

Conjunctiva is a thin translucent vascular membrane which cover the under surface of the lids and reflected over anterior surface of the sclera up to the limbus. It consists of two layers, the outer one is the epithelium and inner one is the stroma. The stromal layer consists of blood vessels, connective tissues, glands such as Krauses, Wolfring and Goblet cells. The conjunctiva is supplied by sensory nerve via branches of ophthalmic and maxillary division of 5th cranial nerve. Sympathetic nerves are derived from sympathetic plexus.
Bacteriology: Non-pathogenic bacteria–Diplococci, Corynebacterium xerosis, Staphylococcus albus, etc.
Pathogenic Bacteria – Streptococcus, E.coli, B.proteus, gonococci, H. aegyptius, Moraxella, etc.
Virus- Adenovirus, herpes.
DISEASES OF THE CONJUNCTIVA
Inflammation (conjunctivitis): Classification
- Infective—
- Acute
- Sub-acute or chronic
- Allergic—
- Acute or subacute
- Phlyctenular
- Spring or vernal—conjunctivitis.
INFECTIVE CONJUNCTIVITIS
1. Acute Mucopurulent Conjunctivitis
It is often associated with measles and scarlet fever. It occur as epidemic and usually bilateral. It is contagious and spreads by flies, fingers and fomites. It is self limiting.
Symptoms
There is readness of the conjunctiva with the foreign body sensation.
Mucopurulent discharge sticking together of lids specially in the morning because of accumulation of mucous discharge during the night.
Colour haloes due to flakes of mucous passing across the cornea.
Signs
Conjunctival-congestion with red eye. Chemosis of conjunctiva may be associated with subconjunctival haemorrhage.
Complications
Superficial-keratitis and marginal corneal ulcer.
Aetiology
Staphylococci, Haemophilus aegypticus, pneumococci.
Treatment
- Isolate the patient
- Avoid using the patients towel
- Antibiotic eye drop as: Ciplofloxacin, gentamycin, tobramycin, neomycin, etc. according to culture + sensitivity for hourly use.
- Antibiotic ointments as chloromycetin, gentamycin, tetracycline, ciprofloxacin, etc. used 8 hourly.
2. Purulent Conjunctivitis
It is contagious, due to the gonococci, staphylococci and Corynebacterium diphtheriae.
Right eye affected first.
Signs/Symptoms
Common in adults as well in children. In adult the infection comes from genitals. Swelling of the lids + conjunctival congestion with chemosis +ve. Copious purulent discharge +ve. Cornea is diffuse and hazy with gray or yellow spot on the centre. Ulcer may be formed at any part of the cornea due to necrosis of epithelium. Marginal ulcer may extent completely due to collection of pus and bacteria at gutter. Ulcer may be perforated. Iridocyclitis, endocarditis even septicaemia may also form as its complications.
Rise of temperature, mental depression, preauricular glands are enlarged and tender. Incubation period is from few hours to 3 days with the coincidence of urethritis.3
Treatment
- Cleaning of the conjunctival sac with warm water.
- Instillation of penicillin drops (10,000 units/ml) every minute for ½, later can be continue for hourly for 3 days.
- Tetracycline, ciprofloxacin, gentamycin, tobramycin, etc. can be used according to culture and sensitivity test.
- Atropine is applied if there is involvement of cornea.
OPHTHALMIA NEONATORUM
It occur in the new baby due to maternal infection. This is virulent conococci infection cause 50% blindness in children. It is usually bilateral.
Signs/Symptoms
Discharge purulent +ve with the oedematous eyelids. Conjunctiva intensively inflamed, bright red, with marked chemosis. Later on purulent discharge changes into the mixture of pus, serum and blood.
Complications
Cornea hazy due to the marginal and central ulceration, it may lead the perforation of the cornea—Iris prolapse, lens may be extruded and ultimately form panophthalmitis. Metastatic stomatitis and arthritis of big joints 3-4 weeks of the disease.
Treatment
- Same as purulent conjunctivitis in the form of penicillin drops and antibiotics. In addition to this Penicillin is given in the form of parental/intramuscular.
- Precautionary measure if there is vaginal discharge should be treated.
- Aseptic precaution at the time of child birth should be taken.
- Penicillin drops or Ag NO3 1% should be instilled in the eyes of newborn.
Sequelaes are:- Corneal opacity
- Adherent leucoma, partial or complete
- Ant. capsular cataract.
- Macular fixation defective so develops the nystagmus and persists throughout the life.
- Membraneous conjunctivitis: Conjunctiva is covered by fibrinous membrane.Etilogical factor is Diphtheriae bacilli. Pseudomembrane may be formed due to the Pneumococcus and Streptococcus in weak children who have 4suffered from measles and Scarlet fever. Common in unimmunized children.Pseudomembrane can be seperarted from conjuntiva but true membrane not. It may cause bleeding if true membrane is peeled of rapidly.
Signs/Symptoms
Swelling of the lids +ve with serous or mucopurulent discharge.
Palpebral conjunctiva is covered by white membrane.
Cause the bleeding if membrane is peeled of from conjunctiva. In severe cases lids are browny and membrane firmly attached with conjunctiva by semisolid exudates. Show the changes of necrosis in conjunctiva and cornea.
Preauricular glands +ve later on symblepharon may develop in 12 hours with the associate treatment until and up to negative swab result from throat and conjunctiva.
Treatment
Every case should be treated as diphtheria unless good negative evidence is offorded. This consists of the intensive local and general administration of penicillin together with the prompt injection of antidiphtheritic serum (4-6-10,000 units repeated in 12 hours). Antitoxin given early and in adequate amounts both locally and systemically is curative, but it should be combined with the antibiotic.
CHRONIC—CONJUNCTIVITIS
- Simple chronic conjunctivitis
- Angular conjunctivitis
- Follicular conjunctivitis
- Trachoma
- Tuberculosis
- Syphilis
- Tularemia.
Simple Chronic Conjunctivitis
It is the continuation of simple acute conjunctivitis. It is frequent when a cause of irritation is continuous as smoke, dust, heat, bad air, permanent irritation from concretion in the palpebral conjunctiva, misplaced lashes, dacryocystitis, chronic rhinitis, etc.
Signs/Symptoms
Burning and grittiness. Difficulty in keeping eye open.
Conjunctival congetion of palpebral + bulbar conjunctiva +ve
Treatment
Treatment for the cause.
Angular Conjunctivitis
Intermarginal strip of the bulbar conjunctiva is conjested at the inner and outer canthi. Excoriation of the skin at the inner and outer palpebral angles. Complaints are frequent Blinking + Mucopurulent discharge.
Complications
1) Blepharitis, 2) Marginal, central or hypopyon corneal ulcer.
- Pathologicla organism Moraxella bacilli, staphylococci and diplobacilli. Morax axenfield Diplobacillus is found in nasal cavity, so nasal discharge is common with angular conjunctivitis. Incubation period is of 4 days.T/T: Oxytetracycline and zinc oxide ointment frequently used.
Follicular Conjunctivitis
Associated with the development of follicles that is the aggregation of lymphocyte cells. In children the follicles develop after the age of 3 months.
Aetiology
- Allergic conditions
- Virus infections, e.g. herpes and adenovirus
- Certain chemicals and toxins, e.g. pilocarpine, eserine.S/S: Irritation and discomfort with FB sensation.
Trachoma
It was the major cause for blindness as 1/5 of world population is affected by trachoma. It is commonly seen in crowded unhygienic dusty and dirty environment. It is not racial disease. Chlamydia trachomatis is the cause of this disease, spread by sexual transmission. Contagious disease in its acute stage being spread by the transference of conjunctival secretion by such means fingers, towel, or by flies. Primary infection is epithelium and involves both conjunctiva and cornea.
Conjunctiva — Diffuse inflammation with congestion, characterized by papillary enlargement and development of follicles. Conjunctiva covering the tarsal plate is affected mostly. Each follicle is of 5 mm in diameter. Follicles are arranged in the form of row at the border of the eyelid over the tarsal plate. Cicatrization of the follicles is the important diagnostic feature.6



Cornea — Manifest as superficial keratitis, later on converted in to superficial erosion. Cornea is vascularized with the infiltration of lymphocytes cells called as Pannus. Branches of corneal vascularization come from anterior ciliary and episcleral blood vessels. The follicles along with infiltration at limbus and converted in to pits are known as ‘Herbert's pits (Fig. 1.1).
Blood vessels are superficial in between the epithelial and Bowman's membrane. Later on the Bowman's membrane disappear and superficial layer of substansia propria is involved and corneal ulcer is formed which is the only complication of trachoma, commonly situated at the advancing edge of the Pannus. The ulcer is shallow, little infiltrated and very irritable cause lacrimation and photophobia. Pannus may resolve completely leaving the cornea quite clear apart from the obliterated blood vessels where Bowman's membrane is not destroyed. In other case permant opacity results.
Varities of Pannus (Fig. 1.2)—Two types of pannus:
- Progressive pannus
- Regressive pannus.
Progressive pannus: Lymphocytes infiltration is beyond the growing end of blood vessels indicate the acute stage of the disease.

Pathology: Chlamydia trachomatis is seen inconjunctival scraping in the colony form in the epithelial cells as Halberstadter-Prowazek inclusive body. Inclusive body burst and liberate the large number of elimentary bodies.
The elimentary body attach the new cell and enter in it's cytoplasm and form the new inclusive body. Aggregation of lymphocytes is the follicles. Because of hyline and other degenerative changes fibrous tissue is formed and later on converted in to cicatrical band which is the characteristic of trachoma. The multinucleated inclusive body is known as Laber's cell (Fig. 1.3).
SEQUELAE COMPLICATIONS
Corneal ulcer is the only complication of trachoma.
Sequelae are:
- Trichiasis — Misdirected eye lashes due to cicatrization.
- Entropion — Rolling of lid margin due to scarring.
- Ptosis — Due to the increase weight of the eyelids.
- Xerosis — Due to the destruction of goblet cells because of conjunctival scarring.
Diagnosis
- Clinical: By the presence of follicles or papillae
- Epithelial keratitis
- Pannus formation, and
- Scarring of conjunctiva (Fig. 1.4).
Laboratory

Treatment
- Topical treatment
- Sulfacetamide drops 20-30% twice a day for 3 months.
- Artificial drops for xerosis.
- Systemic
- Doxycycline 5 mg/kg of body weight once per month for 12 months.
- Tetracycline, erythromycin and sulfonamides are effective.
- Surgical — Excision of fornix — in the situation of large follicles.–Tarsectomy to get relief from ptosis.Surgical treatment for sequelae as Trichiasis, Entropion.
ALLERGIC CONJUNCTIVITIS
Acute or Subacute Catarrhal Conjunctivitis
It is acute reaction to allergen.
- Bacterial protein of endogenous nature e.g. staphylococci in nose.
- Exogenous protein as in Hay fever, contact with animals, e.g. dog, cat, etc.
- Chemicals — Cosmatic, Drugs, e.g. atropine, hair dye, etc.
Signs and Symptoms
Itching with watery secretion and marked redness of the conjunctiva. Secretion contains the large number of eosinophilia.
Treatment
Removal of allergan, anti-histaminic drugs, corticosteroid drops useful in severe cases.
Phlyctenular Conjunctivitis
It is characterized having phlycten or Bleb at the limbus, is supposed to be due to the tuberculous protein. In some cases it is associated with the infection of tonsil and adenoid. It is common in children in between the ages of 5 to 15 years.9
One or more nodular swelling grey-yellow in colour with the bulbar conjunctiva close to the limbus. It is not tender. Bulbar conjunctiva is not movable over the nodule separately. Whenever, the involvement of cornea is there it is known as ‘Phlyctenular keratoconjunctivitis’.
Treatment
Corticosteroid in the form drops and ointment is very effective. Treatment should be given for the cause, e.g. tuberculosis, tonsil and adenoid, etc.
Vernal Conjunctivitis (Fig. 1.5)
It is caused by the exogenous allergen such as pollen and dust. It is common in young boys 5 to 15 years. It is bilateral, usually occurs at the onset of hot weather. Patients main complains are: 1) Itching. 2) Thick white ropy mucous discharge. 3) Burning and foreign body sensation. 4) Photophobi, and 5) Lacrimation.
Types
- Palpebral form: Palpebral conjunctiva shows multiple polygonal nodular swelling looks like cobbles stones, milky-white in colour. Nodules are hard as it contains dense fibrous tissues and eosinophils.
- Bulbar form: Multiples nodular are around the upper part of the limbus. Discrete chaky-white superficial spots are known as ‘Horner-Tranta's dots composed of eosinophils.
This disease may persist for several years. Because of development of resistance jn majority of cases disease may subside at puberty. Cornea may be affected as the complication in the form of superficial punctate keratitis, epithelial macroerosion and ulcer.
Treatment
- Topical corticosteroids in the form of drops and ointment, e.g. dexamethasone or betamethasone .o1%.Steroid drops are instilled in low concentration to avoid the steroid induce glaucoma and cataract formation.
- Acetyl cystine —10 to 20% drops control excess mucous formation.
- Disodium cromoglycate 2% drops four times a day. It helps to release histamine.
- Cryotherapy of the nodule may be effective.
- Nonsteroid anti-inflammatory drugs 'NSAIDs, e.g. flurbiprofen, indomethacin, etc.
- Supra tarsal injection of steroids e.g. Depomedrol o.25 ml is very effective.
- Surgical management — Removal of large mucous plaques.

DEGENERATIONS
CONCRETION
This is the accumulation of epithelial cells and inspissated mucus in Henle's gland. Occur as minute, hard, yellow spot in the palpebral conjunctiva project from the surface. It scratches the cornea and gives the sensation of foreign body, commonly in the elderly people.
Treatment
Should be removed with the sharp needle under the topical anaesthesia.
PINGUECULA
Trangular patch on the conjunctiva. Common in the elderly people, those exposed to the strong sun light, dust. wind and so on. Yellow in colour and look like a fat (fat = pinquis). It is situated near the limbus in the palpebral aperture. The base of the pinguecula is always toward rhe limbus and apex away from the cornea. This is due to the hyaline infiltration and elastotic degeneration of the submucous tissue.
Treatment
No treatment as it is symptomless condition.
PTERYGIUM
Degenerative condition of the conjunctiva which encroaches over the cornea in the form of vascular granulation sheath. It is the subepithelial hyaline type degeneration, commonly in the sunny climate. Ultraviolet light is probably an aetiological factor. It is bilateral commonly present on nasal side, males are affected more. In some cases it presents on the nasal side as well as temporal side in the unilateral eye. It is triangular in shape consists of head, neck and body. Pterygium invades the cornea by 11head and involve the Bowman's membrane and the superficial layer of stroma. It is loosely attached to the sclera by its whole length. The area of its adhesion being always smaller than its breadth. So that there are folds at the upper and lower border of the pterygium. It frequently follows the pinguecula.
Classification
- True pterygium
- Pseudopterygium.
True pterygium is differentiated by it's site in the inter palpebral region and the probe can not pass beneath the truepterygium as in pseudopterygium. Truepterygium is the degenerative phenomenon where as pseudo-pterygium is the postinflammatory.
True pterygium is classified
- Benigin
- Malignant
- Vascular
- Avascular
- Atropic
- Recurrent.
Treatment
Pterygium is supposed to be the minor ocular disorder but major ophthalmic problem because of it's high rate of recurrence. Surgery is the only choice of treatment. Encroachment of the pterygium's head over the pupillary area not less than 1 mm by which the vision of the patient is affected may be considered for the surgery.
Surgeries are:
- Simple excision with or without bare sclera
- Excision of the pterygium with lamellar keratoplasty.
- Transplantation of the epithelial layer of the conjunctiva from the other part of the eyeball, mucous membrane autograph or amniotic membrane graph after the excision of the pterygium.
- Beta-radiation — 2500 rads are given in the first week.
- Thiotepa 1:2000 solution is applied 4 times a day for 6 weeks. It prevent the recurance of the pterygium.
- Mitomycin C. 04% is effective to prevent the recurrance of pterygium. The procedure of 4th, 5th, and 6th is used after the primary surgical procedure to prevent the recurrance of the pterygium.
- Argon Laser can be used in pterygium by obliterating blood vessels.
- Transposition of pterygium by:
- Mc Reynold's technique
- Pawar's modified technique.
In the Mc Reynold's technique the pterygium is separated from the cornea and underlined sclera and then the whole pterygium mass is undermined at the upper or lower fornix under the tenon's capsule.
Pawar's Modified technique: Epithelial layer is separated from the fleshy-vascular mass of pterygium (Figs 1.6 A to G).
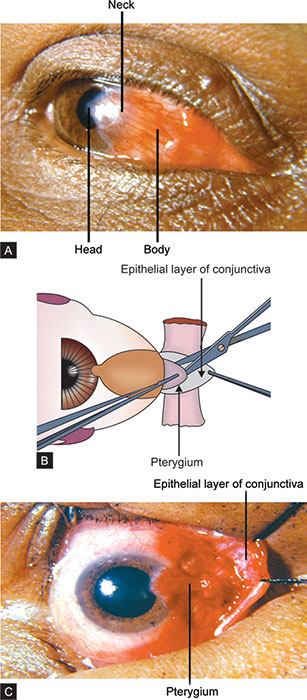

- Pterygium is divided in two equal parts from head to body after separating the encroached head and adherent portion from sclera.Divided heads of the pterygium is cauterized, along with the bare sclera close to the limbus.
- Two divided portion of pterygium along with the cauterized heads are fixed with the vicryl 6/0 to the sclera at the upper and lower fornix beneath the tenon's capsule.
- Reflected epithelial layer is replaced and sutured.
- This is the good surgical technique particularly in the cases of recurrent pterygium.
CYSTS AND TUMOURS
Cysts
The common conjunctival cysts are due to: 1) Lymphangiomata: This is due to the dilation of lymph spaces (Lymphangiectasis). 2) Larger retention cyst of Krause's accessory lacrimal gland in the upper fornix. 3) Cysticercus and Hydatid cyst: These represent in the form of subconjunctival cyst. 4) Epithelial implantation cyst: Cysts are present at the site of injury or at the site of operation for strabismus.
Treatment
Excision or cauterization by thermal or laser.
Tumours
- Demoid, dermolipoma are the congenital.
- Papillae – are present in the patient wearing the contact lenses at the upper tarsal plate.
- Simple granuloma.
- Epithelioma (squamous cell carcinima).
- Pigmented tumours e.g. Naevi or conjunctival mole, precancerous melanosis, malignant melanoma.
- Rodent ulcer (Basal cell carcinoma)
- Dermoid: Lenticular yellow, commonly at the outer side, consist of epidermoid epithelium with sebaceous glands and hair. Tend to grow at puberty.
- Treatment: Excision with Tatooing or Lamellar graft.
- Dermolipoma: Fibrofatty tumour consists of fibrous tissue and fat. Present at outer canthus, not capsulated.
- Papilloma: Occurs at inner canthus, at the fornix or at limbus,may go to malignant stage.
- Epithelioma (Squamous cell carcinoma): Common at the limbus. Spread over the growth as early as possible the surface and in to fornixes. Rarely perforate the globe. Treatment – Removal, the base should be cauterized with diathermy. If it is confirmed by histopathological examination then Enucleation or Exenteration operation should performed.
- Pigmentary tumours: Naevi (congenital mole) – Grey gelatinous or pigmented nodule at the limbus. They are congenital tends to grow at puberty. Rarely become malignant. Treatment – Complete removal or excision before puberty.
- Precancerous melanosis: Diffusely spreading pigmentation of the conjunctiva rarely occur. Elderly people are affected, slowly spreading assume malignant characteristic giving rise to metastasis. Treatment – Widely excision of the globe with extentration of the orbit. Beta irridication after excision.
- Malignant melanoma: Occurs typically at the limbus is usually pigmented. Old patients are affected, spread over the globe but rarely penetrates. Treatment – Excision of the globe with exenteration of the orbit.
- Rodent ulcer (Basal cell carcinoma): Invade the conjunctiva from the inner canthus. The edges of the ulcer are raised and indurated, invade the conjunctiva from the lid. Rarely below the age of 40 years. Treatment – Exenteration of the orbit. If it is small excision with radio-therapy as it is sensitive to radium.
XEROSIS (DRY EYE)
It is a dry lusterless condition of the conjunctiva. This is due to the unstable tear film, exposing the conjunctival epithelium to evaporation. Tear film consists of three layers (Figs 1.7A to C): 1) Outer one is lipid layer – secreted by meibomian gland and zeis gland. 2) Aqueous layer – It is secreted by lacrimal and accessory gland. It consists of inorganic salts, lysozyme, lactoferrin and immunoglobulin. 3) Mucin layer – Secreted by goblet cells. Normal rate of tear production is 1 to 2 microlitre/minute.
Aetiology and classification:
- Decrease tear secretion–
- Lacrimal gland diseases, e.g.
- Autoimmune destruction – Sjögren's syndrome,
- Inflammation – Viral sarcoidosis,
- Block of excretary duct e.g. Steven Johnson's syndrome, ocular cicatrical pempigoid,
- Injury – Chemical injury, surgical damage.
- Systemic medication – Antihistaminics, Antihypertensive, psychotropics drugs.
- Reduced corneal secretion – Neuroparalytic keratitis
- Increased evaporation
- Lag-ophthalmous
- Meibomian gland destruction
- Contact lens wear.

Clinical Evaluation
Symptoms
Foregin body sensation or dry sensation
Burning sensation, photophobia, inability to read or to watch television for long time, bluring vision, decrease tearing in response to irritation or emotion.
Signs
- Blinking,
- Lid may be associated with trichiasis, blepharitis, irregular lid margin,
- Bulbar conjunctiva – increased debris and mucous strands lead to papillae, follicales and symblepharon.
- Palpebral conjunctiva – Superficial fibrosis, shortening of fibrosis.
- Corneal surface – Puncate-keratitis, irregular corneal surface, thinning or perforation of cornea.
- Systemic examination – Seborrhoric dermatitis, lupus erythematosus, salivary gland enlargement, Thyroid gland enlargement
- Mouth dryness
- Joints – Changes of rheumatoid arthritis are present.
Clinical Tests (Investigations)
- Schirmer test: It measures the rate of tear formation with the strip of Whatman filter paper of the size of 5 mm by 30 mm. Gently inserted strip at the lower fornix is wetted less than 5 mm after 5 minutes, it is diagnosed of +ve test (Normal range is 10 – 25 mm).
- Slitlamp examination
- Staining with fluorescein
- Tear lysozyme ratio is between 0.9 and 0.6 usually. Tear lysozyme is also reduced.
- Lacrimal and salivery gland biopsy – for diagnosis of Sjögren's syndrome.
- Goblet cell counts – are read from biopsy specimen of the deep tarsal portion of inferior nasal conjunctival fornix. Approximately normal goblet cells are 8/mm severely reduced goblet cells count are seen in mucin deficient states.
- Tear film break time – (BUT): One drop of fluorescein instilts in the eye and ask the patient to blink 2-3 times to disturb the dye. Then the eyelids of the patient open and then count the seconds until the apperance of a dry spot (fluorescein free area) appear black.
Normal BUT is 15 to 30 seconds or longer. Lesser time than this suggest the mucin deficiency. So mucinomimetic agent is the choice of treatment.
Management
- Tear replacement – Hypotonic solution as methylcellulose, polyvinyl alcohol. Dose – Every hour to bd as needed.
- Ocular insert – Hydroxy propil methylcellulose small units placed in the lower fornix and allow the day to dissolve to stabilize the tear film and lubricate the eye (5 mg rod is 4 mm in length can be used once, twice, thrice according to the need of the patient).
- Soft contact lens therapy.
- Punctal- occlusion – by – Cauterization
- Diathermy
- Silicon plug.
- Laser.
- Tear-stimulant
- Bromhexine - Orally 32 mg/day is given to stimulate tear production
- Cyclosporine tropical.
- Surgeries:
- Parotid duct transplantation
- Rectal mucous membrane graphs are tried, but the results are not satisfactory.