

“Listen to what patients are saying Because they are telling you the diagnosis”
The history, physical examination, electrocardiogram and chest radiography are the keystones for the diagnosis of cardiac problems in children. With each technique, different aspects of the cardiovascular system are viewed, and by combining the data derived, a fairly accurate assessment of the patient's condition can be obtained.1 More sophisticated techniques, such as echocardiography and cardiac catheterization, permit detailed patient evaluation.
Symptoms of congenital cardiac disease are protean, sometimes subtle and may manifest anytime from fetal period to adulthood (Table 1.1).
Many aspects of the history are age specific and therefore, historical information should be obtained from both parents and the child.
GESTATIONAL AND NATAL HISTORY
Exposure to possible teratogens may provide important etiological clues (Table 1.2). Increasingly, infants are being born having a fetal cardiac scan and one must always enquire into the indication with special emphasis given to an abnormal scan. Complications such as toxemia, birth asphyxia, fetal distress, and low birth weight may result in perinatal insult to the myocardium and persistent pulmonary hypertension.
| |||||||||||||||||||||||
Clinical differentiation from CHD may be difficult and usually requires an echocardiographic evaluation.2
MATERNAL CONDITIONS
There is a high incidence of reversible ventricular hypertrophy in infants born to diabetic mothers. Additionally, these babies have structural heart diseases such as transposition (TGA), ventricular septal defect (VSD) and patent ductus arteriosus (PDA).
Systemic lupus erythematosus (SLE) and mixed connective tissue disorders in the mother increase the risk of congenital complete heart block. However, most mothers of infants born with congenital complete heart block have no symptoms of SLE. A history of frequent abortions in previous pregnancies may be obtained. Maternal history of congenital heart disease increases the incidence of CHD in offspring from 1 to 15%.
BIRTH HISTORY AND WEIGHT
Prematurity is a clue more to presence of noncardiac especially respiratory disease, but may point to cardiac disease (PDA). Prematurity influences the rate of regression of pulmonary vasculature and premature infants with left-to-right shunts tend to present with heart failure at a relatively younger age. Birth weight can alert to a syndrome, for example, in congenital rubella the child is small for gestational age and in maternal diabetes the child is large for gestational age. Birth asphyxia is associated with both persistent pulmonary hypertension and myocardial dysfunction.
FAMILY HISTORY
A family history of sudden death and a structural or functional cardiac abnormality in a first degree relative may have diagnostic relevance. Family history is also important to prognosticate recurrence risks and also that many inherited or genetically determined conditions have cardiac components, e.g. Noonan's syndrome, Familial long QT-interval or Duchenne's dystrophy. In hypertrophic cardiomyopathy, there is evidence of more than 20% higher incidence 3of inheritance in first degree relatives, thus, meriting consideration of an echocardiographic screening of relatives. The family history should identify the presence of early myocardial infarction and hypercholesterolemia that may prompt cholesterol screening.
POSTNATAL HISTORY
The time at which signs and symptoms of heart disease begin may indicate the type of cardiac lesion. Most newborns are asymptomatic at birth and as perinatal changes are completed, symptoms specific to physiology of the defect becomes evident, e.g. ductal dependent left or right sided obstructive lesions present in the first week of life as the ductus arteriosus closes. In the former group of lesions this results in decrease in cardiac output and signs of shock children. Commonly, murmurs detected in the neonatal period are because of atrioventricular valve (AV) regurgitation. The significant left-to-right shunts present around 4 weeks of age, when pulmonary vascular resistance decreases and heart failure ensues. The three most common postnatal presentations are cyanosis, respiratory difficulty and murmur.
Cyanosis, “Cyanotic Spells” and Squatting
Cyanosis is a bluish or purplish color of the skin, lips or mucous membrane caused by the presence of at least 5 g/dL of reduced hemoglobin. Central cyanosis must be distinguished from peripheral or acrocyanosis; the latter is usually confined to nail beds and perioral skin and occurs when the child is exposed to hypothermia. A distinctive feature of central cyanosis is that it worsens with activity and increasing cardiac output while acrocyanosis often improves. Cyanosis in association with cardiac murmur strongly suggests a structural heart lesion. Children in shock may also appear cyanosed because of venous stasis. Episodic central cyanosis may be a sign of cardiac disease as in hypercyanotic spell or of respiratory or neurological disorders such as asthma, apnea and fits. The true hypercyanotic spells are seen in infants with TOF and require immediate attention. The precipitating factors, duration of spell and its frequency should be enquired into. In a true spell, the child would be breathing fast as compared to a child with breath holding spell that would be apneic. A typical spell is characterized by a sudden increase in intensity of the cyanosis, at times associated with loss of consciousness. Special enquiry must be made as to whether the child squats when tired or has a favorite position of comfort (knee-chest) when tired. In this position, the systemic arterial resistance rises, the right-to-left shunt decreases and patient becomes less desaturated.3
Tachypnea, Dyspnea
The infant's breathing patterns should be documented which may be: (1) tachypnea with abnormally rapid respirations. This is often seen in cyanotic heart disease with low cardiac output and usually associated with a compensatory rapid respiratory rate, particularly on exertion, because of diminished peripheral oxygenation or (2) grunting and dyspnea with difficult breathing. Dyspnea or labored breathing is also often present in patients with pulmonary congestion from either left sided cardiac failure; conditions raising the pulmonary venous pressure or from marked hypoxia. Increased pulmonary venous pressure causes 4increased stiffness of the pulmonary vessels and transudation of fluid into the interstitial tissue, making the lungs less compliant. The child works harder to breathe. Wet, stiff lungs encourage secondary infection; respirations become rapid, the accessory muscles come into use, and subcostal indrawing is observed. Older children complain of shortness of breath. Occasionally, wheezing or cough could suggest CHF. Tachypnea also leads to poor feeding and weight gain. A sleeping respiratory rate more than 40/min in children and 60/min in neonates is significant.
Frequent Respiratory Infections
Congenital heart with large left-to-right shunts and increased pulmonary blood flow predispose to frequent lower respiratory tract infections (LRTIs). Compression of the airways by plethoric vessels may contribute to stasis and atelectasis and predispose children to LRTIs.
Weight Gain, Development and Feeding Pattern
In young infants, metabolic demands are usually greatest during feeds. The infant with poor peripheral oxygenation because of low cardiac output will tire easily during feeds, the equivalent of exercise in older children. As a result of fatigue, the infant is unable to take a full feed. In addition, rapid respiration diminishes the time available for swallowing. This combination of factors results in failure to gain weight. In the baby with a large left-to-right shunt, the process is exaggerated by the increased caloric needs of an overworked myocardium. Increased sympathetic activity causes excessive perspiration–often a valuable diagnostic feature. Any baby with this clinical presentation of suck-rest-suck cycle has congestive heart failure until proved otherwise. When a young baby tires rapidly, sweats during feedings, and has subcostal indrawing, always think of the possibility of left sided cardiac failure.4
Exercise Intolerance
Decreased exercise intolerance is usually seen in large left-to-right shunt lesions, cyanotic defects, valvular stenosis or regurgitation and arrhythmias. Enquiries regarding exercise intolerance should be age relevant and in very small infants should include feeding patterns, easy fatigability or resting after minimal feeding may give a clue to CHF. In older infants history must include the ability to climb stairs or walk for extended periods. In older children, a comparison with peer sporting interactions, level of function in physical education, and index of aerobic ability should be sought.
Puffy Eyelids and Peripheral Edema
Puffy eyelids and sacral edema are signs of systemic venous congestion. Ankle edema is not usually found in infants. Pretibial and presacral edema are late developments in the child's congestive circulatory failure picture, apparently because of difference in tissue turgor. When peripheral edema because of heart failure does develop in an infant, it first appears periorbitally, usually preceded by other manifestations such as tachypnea, tachycardia, dyspnea, and liver enlargement and suggests right heart failure.5
Heart Murmur
An enquiry into the timing of discovery of heart murmur may be relevant. Aortic stenosis, pulmonary valvular stenosis, small VSDs, PDAs and atrioventricular regurgitation manifest with murmur a few hours to a few days after birth. Many instances of tetralogy of Fallot (TOF) are often identified soon after birth because of a systolic murmur. These infants are often initially pink and cyanosis appears later as the pulmonary stenosis worsens. The murmur of large left-to-right shunts usually presents beyond 4 weeks with regression of pulmonary pressures. A febrile illness usually unmasks a heart murmur.5,6
Chest Pain
Chest pain is a benign symptom in older children and adolescents. Chest pain rarely occurs with cardiovascular disease and the common noncardiac causes are musculoskeletal, gastroesophageal reflux, anxiety and respiratory causes (asthma, pleuritis, bronchitis, pneumonia). Cardiac conditions that may cause chest pain include severe aortic and pulmonary stenosis, pulmonary vascular obstructive diseases, mitral valve prolapse, pericarditis, myocarditis and Kawasaki's disease. Chest pain may also be experienced with very rapid paroxysmal tachycardias and has been recognized in infants with an aberrant left coronary artery (ALCAPA). 7
Palpitations
Palpitations is the subjective feeling of rapid or forceful heartbeats or irregular heartbeats and is common in school aged child and adolescents. Palpitations usually occur concurrently with chest pain. In children with MVP, palpitations may be the presenting symptom.
Neurologic Symptoms
Syncope: Transient loss of consciousness and muscle tone that result from inadequate cerebral perfusion. Dizziness is the most common prodromal symptom of syncope. These complaints could represent a serious cardiac condition that may result in sudden death because of life-threatening arrhythmias or conditions such as MVP, hypertrophic cardiomyopathy or severe aortic stenosis. Syncope could be because of noncardiac causes (such as benign vasovagal syncope), neuropsychiatric conditions, and metabolic disorders. Left ventricular outflow tract obstruction (e.g. aortic stenosis or hypertrophic cardiomyopathy) commonly causes effort syncope, whereas syncopal episodes because of dysrhythmias can occur either at rest or during activity.
A history of stroke suggests embolization or thrombosis, secondary to cyanotic CHD with polycythemia or infective endocarditis. A history of headache may be a manifestation of cerebral hypoxia with cyanotic heart disease, severe polycythemia, or brain abscess. Hypertension with or without coarctation rarely causes headache in children.8
Medications
Physicians should note the timing, dosage, compliance and duration of cardiac and noncardiac medications. Tachycardia may be produced by aminophylline, antihistamines and related drugs.6
Joint
Joint pains, swelling may be seen in children with rheumatic fever, systemic diseases, infective endocarditis and children with Eisenmenger's syndrome.
Disease Impact
History of disease impact on child especially growth and development, schooling, sports, sibling and family is also important.
Previous Evaluations and Records
It is important to ascertain whether the patient was evaluated previously for suspected heart disease. Previous records may provide important insights into the natural history of the underlying condition. For example, a subpulmonic VSD may progress to have aortic valve prolapse and aortic regurgitation at a later age.
Age at presentation of clinical signs gives a clue to underlying CHD.9
- If congestive cardiac failure develops solely because of CHD then symptoms usually arise before 3 months. Heart failure is rarely present at birth as the fetal circulation is in parallel and there are communications between the two sides. When there is obstruction on one side, blood flows easily to the other. As the fetal lungs are collapsed, increased pulmonary blood flow does not occur in utero.
- Heart failure that develops during the first week of life, especially in the first 3 days, is usually because of an obstructive lesion or to persistent pulmonary hypertension.
- Heart failure that develops at 4 to 6 weeks of age is invariably due to left-to-right shunting through a defect (volume overload). Pulmonary resistance usually nadirs at around 4 weeks of age, allowing left-to-right shunting to reach a maximum.
- If heart failure develops after 3 months of age, additional causes must be kept in mind, such as myocarditis, cardiomyopathy, or paroxysmal tachycardia.
- Central cyanosis because of congenital heart disease may be present at birth or may appear first when the ductus closes off, usually by 5 days of age. In tetralogy of Fallot, it may develop later (2 months of age or older) when the infundibular stenosis becomes more severe, increasing the volume of right-to-left shunting.
PHYSICAL EXAMINATION
Developing an organized routine in the performance of cardiac examination is necessary so as to not miss the important signs. The cardiac examination consists of vital signs assessment by inspection, palpation and auscultation.
Overall Appearance
A general assessment would reveal the child to be well or sick. The sick infants often appear anxious, fretful, diaphoretic, pale, or breathless and are seldom consolable.
An assessment of child's overall growth, appearance and state of distress serve to guide the urgency of further investigations and management. The height and weight should be measured 7and plotted on a standard growth chart that would aid in determining the presence of failure to thrive.
Different patterns of growth impairment are seen in various types of CHD.
- Acyanotic patients, particularly those with a large left-to-right shunt, with or without pulmonary edema and/or ventricular dysfunction tend to have cardiac malnutrition with weight being more affected than height and degree of weight impairment proportional to the size of the shunt.
- Acyanotic children with pressure overload lesions without intracardiac shunts grow normally.
- Cyanotic patients have disturbances in both (usually height more evident than weight).
Infants should gain about 20 g/day; Those with impaired growth would need adjustment of medications (diuretics, digoxin, correction of anemia if present) and use of caloric-supplemented food. If these methods are insufficient, surgical catheter interventions may be necessary.
It should be remembered that poor growth in a child with a mild cardiac anomaly or failure of catch-up weight gain after repair of the defect may indicate failure to recognize certain genetic syndromes or associated noncardiac deformities.
Evidence of pallor, clubbing, edema, pattern of respiration, sweating and dysmorphic features must be looked for in general examination. Clinical cyanosis is evident only when the oxygen saturation is below 85%. The presence of cyanosis should therefore be ascertained with pulse oximeter in all with suspected CHD. If cyanosis is present, the degree and distribution should be additionally noted. In differential cyanosis, the upper half of the body is pink and the lower half blue, or vice versa. Systemic-level pulmonary vascular resistance and a patent ductus arteriosus need to be present for this phenomenon to occur. The oxygen saturation can be higher in the upper extremity in patients with normally related great arteries if there is right-to-left shunting at the level of the ductus arteriosus (as seen in infants with either persistent pulmonary hypertension of the newborn, severe coarctation of the aorta, or interrupted aortic arch). The differential effect is reduced if there is also right-to-left shunting at the level of the foramen ovale, or if there is left-to-right shunting across a coexisting ventricular septal defect.10
The lower portion of the body can be more cyanotic than the upper segment in older patients with Eisenmenger syndrome caused by a persistent large patent ductus arteriosus.
Clubbing: Reddening and shininess of the terminal phalanges are seen in the early stages of clubbing and most noticeably in the thumb. Presence of clubbing represents chronic arterial desaturation of at least 3 months duration. When fully developed, clubbing is characterized by a widening and thickening of the ends of the fingers and toes as well as by convex finger nails and loss of angle between the nail and nail bed. With marked clubbing, the terminal phalange becomes bulbous. Clubbing may also be associated with lung disease (e.g. abscess), cirrhosis of the liver, and subacute bacterial endocarditis. Occasionally, clubbing without cyanosis occurs in healthy people, as seen in familial clubbing.
Edema
Pitting edema indicates systemic congestion and is unusual in children with CHD. In older children edema can be caused by cardiac dysfunction or may be noted after Fontan procedure 8because of protein-losing enteropathy, a complication that occurs with high venous pressure. Swelling of the face, neck, and arms can occur with superior vena cava obstruction, post-palliative surgery for CHD, intravascular thrombosis associated with an indwelling central venous catheter, or obstructing mediastinal mass. Obstruction of the inferior vena cava or iliac or femoral veins occasionally occurs secondary toin uterothrombosis or as a complication of catheterization and can produce edema of the abdomen and lower extremities. Nonpitting swelling of the hands and feet represents lymphedema and may be seen in infants with Turner's syndrome.
Extracardiac anomalies should be looked for in all children with congenital heart disease. Multiple syndromes have characteristic facies. A webbed neck and short stature suggest Turner's syndrome. Arachnodactyly, pectus deformity, scoliosis, and arm span exceeding height are features of Marfan syndrome. Radial dysplasia is a component of Holt-Oram syndrome.
Heart Failure
Children with CHD with a low cardiac output and high pulmonary venous pressure would have sufficient underlying hemodynamic disturbances to have clinical manifestations. The precordial bulge noted in these children is because of underlying cardiac enlargement of at least 3 months duration. Additionally, tachycardia, tachypnea, dyspnea, poor weight gain, flaring of the inferior rib cage with subcostal indrawing and Harrison's groove (line of depression in the bottom of the rib cage along the attachment of the diaphragm) could be noted and indicate poor lung compliance of long duration as seen with large left-to-right shunt lesions. Infants with CHF often have a cold sweat on the forehead and represents a heightened sympathetic activity as a compensatory mechanism for decreased cardiac output.11
CARDIOVASCULAR ASSESSMENT
Vital Sign Assessment
Vital signs should be recorded for each patient.
Pulse Characteristics
The pulse is examined with respect to rate, rhythm, volume and character.
Sinus tachycardia occurs in a variety of conditions, including anxiety, fever, pain, anemia, large left-to-right shunts, decreased cardiac contractility, cardiac tamponade, sepsis, pulmonary disease, or hyperthyroidism. Supraventricular tachycardia in infants or children typically occurs at a rate that is too rapid to count by an observer (more than 220 beats/minute). Bradycardia is seen in athletes, hypothyroidism, or heart block.
Normal resting heart and respiratory values for age are presented in Table 1.3.
|
Rhythm: A phasic variation related to the respiratory cycle (faster during inspiration) is characteristic of sinus arrhythmia. Occasional premature beats can represent atrial, ventricular, or junctional premature beats. Nonconducted atrial premature beats are the most common cause of a “pause” in the neonatal period and usually resolve during the first month of life. Isolated ventricular premature beats are common in adolescence; resolution with exercise suggests a benign etiology.
Volume: The dynamic character of the pulse may provide information about the cardiac output. Clinical information of cardiac output includes the warmth of the digits and measured capillary refill time that is usually 2 to 3seconds. Bounding pulses are present in febrile states, hyperthyroidism, exercise, anxiety, severe anemia and with aortic runoff lesions that produce increased pulse pressure (aortic regurgitation, patent ductus arteriosus, arteriovenous malformations, aortopulmonary window, truncus arteriosus). The prominent pulse which is classically associated with aortic regurgitation has been termedCorrigan's pulseorwater hammer pulse. This high runoff conditions produce visible ebbing and flowing of the capillary pulse that can be observed by partially compressing the nail bed, a phenomenon termed Quincke's sign.
Generalized decreased intensity of pulses is associated with low cardiac output. This can be caused by acquired heart disease such as myocarditis, cardiomyopathy or obstructive lesions, pericardial tamponade or constrictive pericarditis. Pulses may be absent or decreased in Takayasu's arteritis, that is a rare form of vasculitis affecting the large arteries (also termed as pulseless disease).
A weak, thready pulse is found in cardiac failure or circulatory shock. The radial and brachial pulses should be assessed simultaneously in the upper limb. By palpating the pulse on two sites and altering the pressure applied by the palpating fingers, a more accurate assessment of the rate of arterial pressure rise, volume and contour may be obtained.
The radial pulse should also be compared with the femoral to feel for any delay that may be seen in coarctation of the aorta. The presence of a palpable femoral pulse may not always rule out coarctation because collateral vessels may perfuse the lower limbs. Previous arterial instrumentation, injury or congenital variability may account for a reduction in palpable peripheral pulses. In Takayasu's arteritis, segmental affection of aorta may result in differences in volume of extremity pulses depending on site of affection. A systemic–to–pulmonary artery shunt (either classic Blalock-Taussig shunt or modified Gore-Tex shunt) or subclavian flap angioplasty for repair of COA may result in an absent or weak pulse in the arm affected by surgery.
Variation: In pulsus paradoxus, an exaggerated decrease in inspiratory systolic pressure of more than 10 mm Hg is noted and is seen with pericardial tamponade or severe respiratory distress. Pulsus alternans consists of a decrease in systolic pressure on alternate beats and indicates severe left ventricular dysfunction and can be easily appreciated observing intravascular blood pressure recordings. Pulsus bisferiens consists of a pulse with two peaks separated by a plateau and can occur in patients with either hypertrophic obstructive cardiomyopathy or large left ventricular stroke volume.10
Venous Examination
The jugular venous pulse is generally difficult or impossible to assess in infants and young children. In them, the liver character and size are more reliable indicators of systemic congestion. The congested liver margin is rounded, firm and tender. In a cooperative child or adolescent, venous pressure can be estimated by examination of the jugular vein. When the patient is sitting or reclining at a 45° angle, the jugular vein should not be visible above the level of the clavicle. Measuring the difference in the height of the jugular vein with a parallel line drawn through the level of the manubrium yields central venous pressure.
Prominent jugular venous waves are present in normal atrial contraction into a stiff right ventricle or against a closed tricuspid valve (tricuspid atresia; complete heart block, tricuspid regurgitation, pericardial disease (pericardial tamponade, constrictive pericarditis), vein of Galen malformation and superior vena cava obstruction. Splenic enlargement in CHF is unusual.
Blood Pressure Measurement
Blood pressure measurement can be difficult and time-consuming, but is an essential part of cardiovascular system assessment. It is recommended that the bladder width of the blood pressure cuff is approximately 40% and the bladder length is approximately 80% of the arm circumference midway between the olecranon and the acromion. The inflatable bag should thus ideally cover two-thirds of the full length of the arm. The equipment necessary to measure blood pressure in children 3 years of age through adolescence includes pediatric cuffs of different sizes. For newborn—premature infants, a cuff size of 4 × 8 cm is recommended; for infants, 6 × 12 cm; and for older children, 9 × 18 cm. A standard adult cuff, a thigh cuff for leg blood pressure measurement and cuffs for use in children with very large arms are also available.13
In general, blood pressure obtained by palpation or flush technique is significantly less accurate than auscultation. The systolic pressure is recorded as the first audible Korotkoff sound, with the diastolic pressure correlating best with muffling phases or fourth Korotkoff sound. Increasingly, automated oscillometric methods allowing digital print outs of systolic, mean and diastolic pressures are being used for blood pressure measurements. The upper and lower limb blood pressures should be recorded at least on one occasion in child's life. The calf cuff application to the thigh and Doppler assessment of popliteal systolic pressure can be easily performed. The lower extremity systolic pressure can be 5 to 10 mm Hg greater than the upper extremity value because of the standing wave effect, with successive heartbeats adding to the pressure downstream. If systolic pressure in the upper extremity is more than 10 mm Hg than in the lower extremity, it strongly suggests presence of coarctation of the aorta. The blood pressure measured should be compared with normal values for age and sex of the child (Figs 1.1A to D). Tables are available that provide the systolic and diastolic blood pressure level at the 95th percentile according to age, sex, and height.14 Hypertension in children and adolescents is defined as systolic and/or diastolic blood pressure that is consistently equal to or greater than the 95th percentile of the blood pressure distribution. The pulse pressure is the difference between systolic and diastolic values. The pulse pressure is increased in conditions associated with bounding pulses and decreased in states associated with diminished pulses.


Figures 1.1A to D: (A,B) Age-specific percentiles of BP measurements in boys and girls respectively—birth to 12 months of age. (C, D) Age-specific percentiles for BP measurements in boys and girls respectively—1–13 years of age(From National Heart, Lung, and Blood Institute, Bethesda, D: report from second task force on blood pressure control in children, 1987)13
Respiratory Assessment
A review of respiratory system should be a part of the assessment of cardiovascular examination. The rate, depth, effort of respiration, evidence of air trapping, increased chest diameter, or 12presence of Harrison's sulci should be noted. Infants with heart failure often have labored efforts and tend to use their accessory muscles of respiration quite prominently.
Tachypnea is present with pulmonary parenchymal disease, pulmonary edema, large left-to-right shunts that elevate pulmonary venous pressure, and conditions causing metabolic acidosis. The normal respiratory rate at different ages is mentioned in table 1.3. Quiet tachypnea is often present in left-to-right shunt lesions, while labored tachypnea is observed with pulmonary disease. Both can be accompanied by intercostal or subcostal retractions, flaring of the alae nasi, or audible wheezing. Orthopnea is pathognomic sign of left ventricular dysfunction or severe elevation in pulmonary venous pressure.
PRECORDIAL EXAMINATION
Inspection
A visible apical impulse can be seen in left ventricular volume overload lesions, including large left-to-right shunts and significant mitral or aortic regurgitation. A visible parasternal impulse is associated with right ventricular overload lesions, including tetralogy of Fallot, absent pulmonary valve associated with severe pulmonary regurgitation or severe tricuspid regurgitation associated with Ebstein's anomaly, and large arteriovenous malformations.6 Harrison's groove, a line of depression in the bottom of the rib cage along the attachment of the diaphragm, indicates poor lung compliance of long duration such as that seen with large left-to-right shunts. Substernal thrust indicates the presence of right ventricular enlargement, whereas, an apical heave is noted with left ventricular hypertrophy. A hyperdynamic precordium suggests a volume load such as that found with a large left-to-right shunt, although it may be normal in a thin patient. A silent precordium with a barely detectable apical impulse suggests pericardial effusion, severe cardiomyopathy, Fallot's tetralogy or may be normal in an obese patient.
Palpation
The chest should be palpated for: apical impulse, point of maximum impulse (PMI), hyperactivity of the precordium, and palpable heart sounds and thrills. In general, if apical impulse is not palpable and if the pulses are of normal volume, then in most probability, the child does not have a serious hemodynamic disturbance.15
- Apical impulse: The location and character of apical impulse should be noted. The apical impulse is best appreciated using the tips of the index and middle fingers and is normally located in the left midclavicular line in the fourth or fifth intercostal space. The apical impulse is displaced laterally and is more prominent in left ventricular overload lesions such as severe aortic or mitral regurgitation or lesions associated with large left-to-right shunts at the ventricular or great vessel level. The right ventricular impulse is best detected by placing the hand on the chest with the heads of the metacarpals along the left costochondral junctions. A prominent lift indicates right ventricular hypertension or right ventricular volume overload. The right ventricular impulse can also be assessed in the epigastric area under the xiphoid process; the tips of the fingers can easily palpate 13the right ventricular impulse. However, the specificity of this pattern is rather limited. Right-sided apical impulses signify dextrocardia, tension pneumothorax, or left-sided thoracic space-occupying lesions (e.g. diaphragmatic hernia), left lobar emphysema, or scimitar syndrome. The character of the apical impulse is a useful guide to the underlying physiology. LV volume overload such as that which occurs with large VSD, mitral or aortic regurgitation results in a hyperdynamic apex. Here the apex is forceful but the outward movement occupies < 50% of the cardiac cycle. Obstructive lesions in the left ventricular outflow result in a sustained heave (> 50% of the cardiac cycle) and are often accompanied by a presystolic impulse (S4) which is slow rising heaving apical impulse. If impulse is well localized and sharp rising, it is called a tap and is noted in mitral stenosis. Heaving apex is classically seen in pressure overload conditions that result in ventricular hypertrophy (aortic stenosis, systemic hypertension, etc.). This is a forceful and sustained apex that is usually localized. Hyperdynamic apex is classically seen in volume overload conditions where there is ventricular dilatation (aortic regurgitation, hyperdynamic circulation, etc.). This is a forceful, but ill-sustained apex that is palpable over a larger area than normal (diffuse), i.e. more than one intercostal space.16
- Point of Maximal Impulse: Site of maximal impulse helps to determine that of the ventricles are enlarged. With RV dominance, the impulse is maximal at the lower left sternal border or over the xiphoid process and would be heaving in character if the RV systolic pressure is elevated; with LV dominance, the impulse is maximal at the apex. Systolic pulsations in the left second intercostal space suggest pulmonary hypertension or rarely, a L-posed aorta of corrected transposition. Suprasternal pulsations suggest enlargement of the ascending aorta.
- Palpable heart sounds: A palpable second heart sound usually indicates severe pulmonary hypertension but can also be present in conditions in which the aorta has an anterior location, such as transposition of the great arteries. A palpable first heart sound can be present in hyperdynamic states. The third and fourth heart sounds are often better felt than heard because of their low frequencies.
- Precordial Thrills: These are best identified by palpation with the palmar surfaces of the metacarpophalangeal and proximal interphalangeal joints of the examiner's hand. Thrills are vibratory sensations that represent palpable manifestations of loud, harsh murmurs (grade IV) and are located in the same areas as maximum intensity of the murmur. The timing and location of thrills should be noted. Systolic thrills at the left lower sternal border usually are caused by small ventricular septal defects and occasionally tricuspid regurgitation, if there is right ventricular hypertension. Mitral, aortic, and pulmonary thrills are located at the apex, right upper sternal border, and left upper sternal border, respectively. A thrill in suprasternal notch should arouse suspicion of aortic stenosis, coarctation or less commonly pulmonary stenosis and indicate significant degrees of obstruction. In patent ductus arteriosus or aortic insufficiency, the suprasternal notch is very pulsatile. Although most thrills occur in systole, diastolic thrills can occur at the apex with mitral stenosis, or along the left sternal border with aortic or pulmonary regurgitation.17
Percussion
In general, percussion of the heart in children is of negligible diagnostic value.
Auscultation is an art that improves with practice and provides perhaps the most useful diagnostic information. The precordium should be listened to in the four cardinal areas and the back with both bell and diaphragm, the former better suited for detecting low-frequency events, while the diaphragm selectively picks up high frequency events. It is important to be systematic so that all available data are collected and a reliable diagnosis is made. It is also important to listen to one sound at a time. The components to be evaluated include the heart sounds (S1, S2, S3, S4), ejection click, opening snap, pericardial rub, and murmurs (systolic, diastolic, continuous). The patient should be evaluated in more than one position, including supine, sitting, and standing, depending on the diagnosis, because some heart sounds change or are more easily appreciated with different patient posture.18
- Heart rate and regularity: Extremely fast or slow rates or irregularity in the rhythm should be evaluated by an ECG and a long rhythm strip.
- Heart sounds: Intensity and quality of the heart sounds, especially the second heart sound (S2) should be evaluated. Abnormalities of first, third and presence of gallop rhythm or the fourth sound (S4) should be noted. Systolic or diastolic sounds (e.g. an ejection click in early systole and midsystolic click) provide important clues to diagnosis.
- Heart murmurs: Heart murmurs are caused either by turbulence in blood or tissue vibration.
Heart Sounds
First heart sound (S1): This represents closure of the mitral and tricuspid valves and occurs when the ventricular pressure exceeds the atrial pressure at the onset of systole. Splitting of the first sound is normal as mitral valve closes earlier than the tricuspid. The intensity of first heart sound is decreased in low cardiac output states, prolonged atrioventricular conduction and in myocardial diseases. It is accentuated with increased blood flow across atrioventricular valve as in left-to-right shunts or in high cardiac output states and in mitral stenosis. Patients with complete heart block have variable intensity of S1.
Second heart sound (S2): S2 is produced by closure of the semilunar valves and is typically best appreciated at the left upper sternal border. The quality of S2 yields important information on cardiac physiology, particularly in a child with cardiac malformation. The second heart sound has two components that represent the asynchronous closure of the aortic and pulmonary valves and signal the end of ventricular ejection. Aortic closure (A2) normally precedes the closure of pulmonary valve (P2) because right ventricular ejection is longer. The time interval between the components varies with respiration, i.e. with inspiration, the degree of splitting increases and with expiration, it shortens. This variation is because of greater volume of blood that returns to the heart during inspiration, and longer time taken for ejection of this augmented volume of blood. Detecting splitting of S2 is always challenging. If the split is easily detected, the split is often wide. In infants with tachycardia and tachypnea, correlating S2 with the respiratory cycle is impossible. The best the examiner can do is to detect variability with a split present in some beats and not in others. Table 1.4 shows the conditions with abnormal S2.
A widely fixed split S2 occurs with right ventricular volume overload lesions, the most common of which is atrial septal defect and less with total or partial anomalous pulmonary venous connection or large arteriovenous malformation. In these conditions, the persistent right ventricular volume overload delays pulmonary valve closure so that the split is wider. Wide inspiratory splitting can also be noted with right bundle branch block, pulmonary stenosis, or idiopathic dilation of the main pulmonary artery due to prolonged contraction of the right ventricle and also with significant mitral regurgitation (due to earlier closure of the aortic valve). Paradoxical splitting is uncommon in children and difficult to appreciate.
The intensity of S2 depends on the pressure closing the semilunar valves and the anterior-posterior position of the great arteries. The most common cause of a loud S2 is pulmonary hypertension. Pulmonary hypertension can be caused by increased pulmonary flow or elevated pulmonary vascular resistance; evaluation of murmurs often helps to distinguish between these two mechanisms, with the former being associated with diastolic rumbles across the atrioventricular valve that receives increased flow. Increased intensity of S2 is also present in patients with transposition of the great arteries because of the anterior location of the aorta, and often in tetralogy of Fallot. S2 is single in patients with severe pulmonary hypertension and when there is atresia of one the semilunar valves.
Third heart sound (S3): This is normally heard in many children and is accentuated in pathological states and best heard with the bell of the stethoscope. This sound occurs early in diastole and represents the transition from rapid to slow filling phases. Cardiac diseases associated with a third heart sound include myocardial dysfunction or volume overload conditions as seen with an increased blood flow across either the mitral valve (as in VSD or MR) or through tricuspid valve (as in atrial septal defect). A third heart sound produced by the left ventricle is detected in the apical region, whereas that from the right ventricle is noted at the left lower sternal border. A gallop rhythm found in congestive cardiac failure often represents exaggeration of the third heart sound in the presence of tachycardia. Left ventricular enlargement and dysfunction that accompanies cardiomyopathy, anomalous coronary artery from pulmonary artery (ALCAPA) characteristically has a prominent S3 and is accompanied by a soft S1.
Fourth heart sound (S4): This is abnormal and is produced by atrial contraction in late diastole and is best heard with the bell of the stethoscope. S4 is seen in conditions with decreased ventricular compliance so that increased atrial contractile force is required to fill the ventricle as occurs with myocardial fibrosis, hypertrophic cardiomyopathy, systemic hypertension, and valvar aortic or pulmonary stenosis. When both an S3 and S4 are present, there is a quadruple rhythm. In such a situation, if there is tachycardia and resulting shortening of diastole, the two extra sounds may become superimposed and create a summation gallop.19
Heart Murmurs
Heart murmurs should be evaluated in terms of intensity, timing, location, transmission and quality.20
- Intensity (loudness): The intensity of a murmur is graded on a scale of 1 through 6. Murmurs grade 4 or greater are associated with a palpable thrill. The loudness depends on both the 16pressure gradient and the volume of blood flowing across the site creating the murmur. Murmur is graded as follows:
- Grade 1 : Heard only with intense concentration
- Grade 2 : Faint but heard immediately
- Grade 3 : Easily heard, of intermediate intensity
- Grade 4 : Easily heard and loud (associated with a thrill)
- Grade 5 : Very loud, thrill present and audible with the stethoscope barely on the chest
- Grade 6 : Audible with the stethoscope off the chest.The difference between 2 and 3 or grades 5 and 6 may be somewhat subjective.
- Timing: The relative position within the cardiac cycle and with relationship to S1 and S2. Systolic (occurring between the first and second heart sounds), diastolic (between the second sound and the first sound), or continuous (present continuously through the cardiac cycle).
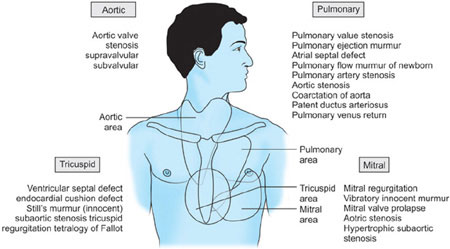
- Location and transmission: It should be noted where the murmur on the chest wall is heard loudest and the other areas where the murmur is audible (extent of radiation) (Fig. 1.2). Aortic valve stenosis has maximal intensity at the right upper sternal border and may radiate to the suprasternal notch and carotid arteries. Aortic valve regurgitation is most easily detected at the left upper sternal border with the patient sitting, leaning forward, in expiration. Pulmonary stenosis and regurgitation are maximal at the left upper sternal border. The severity of aortic or pulmonary regurgitation correlates with the amount of radiation. The systolic murmur of peripheral pulmonary stenosis is common in infancy and is maximal at the left upper sternal border and radiates to the infraclavicular, axillary regions and to the back. Systolic murmurs at the left lower sternal border usually represent a ventricular septal defect but can be associated with tricuspid regurgitation. The murmur of tricuspid regurgitation usually increases during inspiration.Mitral valve disease is best heard at the apex with the patient in the lateral decubitus position. Mitral regurgitation typically radiates to the axilla. Sites other than the precordium need to be auscultated as well. Coarctation is best heard in the intrascapular region on the back. Long-standing severe coarctation can produce collateral circulation audible as continuous murmur over the ribs where the intercostals arteries course. Arteriovenous malformations may be audible over the affected body region in the cranium for vein of Galen malformations or right upper quadrant for hepatic source.
- Duration: The time of the murmur from beginning to end.
- Pitch: The frequency range of the murmur.
- Quality: Harsh murmurs are characteristic of murmurs caused by ventricular outflow tract obstruction or hyperdynamic states. Blowing murmurs are typical of valve regurgitation. A rumbling quality is a feature of diastolic turbulence across atrioventricular valves. A vibratory, musical, or humming property is associated with the innocent Still's murmur.
Classification of Heart Murmurs
Based on the timing of the heart murmur to the S1 and S2, the heart murmur may be classified into three types.21
Systolic Murmur
Systolic murmurs also are classified by their dynamic mechanism, of which there are four types (Fig. 1.3).
- Regurgitation (backward flow of blood)
- Obstruction to forward flow
- Vibration of tissues in heart chamber
- Excessive flow of blood through a normal orifice or vessel.
Thus, the systolic murmurs may be: (i) Holosystolic murmurs when they begin with S1 and continue at the same intensity to S2. These occur when a regurgitant atrioventricular valve is present (tricuspid or mitral) or in association with a majority of ventricular septal defects and each is associated with a high systolic pressure gradient. The murmur of mitral regurgitation is heard loudest at the apex and radiates toward the axilla. The murmur of ventricular septal defect is heard best along the left sternal border, over the right ventricular area. The murmur of tricuspid regurgitation is unique in that it increases in intensity during inspiration because of increased right ventricular filling. Usually pansystolic murmurs are harsh or blowing murmurs. (ii) Ejection murmurs; crescendo-decrescendo or diamond shaped murmur that may arise from narrowing of the semilunar valves or outflow tracts. The velocity and volume of blood passing through the valve is greatest toward the center of systole, and thus the murmur will be loudest in mid-systole creating a crescendo-decrescendo, “diamond shaped” type of murmur. These loud coarse murmurs generally occur over the pulmonary or aortic valve. The murmur of aortic coarctation tends to be higher in pitch, but it is heard in a different area, being maximal high in the precordium, in the left axilla, and over the left side of the back. Generally, obstructive murmurs are coarse and they tend to radiate in the direction of blood flow, e.g. murmur of aortic stenosis is well heard over the carotid arteries. (iii) Vibratory murmur: A medium-18pitched musical murmur would sound like a hum. Because vibration occurs in tissue, it often transmits in the same tissue plane. Thus, the common still's murmur is a vibratory murmur arising in the left ventricular outflow tract will transmit through the left ventricular tissue toward the apex or through the aortic wall up toward the aortic area. Merely detecting a musical quality of the murmur in children means that the chances of the murmur being innocent are high. (iv) Flow murmurs are generated by the turbulence associated with an increased stroke volume. Systolic flow murmurs occur in the outflow tract of either the left or right ventricle and accordingly are usually heard maximally at the left or right sternal border in the second interspace. Invariably, when the patient is examined in a standing position, the systolic flow murmur greatly diminishes in intensity or totally disappears, because of the decrease in stroke volume that occurs in the standing position. The characteristics of the second sound become extremely important in trying to interpret the significance of flow murmurs. Unfortunately, the mechanism of an atrial septal defect murmur, which is actually a flow murmur arising in the right ventricular outflow tract, is similar to that of the innocent functional flow murmur heard in normal individuals, and the two murmurs may be indistinguishable on auscultation. The key distinguishing feature is a characteristic wide and fixed splitting of the second sound that occurs with most atrial septal defects. With atrial septal defect, blood ejected from the right ventricle is constant in volume both in inspiration and in expiration; hence, splitting of the second sound is fixed, meaning it does not change with respiratory phase. Other features (easily palpable right ventricular impulse, mid-diastolic murmur in tricuspid area) may help in the diagnosis of atrial septal defect. (v) Mid to late systolic murmurs: begin midway through systole and are often heard in association with the mid-systolic clicks in insufficiency of mitral valve prolapse (Fig. 1.3). The “whoop” that occurs with mitral valve prolapse is best heard with the patient standing. It occupies the mid-late portion of systole and may be exceedingly loud, sometimes audible without a stethoscope. Whoops are usually evanescent, being loud at one time and absent at another. The patient is usually tall asthenic and frequently has a thoracic bony abnormality such as pectus excavatum. Mitral valve prolapse may be familial due to a congenital conective tissue defect.

Diastolic Murmurs
These are further classified as early diastolic, mid-diastole or presystolic. Usually seen with regurgitation of the semilunar valves, stenosis of atrioventricular valve or an increased flow across the atrioventricular valve. Early diastolic murmurs are decrescendo in nature and arise either from aortic or pulmonary valve insufficiency. Mid-diastolic murmurs are diamond shaped and occur either because of an increased flow across a normal tricuspid or mitral valve or normal flow across an obstructed or stenotic tricuspid or mitral valve.22
All diastolic murmurs are organic. Diastolic murmurs are classified similarly to systolic murmurs and may be early, beginning with the second sound, mid, or mid-late or presystolic. The mechanisms are the same, and the murmurs that are produced, are therefore regurgitant, obstructive, flow, or vibratory.
Regurgitant diastolic murmurs imply either aortic or pulmonary valve regurgitation. As with systolic regurgitant murmurs, the murmur begins with the closure of that portion of the second heart sound caused by the closure of either the pulmonary or aortic valve. The murmur of aortic regurgitation will be high pitched because of the high-pressure gradient between the aorta and the left ventricle in diastole, and it will be heard maximally along the left sternal border. The murmur of pulmonary regurgitation with normal pulmonary artery pressure is low pitched because of the low-pressure gradient; it is heard in the same area as the aortic regurgitation murmur. When the child has pulmonary hypertension, the murmur, known as the Graham-Steell murmur, is of high pitch, because of the high-pressure gradient between the pulmonary artery and the right ventricle in diastole.
Obstructive murmurs are caused by mitral or tricuspid stenosis of usually, chronic rheumatic carditis. Decrescendo-crescendo in shape related to flow velocity, the murmur will be low pitched, and it will not begin until the mitral valve opens; therefore, there will be a pause between the second sound and the start of the murmur. With mitral valve stenosis, the murmur occurs in the left ventricle and is loudest at the apex.
A diastolic flow murmur also is noted with lesions such as moderate to large ventricular septal defect, atrial septal defect, and mitral or tricuspid regurgitation. Its presence indicates that flow volume across the AV valve is at least twice normal. Mid-diastolic in timing, of short duration, and medium pitch, it is heard maximally in either the apical or tricuspid areas, according to which valve generates the turbulence.
Continuous Murmurs
Flow through vessels or channels distal to the semilunar valves begin in systole and persist through S2 into early, mid, or all of diastole. Continuous murmurs are generally pathologic except the continuous murmur of venous hum.
Of the many causes of continuous murmurs, only two are of major importance. The venous hum is seen in children whose circulation is hyperkinetic, continuous turbulence is audible over the jugular veins, usually loudest in the right supraclavicular fossa. This murmur, usually heard only in the sitting or upright position, varies considerably in intensity with movement of the child's head and its intensity may be influenced by light pressure on either jugular vein. The turbulence may also be palpated with light pressure on the jugular vein.
The other important continuous murmur is that of a patent ductus, heard maximally on the left side of the thorax, usually just below the clavicle, or between the left sternal border and the midclavicular line in the second interspace. Flow through a patent ductus of average size increases aortic runoff and left ventricular stroke volume. Accordingly, the pulse will be bounding and left ventricular activity is readily palpable. The ductus murmur has a “machinery” quality. The other causes of continuous murmurs are:
- Systemic and pulmonary arterial circulations: Surgically created Blalock-Taussig, Waterston, Potts, or central shunts, patent ductus arteriosus, aortopulmonary collaterals, aortopulmonary window, anomalous left coronary artery arising from the main pulmonary artery
- Systemic arteries and veins: Arteriovenous malformation
- Systemic arteries and cardiac chambers: Coronary arteriovenous fistula, ruptured sinus of Valsalva aneurysm
- Disturbed flow in arteries: Collateral circulation associated with severe coarctation
- Disturbed flow in veins: Venous hum.
In a coronary AV fistula the continuous murmur is best heard low along the left sternal border. A continuous murmur is distinguished from a to-and-fro murmur, which consists of two murmurs, one that occurs in systole and the other that occurs in diastole. A to-and-fro murmur does not continue through S2 but instead has peak intensity earlier in systole. Examples include patients with combined aortic stenosis and aortic regurgitation (as can occur after balloon dilation of a stenotic bicuspid valve), combined pulmonary stenosis and pulmonary regurgitation (as can occur after repair of tetralogy of Fallot), or ventricular septal defect, prolapsed aortic cusp, and aortic regurgitation.
Additional Sounds
- The terms, clicks and snaps are a continual source of confusion. Valve opening is quiet in health and signals the end of the period of isovolemic contraction or relaxation. When a sound is heard at the time of the opening of any heart valve, it is abnormal.20–22A sound heard at the time of opening of the pulmonary or aortic valve is called an ejection click; when mitral or tricuspid opening is heard, the term opening snap is used. The “clicks” signal the beginning of ejection into a dilated great vessel; the “snaps” signal the commencement of diastolic flow into the ventricle.Opening Snap: An opening snap is a high-frequency sound associated with mitral stenosis. As the degree of mitral stenosis progresses, the opening snap occurs earlier in diastole because of elevated atrial pressures and becomes softer because of decreased leaflet mobility.Clicks: Ejection clicks are brief, high-frequency, sharp sounds that have a quality distinct from S1 and S2. They usually are associated with abnormal valve structure. Evaluation of location, timing (early versus mid-systolic), and nature (constant versus variable) enables the examiner to determine the affected valve. In patients with mitral valve prolapse, the click may be associated with a murmur of mitral regurgitation that is only present or 21louderin the standing than supine position because of reduced left ventricular volume that produces a greater degree of prolapse.The click associated with aortic stenosis or bicuspid aortic valve is best detected at the apex rather than the aortic valve region at the right upper sternal border. At times, it is difficult to distinguish a split S1 (normal variant) from an aortic valve ejection click, and echocardiography is needed for differentiation. The click associated with pulmonary stenosis is located at the left upper sternal border and is variable and louder in expiration because of greater systolic valve excursion in this phase of the respiratory cycle. Clicks associated with semilunar valve stenosis become softer as the degree of obstruction progresses because of reduced valve mobility. Ebstein's anomaly of the tricuspid valve can be associated with a systolic click at the left lower sternal border. Clicks occasionally occur in conditions associated with dilation of the aorta or pulmonary artery. The latter can occur with pulmonary hypertension, patent ductus arteriosus, or idiopathic dilation of the main pulmonary artery. In neonates with left-to-right shunting across a patent ductus arteriosus, there may be multiple systolic clicks at the left upper sternal border. Clicks can also be produced by membranous ventricular septal defects associated with aneurysm of the ventricular septum and are located at the left lower sternal border.
- Pericarditis and mediastinal emphysema: Two other auscultatory findings of significance are the pericardial friction rub of pericarditis and the mediastinal crunch of mediastinal emphysema. Pericardial friction occurs most frequently after operation in patients undergoing cardiac surgery, or in the so-called postpericardiotomy syndrome, which characteristically occurs 3 to 6 weeks after operation. In a nonoperative situation, it may be a sign associated with pericarditis from any cause, but usually viral. Most clinicians identify a friction rub easily because of its characteristic scratchy quality. The sound is not present if there is a moderate to large pericardial effusion because the two surfaces of the pericardium cannot rub together. Pericardial rubs may be heard anywhere on the left side of the chest but are usually best heard along the sternal border with the patient sitting and leaning forward and often has inspiratory accentuation. They generally have three phases, related to atrial filling, ventricular ejection, and the rapid phase of ventricular filling giving a triple cadence. The mediastinal crunch has much the same quality as pericardial friction, and although it may have a to-and-fro rhythm, it will not have a three-phase cadence. More often, its rhythm will be chaotic, at times systolic and at times phasic with respiration.23Relative timings of heart sounds and added sounds on auscultation are shown in (Fig 1.4).
Innocent heart murmurs also called as functional murmurs arise from cardiovascular structure in the absence of anatomical abnormalities. More than 80% of children have innocent murmurs sometime during childhood, usually beginning around 3 to 4 years of age. All innocent murmurs are accentuated or brought out in a high output state, usually during a febrile illness. A left ventricular false tendon is often found in children and adults with innocent heart murmurs.

Figure 1.4: Relative positions of heart sounds and added sounds in auscultation. Sounds in red are high pitched. A2: aortic component of second heart sound; EC: ejection click; MSC: mid-systolic click; OS: opening snap; P2: pulmonary component of second heart sound; S1–S4: heart sounds.22
|
When one or more of the following are present, the murmur is more likely pathologic and requires cardiac consultation, i.e. symptoms, abnormal cardiac size or silhouette or abnormal pulmonary vascularity on chest X-ray, abnormal ECG, diastolic murmur, a systolic murmur that is loud (with a thrill), cyanosis, abnormally strong or weak pulse and abnormal heart sounds11,12,27 (Table 1.4). An underlying fear that a cardiac abnormality is present may negatively affect a child's self-image and subtly influence personality development and a 2D echocardiogram may allay this anxiety.
Chest Examination
Chest Deformity
Congenital heart disease associated with cardiomegaly can produce prominence of the left chest because of the effects of cardiac contraction against an elastic rib cage. Pectus carinatum is a feature of Marfan syndrome. Pectus excavatum is associated with mitral valve prolapse; the mitral valve prolapse often improves after surgical correction of the chest wall deformity. An 23asymmetric precordial bulge can also be seen in pulmonary conditions, including atelectasis, pneumothorax, emphysema, and diaphragmatic hernia.
Chest pain in children frequently has a musculoskeletal basis, including costochondritis, slipping rib syndrome, or myodynia. The diagnosis of musculoskeletal pain can be confirmed by an ability to reproduce a similar quality of discomfort by palpation of the chest. The examination should include palpation of the costochondral junctions, the insertion site of the pectoralis major muscle group by grasping the head of the muscle between the examiner's fingers and thumb, the inframammary area, and other regions of the chest where pain is reported. Although one would expect the right and left costochondral junctions to be equally affected, the left-sided junctions are more typically involved. In patients with slipping rib syndrome, the examiner can perform the “hooking” maneuver by placing fingers around the lower costal margin and lifting anteriorly to elicit a click and reproduce pain. The demonstration of pain reproduction and an explanation of the anatomic basis are reassuring to the family and patient and help allay concerns about the heart.28
Pulmonary Auscultation
Lesions associated with excessive pulmonary flow or left-sided dysfunction or obstruction can be associated with inspiratory rales or expiratory wheezing. These features are also present in patients with reactive airway disease or pneumonia.
Abdomen Examination
Palpation of the liver yields information about visceral situs and central venous pressure. A right-sided liver indicates normal situs of the abdominal viscera, a left-sided liver indicates situs inversus, and a midline liver indicates the presence of situs ambiguous and heterotaxy. Hepatomegaly is present in conditions associated with elevated central venous pressure. Percussion of the liver size helps to distinguish patients with “false” hepatomegaly caused by inferior displacement by a flattened diaphragm caused by hyperinflation. Palpation of the liver is easier when the abdomen is soft. Flexing the knees can relax the abdominal musculature. In infants, the liver can normally be palpated about 2 cm below the costal margin in the midclavicular line. In children, the liver can be palpated 1 cm below the right costal margin. An engorged liver is usually tender to palpation. A pulsatile liver is palpated in patients with elevated right atrial pressure, most commonly associated with significant tricuspid regurgitation.
In infants, a spleen tip can normally be palpated under the costal margin. Location of the spleen also aids in determination of visceral situs. Elevated central venous pressure usually does not produce splenomegaly. An enlarged spleen is a feature of bacterial endocarditis, and in a known cardiac patient with fever or new regurgitant murmur, this physical finding should prompt thorough evaluation of that complication.
Thus, equipped with data from history and clinical examination data, the clinician can arrive at an appropriate clinical diagnosis. With a systematic approach, the physician can develop the skills and confidence that will allow to make correct decisions on most children. Best classification and a simplistic approach is the one proposed by the legend, late Dr Paul wood29 and are based on answering the following basic questions:
- Q1. Does the child have a CHD?
- Q2. Is the child cyanotic or acyanotic?
- Q3. Is the pulmonary arterial blood flow increased or not?
- Q4. Does the malformation originate from the right side or left side of the heart?
- Q5. Which is the dominant ventricle?
- Q6. Is pulmonary hypertension present or not?
The clinical findings have to be interpreted in terms of the underlying hemodynamic disturbance and conclude by noting the severity of lesion and complications, if any.
SUMMARY
A good clinical assessment can spare many children with cardiovascular complaints from unnecessary or inappropriate investigative procedures. The key element is a systematic approach that always interprets each symptom and sign in terms of the underlying hemodynamic disturbance.
REFERENCES
- Zoneraich S, Spodick DH. Bedside science reduces laboratory art. Circ. 1995;91:2089–92.
- Gillian M Blue, Edwin P Kirk, Gary F Sholler, et al. Congenital heart disease: Current knowledge about causes and inheritance. Med J Aust. 2012;197(3):155–9.
- John F Keane, Donald C Fyler, James E Lock. History. Physical examination and laboratory tests. In: Fyler DC (2nd edition) Nadas ‘Pediatric Cardiology St. Louis. Mosby. 2006.
- Emmanouildes GC, Reemenschneider TA, Alien HD, et al. Moss and Adams Heart Diseases in Infants, Children, and Adolescents. Including Fetus and Young adult. 5th edition Baltimore, Williams & Wilkins. 1995.
- Mc Connell ME, Adkins SB, Hannon DW. Heart Murmurs in Pediatric Patients: When Do You Refer? Am Fam Physician. 1999;60(2):558–64.
- Pelech AN. Evaluation of the pediatric patient with a cardiac murmur. Pediatr Clinic of North Am. 1999;46:167–87.
- Surendranath R. Veeram Reddy, Harinder RS. Chest Pain in Children and Adolescents. Pediatrics in review. 2010;31(1). pp. e1–e9.
- Martin K, Bates G, Whitehouse WP. Transient loss of consciousness and syncope in children and young people: What you need to know. Arch Dis Child Educ Pract Ed. 2010;95:66–72.
- Yun SL, Jae SB, Bo Sang K, Gi BK, et al. Pediatric Emergency Room Presentation of Congenital Heart Disease. Korean Circ J. 2010;40(1):36–41. Published online 2010 January 27.
- Rao PS. Diagnosis and management of cyanotic congenital heart disease: part I. Indian J Pediatr. 2009;76(1):57–70. Epub 2009 Apr 18.
- Erin M, Michael Silberbach. Heart Failure in Infants and Children. Pediatrics in review. 2010;31(1). pp. 4–12.
- National High Blood Pressure education Program Working Group on Hypertension Control in Children and adolescents. Update on the 1987 Task Force Report on High Blood Pressure in children and Adolescents: A Working Group. Report from the National High Blood Pressure Education Program. Pediatrics. 1996;98:649–58.
- National High Blood Pressure Education Program Working Group. The Fourth report on the diagnosis, evaluation and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114:555–76.
- Gaskin, PR, Owens A, Talner SN, et al. Clinical Auscultation Skills in Pediatric Residents. Pediatrics. 2000;105:1184–87.
- Michael S, David Hannon. Presentation of Congenital Heart Disease in the Neonate and Young Infant. Pediatrics in review. 2007;28(4). pp. 123–31.
- Taggart NW, Cetta F. Overview of Congenital Heart Disease. Epocrates Online: BMJ Group. [Internet] 2011 [updated 2010 Nov 30; cited 2011 Mar 6].
- Uazman Alam, Omar Asghar, Sohail Q Khan, et al. Cardiac auscultation: an essential clinical skill in decline. Br J Cardiol. 2010;17(1). pp. 8–10.
- Dhuper S, Vashist S, Shah N, Sokal M. Improvement of cardiac auscultation skills in pediatric residents with training. Clin Pediatr (Phila). 2007;46:236–40.
- Haney I, Ipp M, Feldman W, McCrindle B. Accuracy of clinical assessment of heart murmurs by office based (general practice) paediatricians. Arch Dis Child. 1999;81:409–12.
- Asprey DP. Evaluation of children with heart murmurs. Lippincot's Primary Care Practice 1998;2(5):505–13.
- Pelech AN. The cardiac murmur. Pediatr Clin North Am. 1998;45:107–22.
- Maisch B, Seferovic PM, Ristic AD, et al. Guidelines on the diagnosis and management of pericardial diseases executive summary: The Task Force on the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology. Eur Heart J. 2004;25:587–610.
- Rosenthal A. How to distinguish between innocent and pathologic murmurs in childhood. Pediatr Clin North Am. 1984;31:1229–40.
- Biancaniello T. Innocent Murmurs. Circulation. 2005;111:20–22.
- Sapin SO. Recognizing Normal Heart Murmurs: A Logic-based Mnemonic. Pediatrics. 1997;99:616–18.
- Satou GM, Halnon NJ. Pediatric Congestive Heart Failure. eMedicine: WebMD. [Internet] 2011 [updated 2009 Mar 19; cited 2011 Mar 6].
- Shamberger RC. Cardiopulmonary effects of anterior chestwall deformities. Chest Surgery Clinics of North America. 2000;10(2):245–52.
- Somerville J. Congenital heart disease—changes in form and function. Br Heart J. 1979;41(1):1–22. [PMC free article] [PubMed]