

The proximal femur consists of the femoral head, neck femur, intertrochanteric and subtrochanteric regions. The femoral head articulates with the acetabulum to form a ball and socket hip joint. The femoral head is a round structure of cancellous bone sheathed in the articular cartilage, and is characterized by a dense meshwork of trabecular bones which absorbs and evenly distributes weight to the femoral neck and proximal femur. The femoral head is not a perfect sphere, and the joint is congruous only in the weight-bearing position.1, 2 The size of the femoral head varies in proportion to the body mass and ranges roughly from 38 to 58 mm in diameter and is covered by articular cartilage with an average thickness of 3 to 4 mm.2
The femoral neck lies between the femoral head and the intertrochanteric line anteriorly and the intertrochanteric crest posteriorly. The femoral neck forms an angle with the femoral shaft in the anteroposterior plane ranging from 125° to 140° and an angle of anteversion of 10° to 15° in the lateral plane. In 1938 the internal trabecular system of the femoral head was described by Ward (Figs 1.1A and B). The cancellous bone of the femoral neck has a special trabecular arrangement which is organized into medial and lateral trabecular systems. The orientation is along the line of stress, and thicker lines come from the calcar and rise superiorly into the weight-bearing dome of the femoral head.
The forces acting in this arcade are largely compressive. Lesser trabecular patterns extend from the inferior region of the foveal area across the head and superior portion of the femoral neck into the trochanter and lateral cortex. The presence of osteoporosis is important, especially when the patient is being considered for internal fixation, because the ability of the osteoporotic bone to hold an internal fixation device is poor and such bone can affect the treatment alternatives. The trochanteric region is an area of high stress concentration that is subject to multiple deforming forces, making anatomic reduction of a fracture difficult. The intertrochanteric region of the proximal femur consists of greater and lesser trochanters and it represents a transition zone from the neck of 2the femur to the shaft.


This area is primarily characterized by a dense network of trabecular bone which serves to transmit and distribute the stress, similar to the neck of the femur. The major muscles of the gluteal region are inserted into the greater trochanter; gluteus medius, gluteus minimus and short external rotators, whereas the iliopsoas muscle is inserted into lesser trochanter. The greater trochanter is the site of insertion of the powerful hip abductors, gluteus medius and minimus and short external rotators of the hip (Fig. 1.2). The lesser trochanter is a posteromedial bony eminence at the inferior aspect of the intertrochanteric ridge that provides attachment to the iliacus and psoas hip flexors (Fig. 1.2). These muscles act on the proximal fragment of a subtrochanteric femur fracture, resulting in a flexed, abducted, and externally rotated position. The distal fragment is shortened and adducted by the hamstrings and hip adductors, resulting in an overall varus and anterior apex deformity at the fracture site. The calcar femoral, a dense bone which extends from the posteromedial aspect of the proximal femoral shaft to the posterior part of the femoral neck, forms a strong strut on the inferior part of the femoral neck and intertrochanteric region and serves a strong conduit for the weight transfer. The calcar femorale is thicker medially and gradually thins as it passes laterally.
The subtrochanteric region extends from the lesser trochanter to an area 5 cm distal, and consists primarily of thick, dense cortical bone. This is an area of high stress concentration, with large compressive forces medially and tensile forces laterally. The dense cortical bone permits efficient transmission of loads.
The hip capsule is attached proximally to the acetabulum and distally to the medial side of the greater trochanter, intertrochanteric line anteriorly, superiorly and medial to the lesser trochanter, and to the base of the femoral neck posteriorly. The entire anterior aspect of the femoral neck and proximal 3two-thirds of its posterior portion lie within the capsule.

Three prominent ligaments, iliofemoral, ischiofemoral, pubofemoral and one minor ligament—zona orbicularis conjoins with the hip joint capsule.
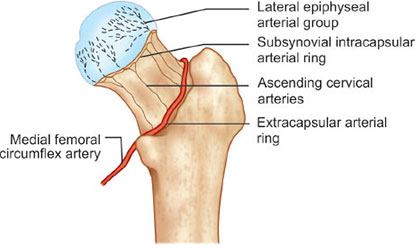
The hip joint capsule is a strong fibrous structure that encloses the femoral head and most of its neck. The capsule is attached anteriorly at the intertrochanteric line; posteriorly, however, the lateral third of the femoral neck is outside the capsule. That portion of the neck that is within the capsule has essentially no cambium layer in its fibrous covering to participate in the peripheral callus formation during the healing process. Therefore, healing of the femoral neck area is dependent on endosteal union alone. The blood supply to the femoral head and neck is complex. The femoral head derives its blood supply from the two largest tributaries of the profunda femoris. Medial and lateral femoral circumflex arteries send branches that anastomose to form an extracapsular arterial ring at the base of femoral neck (Figs 1.3 to 1.5). From this arterial ring, it sends ascending cervical arteries 4called as retinacular arteries which pierce the hip joint capsule and traverse along the neck of the femur deep to the synovial membrane.


There are four major retinacular arteries, out of which the lateral retinacular artery is the most important blood supply to the femoral head and neck. The femoral head also receives blood supply from the artery of the ligament of head of femur, which branches from the obturator artery.
References
- Cathcart RF. The shape of femoral head and preliminary results of clinical use of anonspherical hip prosthesis. J Bone Joint Surg Am 1971;53:397.
- Hoaglund FT, Low WD. Anatomy of the femoral neck and head, with comparative data from Caucasians and Hong Kong Chinese. Clin Orthop 1980;152:10–6.