

2Some bony landmarks are subcutaneous and are seen (inspection), some are deep yet felt (palpation).
- Almost entire length of clavicle can be seen and palpated—first intercostals space lies below the clavicle.
- Tip of the coracoid process can be felt 2.5 cm below the junction of lateral one-fourth and medial three-fourth of the clavicle. Short head of biceps with coracobrachialis is attached here.
- Head of humerus, medial and lateral epicondyles at the lower end of humerus can be felt. Ulnar nerve is felt behind the medial epicondyle.
- Spine of the scapula can be easily felt on the upper part of back. It continues laterally in the acromion process. The root of the spine is at the level of spine of T3 vertebra.
- Tip of the acromion process can be easily felt lateral to the acromioclavicular joint. Length of humerus can be measured from lower border of acromion to lateral epicondyle.


- Hamilton's test—The bulky deltoid muscle gives rounded contour to the shoulder. If there is a dislocation of shoulder joint, the head of humerus is drawn inwards by pectoralis major, latissimus dorsi muscles, therefore, the ruler placed along the outer side of the arm can be in contact with acromion and lateral epicondyle at the same time. This is not possible in normal condition with rounded contour of the shoulder.

Olecranon process of ulna can be felt at the back of the elbow joint. Triceps is attached to its summit.
- The medial and lateral epicondyle along with olecranon process form the angles of an isosceles triangle in the flexed elbow. When the elbow is extended all three bony points lie in a straight line.


- The styloid process of ulna is felt at the same position in supinated forearm.
- The subcutaneous posterior border of ulna can be felt along the back of the forearm.
- Head of the radius can be felt at the back of the extended elbow, in a depression lateral to the olecranon process.
The head of radius rotates during the movements of pronation and supination.
- Head of metacarpals can be seen and felt more prominently dorsally when fingers are flexed. They are called knuckles.
- Dorsal tubercle of radius (Lister's tubercle) can be felt at the middle of the posterior aspect of lower end of radius, in the line of second interdigital cleft. On the medial side of the tubercle lies the tendon of extensor carpi radialis longus and on the lateral side is the tendon of extensor pollicis longus.
- When the wrist is fully flexed, well marked elevations on the dorsum are produced by bases of second and third metacarpals.
- Carpals—
- Scaphoid can be felt in the anatomical snuff box, distal to styloid process of radius.
- Pisiform is felt as a round bone of the palmar aspect, at the medial end of the crease between forearm and palm.
- Hook of the Hamate can be felt 1 cm distal and slightly medial to pisiform.
The flexor retinaculum is attached to the tubercle of scaphoid and ridge of trapezium laterally and to the pisiform and hook of Hamate medially.

- Anterior superior iliac spine can be felt at the lateral end of groin. The inguinal ligament and sartorius is attached to it. Its vertebral level is S1.
- Pubic tubercle is palpated at the medial end of the groin. Midway between two pubic tubercles is the pubic symphysis. Femoral hernia bulges below and lateral to pubic tubercle.
- Pubic crest is medial to pubic tubercle.

- Tubercle on the iliac crest lies 5 cm behind and above the anterior superior iliac spine. Its vertebral level is L5.
- Ischial tuberosity is the lowest bony part in sitting posture, it supports the body and transmits the body weight in sitting position. The Hamstring muscles are attached to the ischial tuberosity.
- Nelaton's line—The line joining the ischial tuberosity and anterior superior iliac spine of the same side is Nelaton's line used on X-rays. The highest point of greater trochanter of femur touches Nelaton's line.
- Ischial spine can be felt on per vaginal examination. It is used as a guideline for pudendal block.
- Posterior superior iliac spine cannot be felt, but its position is indicated by a depression on the medial side of buttock at the level of spinous tubercle of S2, 4 cm away from the midline.
- Greater trochanter is the lateral most bony point in the hip region. Its upper border lies a hand's breadth below the tubercle of the iliac crest.
- Patella can be seen and felt in front of knee joint. It is the largest sesamoid bone.


- Femoral condyles can be felt on either side of patella.
- Head of fibula is felt on lateral side of knee, following tendon of biceps femoris. The biceps femoris is attached here. Below the head lies the neck of fibula. The common peroneal nerve can be rolled over neck of fibula.
- Tibial condyles are felt in the depression on either side of ligamentum patellae.
- Tibial tuberosity is felt at the lower end of ligamentum patellae. At this level, the popliteal artery divides into anterior tibial and posterior tibial arteries.
- Anterior border of shaft of tibia (shin) is subcutaneous and can be felt throughout. The medial surface tibia is also subcutaneous almost throughout its extent. The long saphenous vein runs over the lower part of this surface.
- Medial malleolus is seen and felt on medial side of ankle joint. Long saphenous vein begins infront of the medial malleolus.
- Head of talus can be seen and palpated, 3 cm in front of the lower end of tibia, when foot is inverted passively when the toes are dorsiflexed, the head of talus is obscured by extensor tendons.
- Sustentaculum tali—the medial surface can be felt immediately below the tip of medial malleolus. On the undersurface of sustentaculum tali passes the tendon of flexor hallucis longus in a groove.
- Peroneal tubercle (trochlea) is felt when it is well developed, 2 cm below the tip of lateral malleolus.
The tendon of peroneus brevis tendon passes anterosuperior and tendon of peroneus longus passes posteroinferior to the peroneal tubercle.
- Tuberosity of navicular is felt 2.5 cm below and infront of the medial malleolus. It provides principal attachment for the tendon of tibialis posterior.
- Tuberosity of fifth metatarsal—present on the lateral side of base can be seen and felt halfway along the lateral border of foot. It gives attachment to peroneus brevis.

THORAX (FIG. 9)
- The plane of thoracic inlet is oblique. Posteriorly it passes between C7 and T10, anteriorly goes down and passes through suprasternal notch between T2 and T3.
- Suprasternal plane is horizontal, passes between T2 and T3.
- Counting of ribs, costal cartilage and intercostals spaces begins at sternal angle.
The costal cartilage and rib level with sternal angle is second. To count further one has to go downwards and laterally as the costal cartilages are crowded anteriorly and the intercostals spaces are narrow anteriorly.
The first costal cartilage lies behind the medial end of the clavicle.
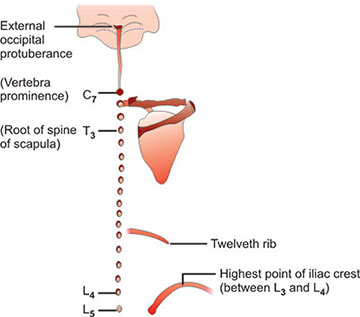
- Spines of vertebrae can be counted upwards or downwards from vertebra prominence (C7), however, spine of T1 may be as prominent as C7.
- T3 spine is level with root of spine of scapula.
- T7- Spine is level with inferior angle of scapula or little above it.
- Highest point of iliac crest lies between spines of L3 and L4.
- Tubercle of iliac crest is level with spine of L5.
ABDOMEN (FIG. 10)
- Xiphisternum can be felt in the epigastrium. The xiphisternal joint is at the level of 7th costal cartilage (between T9 and T10 vertebra).
- Linea semilunaris is the convex lateral border of rectus abdominis (with rectus sheath). It extends from the tip of 9th costal cartilage to pubic tubercle.
- For pubic tubercle, pubic crest, anterior and posterior superior iliac spines, refer to bony landmarks of inferior extremity.
- Spines of lumbar vertebra can be counted downwards from vertebra prominence (C7) or upwards from S2 (level with posterior superior iliac spine that lies in a dimple on medial side of buttock).
- The highest point of iliac crest, which is just behind its midpoint is at a level between L3 and L4. This landmark is used for lumbar puncture.
- Umbilicus usually lies between L3 and L4 vertebra. However, it is supplied by T10 spinal nerve through its ventral ramus.
- Nasion is the meeting point of frontonasal and internasal sutures. It can be felt at the root of nose in the midline.

- Glabella is the meeting point of two superciliary arches. Glabrous means devoid of hair.
- Superciliary arches are covered by eyebrows.
- Margins of the orbit are superior, medial, inferior and lateral.
- In the lateral margin frontozygomatic suture can be felt. It is used as a guide for the pterion.
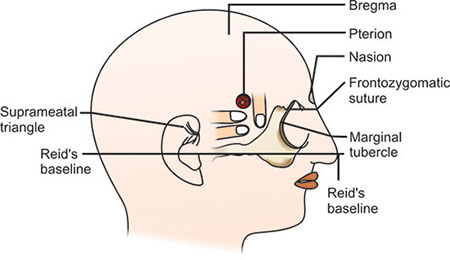
- Little below the frontozygomatic suture the marginal tubercle is felt.
- Reid's baseline passes through lower margin of orbit and center of external acoustic meatus. This line is horizontal in anatomical position of the skull.
- Frankfurt's plane passes through lower orbital margin and upper border of external acoustic meatus. According to some this plane is horizontal in the anatomical position of skull.
- Pterion is the area used to make burr holes to get an access to the interior, e.g. in case of head injury.
- It is at this point, anterior division of middle meningeal artery and vein are related, care should be taken not to injure these vessels. This area also corresponds to divergence of three rami of lateral sulcus from its stem and anterior pole of insula. Stem of lateral sulcus contains middle meningeal artery. The point of divergence of rami of lateral sulcus is called as Sylvian point.
- Suprameatal triangle lies above and little behind the tragus of external ear. It forms the lateral wall of mastoid antrum. The mastoid antrum can be approached through the suprameatal triagle. It is bounded by suprameatal crest anterosuperiorly, posterosuperior border of external acoustic meatus anteroinferiorly, and a tangent drawn to the curvature of posterior border of the external acoustic meatus (Fig. 13).
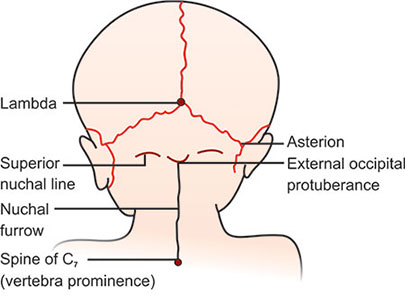
- External occipital protuberance can be felt posteriorly in the midline at the upper border of nuchal furrow. The most salient point on the protuberance is called inion.
- External occipital crest extends downwards from the external occipital protuberance. It can be felt with difficulty in the nuchal furrow, the ligamentum nuchae is attached here.

- Superior nuchal lines extend laterally from external occipital protuberance. They are slightly convex upwards. The trapezius is attached to the medial one-third of the lines and to the external occipital protuberance. The lateral part of the superior nuchal line gives attachment to sternomastoid muscle.
- Inferior nuchal lines are situated 2–3 cm below the superior nuchal lines. They extend laterally from external occipital crest (Fig. 14).24
- Mastoid process can be easily felt behind the external ear. The sternomastoid, longissimus capitis and splenius capitis are attached here.
- Angle of mandible can be seen and felt little below and infront of lobule of ear.
- Tip of transverse process of atlas (C1) can be felt midway between mastoid process and angle of mandible.
- Spines of cervical vertebrae can be felt and counted. The student should stand behind the subject and ask the subject to flex the neck. The prominent spine seen is that of C7 (spine of T1 could be equally prominent) from C7 count upwards till C2. The first cervical vertebra does not have the spine. The ligamentum nuchae is attached to the cervical spines.
- Condyle of manbile (Temporomandibular joint) is felt in front of tragus of ear. While closing and opening the mouth, movements can be felt here.
- Anteriorly, in the midline of the neck, following structures can be felt from above downwards.
- Symphysis menti.
- Laryngeal prominence (Adam's apple) formed by thyroid cartilage is felt and prominent to be seen also in males. It moves with deglutition.
- Ring of cricoid cartilage is felt below the laryngeal prominence.
- Suprasternal notch is felt between the medial ends of the right and left clavicles. The trachea can be palpated here.
BRAIN
- Nasion, inion, pterior, marginal tubercle, etc. have been given with landmarks of Head, Face and Neck.
- Bregma is the meeting point of coronal and sagittal sutures. The anterior fontanelle is situated here. It closes by about 18 to 24 months. Anterior fontanelle is used to know the intracranial pressure as a clue to hydration of babies. Certain medication can be injected here.
- Lambda is the meeting point of sagittal and lambdoid sutures. It is situated about 5 cm above the inion. The posterior fontanelle situated here closes by about 3 months.