- Abnormal contour of the skull
- Abnormal intracranial volume
- Intracranial calcification
- Increased thickness of the skull
- Single lucent defect
- Multiple lucent defects
- Sclerotic areas

Abnormal Contour of the Skull
Normal contour of the skull is maintained by sutures, the intracranial contents and normal bone formation. Abnormality in any of these may result in abnormal contour of the skull.
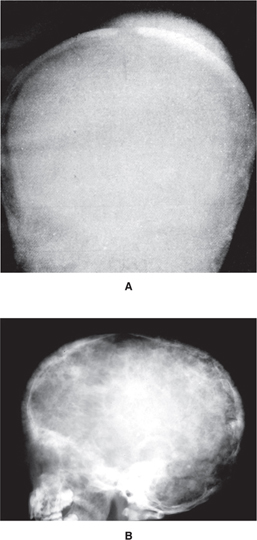
Premature fusion of the sutures, Craniosynostosis is the commonest cause of abnormal contour in children. If the suture closes early, the calvarium expands to accommodate the growing brain in the axis of the fused suture. Thus premature closure of the sagittal suture leads to an elongated narrow skull- scaphocephaly whereas closure of both coronal sutures and lambdoid sutures produces a short wide skull with high head - turricephaly (Fig. 1.6). Plagiocephaly results when there is unilateral coronal synostosis. In this condition, there is elongation of the orbit, elevation of the lateral portion of ipsilateral orbital rim (the harlequin appearance) and tilting of the nasal septum and crista galli towards the affected side. Margins of the affected sutures develop sclerosis. Any decrease or increase in the cerebral volume may result in abnormal contour. Premature fusion of multiple sutures on one side is associated with signs of raised intracranial tension in the form of increased convolutional markings. The hemi calvarium on the ipsilateral side is smaller than the opposite side. The tables of bones of the skull are thickened and there may be elevation of the petrous pyramid on the same side.

Fig. 1.6: Craniosynostosis: Lateral view of skull shows silver beaten appearance due to exaggerated convolutional markings all over the skull vault. None of the sutures are seen
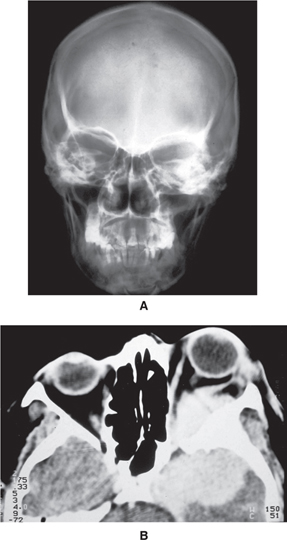
Expansion of the bony calvarium due to the presence of slow growing intracerebral or subarachnoid space occupying lesions such as arachnoid cysts may also result in abnormal contour (Figs 1.7A and B). The bony vault bulges outwards with thinning of the inner table. Chronic subdural haematomas may also cause expansion of the adjacent calvarium and may even erode the inner table. Calcifications when present facilitates the diagnosis.
Abnormal bone formation such as that occurs in achondroplasia characterised by defective enchondral ossification, results in shortening of the bones of the skull base as these bones develop from cartilage. Since the bones of the vault develop from membranous bones, these remain unaffected. The result is a small foramen magnum and enlarged cranium with frontal bossing and large jaws.
Abnormal Intracranial Volume
Size of the calvarium is dependent on the size of the intracranial contents. The most accurate way to determine abnormal cranial volume is to measure the skull directly and compare the measurements to standard for age and body size. A simple method of assessing the size of the skull is to compare the skull vault to the size of the face.

Figs 1.7A and B: Arachnoid cyst: (A) Basal view of skull shows thinning and ballooning of anterior and lateral walls of the left middle cranial fossa (arrow) (B) Axial CT scan of the same patient shows a large left temporoparietal arachnoid cyst
At birth, the volume of skull is approximately four times that of face. This ratio decreases to 3:1 by age 2 and 1.5:1 by adulthood.8
Enlarged head, size may result from hydrocephalus, macrocephaly, hydranencephaly and in pituitary dwarfism. The most common cause of hydrocephalus in children is congenital obstruction of the ventricular system and is associated with raised intracranial tension. Sutures become wide due to expansion of the intracranial contents.
Small skull but otherwise normal contour is characteristically seen in microcephaly associated with mental retardation. Cranial sutures fuse early but this is a result of microcephaly and not the cause. The sinuses are large and the digital or convolutional markings are absent or decreased. It is important to differentiate premature closure of all the sutures from microcephaly with fused sutures. When multiple sutures fuse prematurely, the fusion does not occur simultaneously and the result is an irregular skull due to expansion of the skull in unusual directions to accommodate the brain. Clinically signs of raised intracranial tension are present. Convolutional markings are exaggerated.
Increased thickness of the skull may result due to early cessation of brain growth or due to cerebral atrophy. Increased width of diploic space due to increased haematopoiesis is seen in haemolytic anaemias. Progressive hydrocephalus leads to large bony calvarium and a decreased diploic space. However, if a ventricular shunt is performed and abnormal expansion ceases resulting in arrested hydrocephalus, the cranial sutures close and the inner table of bones of the skull become thicker and the diploic space becomes larger. A history of hydrocephalus and the presence of a ventricular shunt facilitates the diagnosis
Among the haemolytic anaemias producing hyperplasia of the bone marrow, 8thalassaemia causes most marked changes. The diploic space is widened with striking radial striations, the “hair-on-end” appearance (Fig. 1.8). The paranasal sinuses may also be completely obliterated due to widening of the diploic space of facial bones. Such changes may also be seen in other forms of anaemias such as sickle cell disease, hereditary spherocytosis but the changes are much less marked.
Single Radiolucent Defect
When there is a single lucent lesion, the important considerations that help in deciding its nature are its location, associated soft tissue swelling, table of the bone involved and margins of the lytic lesion, whether sharp, ill-defined or sclerotic. Radiolucent defects in the skull bone may be due to variety of causes which may be congenital or acquired. Congenital causes may be parietal foramina, anomalous apertures, meningoencephalocele or dermal sinus. The acquired causes include trauma, infections, tumours and histiocytosis.

Fig. 1.8: Thalassaemia: Lateral skull radiograph shows widened diploic space with coarsened trabeculae giving “hair-on-end” appearance typical of haemolytic anaemia
Bilaterally symmetrical rounded lytic defects located in the posterior parietal bone are characteristic of parietal foramina and are of no clinical significance. Lytic defects due to meningoencephalocele are located in the midline in the frontal or occipital regions and have sharp margins. Associated soft tissue mass clinches the diagnosis. In the first 3 months of life, meningoencephalocele is generally associated with lacunar skull (craniolacunia) (Fig. 1.9). A dermal sinus also occurs in the midline of the skull and may present as a radiolucent defect with a sharp slightly sclerotic border. It is generally associated with a lipoma or a nevus in the overlying soft tissues. These lesions may have an intracranial components which may require a CT scan for demonstration.
Fractures generally occur at the site of injury and may be associated with soft tissue swelling. Linear non-depressed fractures may be seen as radiolucent lines and should not be confused with sutures or vascular grooves.

Fig. 1.9: Craniolacunia: Lateral skull radiograph in an infant shows multiple lucencies with intervening dense areas typical of craniolacunia. Note the associated occipital encephalocele and absence of sutural widening
Fracture lines are non-tapering, non-branching and have sharp borders whereas vascular grooves have ill-defined borders and an undulating course. Sutures are seen in known anatomical positions and have saw tooth edges. Depressed fractures generally occur after severe trauma and are considered more serious than linear fractures. Radiologically the depressed fragment presents as area of increased radiodensity surrounded by a radiolucent zone (Fig. 1.10). In children, when the dura beneath the suture is torn, the arachnoid membrane herniates through the dura into the bony defect. The pulsations of the brain lead to progressive enlargement of the arachnoid collection resulting in expansion of the fracture line termed as growing skull fracture. The bulging membranes result in the formation of leptomeningeal cyst (Fig. 1.11)

Fig. 1.10: Depressed fracture: Frontal radiograph shows the parallel dense lines due to depressed bone fragments and associated lucency due to absence of bone
Infections of the skull are uncommon and generally follow trauma or arise secondary to infection elsewhere in the body. The radiographic appearance consists of mottled irregular lucencies which have ill-defined borders and are associated with soft tissue swelling of the scalp.
Epidermoid tumours develop from a congenital inclusion of epithelial cells within the calvarium.

Fig. 1.11: Growing fracture: PA skull radiographs in a child demonstrate fracture of the right frontal bone with thickening, sclerosis and wide separation of the fracture ends. Note the soft tissue swelling overlying this area
Radiologically these lesions present as well-defined lytic lesions which have sclerotic border and are not necessarily located in the midline. Intracranial epidermoids may also produce a radiolucent shadow which may mimick a lytic lesion (Figs 1.12A and B).

Figs 1.12A and B: Single lucent lesion: (A) lateral skull radiograph shows a well circumscribed lucency overlying the coronal suture mimicking a lytic lesion. (B) Coronal CT scan in the same patient shows a large hypodense lesion due to epidermoid in the temporoparietal region. No lytic lesion of skull vault is seen
Malignant lesions such as primary osteosarcoma or metastasis can also produce lytic defects. Osteosarcoma causes gross destruction of the bone with ill-defined margins and soft tissue swelling (Figs 1.13A and B). Neurofibromatosis is a rare cause of a lytic defect seen along the suture. This defect is not due to the presence of neurofibroma but is a manifestation of mesenchymal defect. Intracranial mass lesions can also rarely present as lytic areas of the skull.
Eosinophilic granulomas, Hand-Schüller Christian disease and Letterer-Siwe disease all form part of a complex comprising, histiocytosis. The severity ranges from mild in eosinophilic granuloma to very malignant course in Letterer-Siwe disease. A single lytic lesion having sharp non-sclerotic border and bevelled edges is characteristic of eosinophilic granulomas. Occasionally a small bone is seen in the centre representing button sequestrum. Lytic lesions in the other two variants are larger, multiple and punched out (Fig. 1.14).
Multiple radiolucent defects in the skull in children may be due to craniolacunia, presence of wormian bones, increased convolutional makings due to raised intracranial tension, histiocytosis and metastasis from neuroblastoma (Figs 1.15A and B), leukaemia or Ewing's sarcoma. In adults multiple myeloma (Fig. 1.16), metastasis and hyperparathyroidism (Fig. 1.17) are the usual causes.
Craniolacunia is due to a defect in ossification of the bones which develop from membranous tissue. There are multiple radiolucent defects seen all over the cranial vault interspersed with strips of normal bone which appear dense. Craniolacunia (Lacunar skull) by itself is not of much significance but it is generally associated with myelomeningocele or encephalocele (Fig. 1.9).

Figs 1.13A and B: Osteosarcoma (A) Large lytic area with irregular margin is seen affecting the left parietal bone (B) CT scan of the same patient shows the soft tissue swelling, destruction of the bone and extradural extension of the tumour
Appearance must not be confused with increased convolutional markings that result from raised intracranial tension and are seen as multiple radiolucent areas not exceeding the diameter of a finger. Convolutional marking may also be seen in normal children in the frontal and occipital region. Presence of increased convolutional markings in the parietal region should generally be considered abnormal. Wormian bones are seen along the sutures and results due to defective mineralisation. Multiple wormian bones are seen in cleidocranial dysostosis, osteogenesis imperfecta, hypothyroidism and pyknodysostosis.
Lytic lesions seen in multiple myeloma are punched out, usually associated with osteoporosis and involve the mandible more frequently compared to metastasis. However, many times differentiation from metastasis may not be possible on radiological appearance alone. Hyperparathyroidism generally results in mottled demineralization but may sometimes cause multiple well-defined lytic areas (Fig. 1.17).

Fig. 1.14: Histiocytosis (Hand-Schüller-Christian disease): Lateral radiograph of skull shows multiple well-defined lytic lesions of the vault with bevelled edges characteristic of histiocytosis
Figs 1.15A and B: Metastatic lesions of the skull in a child with abdominal neuroblastoma (A) Sutural metastasis: Frontal skull radiograph shows widening of the sagittal suture with an overlying soft tissue swelling. (B) Diffuse metastasis of skull vault: Lateral skull radiograph shows multiple lytic areas involving both tables of skull and diploic space. Note widening of coronal suture also

Fig. 1.16: Multiple myeloma: Lateral skull radiographs shows multiple well-defined punched out lytic lesions affecting the skull vault as well as mandible typical of myeloma

Fig. 1.17: Hyperparathyroidism: Lateral skull radiograph shows multiple well circumscribed rounded lytic lesions involving skull vault with bone within bone appearance-an unusual feature of hyperparathyroidism
Sclerotic Areas of the Skull
Areas of increased density in the skull may be seen in both normal as well as pathological conditions. Osteopetrosis is a rare condition which is characterized by diffuse thickening of the skull and face (Fig. 1.18). Fibrous dysplasia may involve the vault or base of skull. There may be a single lesion or it may be part of syndrome (McCune-Albright syndrome) seen in females when it affects multiple bones and is associated with precocious puberty. The lesions are sclerotic with loss of normal trabecular pattern. Mixed type of lesions with sclerotic and lytic areas are also known to occur (Figs 1.19A and B). Multiple hyperostotic lesions affecting the calvarium measuring 5–10 mm in size may be seen in tuberous sclerosis in association with calcified lesion in periventricular region. Thickening of the frontal and parietal bones may occur in rickets due to presence of poorly mineralised bone which on healing becomes dense.

Fig. 1.18: Osteopetrosis: Frontal radiograph shows diffuse increased density affecting all bones of the skull vault as well as base

Figs 1.19A and B: Fibrous dysplasia: Frontal (A) and lateral (B) views of skull reveal a mixed lytic and sclerotic lesions involving the right frontal bone. The maxillary antrum is opaque due to involvement of right maxilla
An osteoma affecting the skull bones is a benign tumour which appears as a dense lesion projecting extracranially from the outer table of skull. Osteoma is also the commonest benign tumour affecting the sinuses (Fig. 1.20). Focal areas of hyperostosis are characteristic of meningioma (Figs 1.21A and B). When the hyperostosis affects the frontal bone, in a case of convexity meningioma, it must be differentiated from hyperostosis frontalis interna (Fig. 1.22), the later is generally seen in elderly females and affects the inner table with sparing of diploic space and does not cross the midline.
Intracranial Calcification
Presence of calcification can provide important clue to the diagnosis in several conditions. Although causes are numerous (Table 1.1) some of these conditions have specific appearance which can be diagnostic.
The most common physiological calcification occurs in the pineal gland. It is seen in the midline approximately 3 cm above and behind the posterior clinoids in the lateral view. Size of the pineal calcification is most important as any increase in size more than 10 mm is abnormal and raises the possibility of pinealoma.

Figs 1.21A and B: Sphenoid wing meningioma (A) PA view of skull shows hyperostosis of the lesser and greater wings of the sphenoid bone (L) typical of meningioma (B) Contrast enhanced CT scan in the same patient shows proptosis and hyperostosis of sphenoid wings with enhancing extradural mass due to meningioma on the left side
Habenular commissure calcification has a characteristic appearance and is seen as a C shaped structure open posteriorly.

Fig. 1.22: Hyperostosis frontalis interna: Lateral skull radiograph shows irregular thickening of the frontal bone in an elderly female. The inner table is involved more than the outer table with sparing of diploic spaces
It lies above and anterior to pineal gland. Choroid plexus calcification is generally bilateral and may be unequal on the two sides. Other normal sites of calcification are the falx and anterior petroclinoid ligaments above the sella.
Tuberous sclerosis is a syndrome comprised of epilepsy, mental retardation and adenoma sebaceum. Multiple hamartomas occur in the brain as well as at other sites such as kidneys. Tumours consist of glial tissue and ganglion cells. In the brain they are usually multiple and are seen in the subcortical, subependymal and basal ganglia regions. Calcification is seen in 50 per cent of the lesions.
Sturge-Weber syndrome is another important cause of intracranial calcification. Patients present with epilepsy and mental retardation and often have cutaneous haemangioma in the distribution of trigeminal nerve on the same side as calcification. Calcification has a typical tram track appearance and is seen in the cerebral cortex (Figs 1.23A and B).
Basal ganglia calcification is an important feature of hypoparathyroidism and pseudohypoparathyroidism. Wide spread irregular and punctate areas of calcification which are diffusely scattered are characteristic of Fahr's disease. In this condition patients present with severe growth and mental retardation. The disease is hereditary and is characterised by microscopic deposits of iron and calcium in the basal ganglia, cerebellum and subcortical region. Infections due to toxoplasma and cytomegalovirus are important causes of intracranial calcification in the newborn. Calcifications are multiple and diffusely scattered in the brain parenchyma or paraventricular region. Bacterial infections may progress to cerebral abscess which may get calcified.
Arteriovenous malformations calcify in 2–25 per cent of all affected patients. Typically calcification is in the form of an incomplete ring but may be nodular or amorphous.16

Figs 1.23A and B: Sturge-Weber syndrome: PA (A) and lateral (B) view of the skull shows gyriform calcification in the right frontal region
A large arc like calcification seen in the region of pineal gland in a newborn presenting with congestive heart failure and hydrocephalus is characteristic of vein of Galen aneurysm. Intracerebral or chronic subdural haematomas may reveal curvilinear calcification. A variety of tumours may show calcification. In children, suprasellar craniopharyngioma is the most common tumour which reveals calcification whereas in adults oligodendrogliomas and meningiomas are the common tumours to calcify.
REFERENCES
- Tress BM. The need for skull radiography in patients presenting for CT. Radiology 146: 87; 1983.
- Moseley I. Long term effects of the introduction of noninvasive investigations in neuroradiology. Neuroradiology 30: 193–200; 1988.
- Rastogi SC, Barraclough BM. Skull radiography in patients with psychiatric disease. Br Med J 287: 1259; 1983.
- Taveras JM. Anatomy and examination of skull. In: Interactive Review of Radiology Williams and Wilkins, Lippincotts 1999.
- Sanders R, MacEwen CJ, McCulloch AS. The value of skull radiography in ophthalmology. Acta Radiological 35: 429–33; 1994.
- Baker HL Jr. The impact of computed tomography on neuroradiologic practice. Radiology 116: 637–40; 1975.
- Taveras JM. The skull. In: Taveras JM, Wood EH (Eds): Diagnostic Neuroradiology, 2nd edn. The Williams and Wilkins Company, 1–65; 1986
- Gerald B. Systematic Radiographic Evaluation of the Abnormal Skull. In: Rabinowitz JG (Ed) Pediatric Radiology. JB Lippincott Company, 285–313; 1978.
- Butler P, Jeffiree MA. The skull and brain. In: Butler P, Mitchell AWM, Ellis H (Eds): Applied Radiological Anatomy, 1st edn. Cambridge University Press 17–60; 2001.