



Headquarter
Jaypee Brothers Medical Publishers (P) Ltd
4838/24, Ansari Road, Daryaganj
New Delhi 110 002, India
Phone: +91-11-43574357
Fax: +91-11-43574314
Email: jaypee@jaypeebrothers.com
Overseas Offices
J.P. Medical Ltd
83 Victoria Street, London
SW1H 0HW (UK)
Phone: +44-2031708910
Fax: +02-03-0086180
Email: info@jpmedpub.com
Jaypee-Highlights Medical Publishers Inc
City of Knowledge, Bld. 237, Clayton
Panama City, Panama
Phone: + 507-301-0496
Fax: + 507-301-0499
Email: cservice@jphmedical.com
Jaypee Brothers Medical Publishers (P) Ltd
17/1-B Babar Road, Block-B, Shaymali
Mohammadpur, Dhaka-1207
Bangladesh
Mobile: +08801912003485
Email: jaypeedhaka@gmail.com
Jaypee Brothers Medical Publishers (P) Ltd
Shorakhute, Kathmandu
Nepal
Phone: +00977-9841528578
Email: jaypee.nepal@gmail.com
Jaypee Brothers Medical Publishers Ltd
The Bourse
111 South Independence Mall East
Suite 835, Philadelphia, PA 19106, USA
Phone: + 267-519-9789
Email: joe.rusko@jaypeebrothers.com
Website: www.jaypeebrothers.com
Website: www.jaypeedigital.com
© 2013, Jaypee Brothers Medical Publishers
All rights reserved. No part of this book may be reproduced in any form or by any means without the prior permission of the publisher.
Inquiries for bulk sales may be solicited at: jaypee@jaypeebrothers.com
This book has been published in good faith that the contents provided by the author contained herein are original, and is intended for educational purposes only. While every effort is made to ensure accuracy of information, the publisher and the author specifically disclaim any damage, liability, or loss incurred, directly or indirectly, from the use or application of any of the contents of this work. If not specifically stated, all figures and tables are courtesy of the author. Where appropriate, the readers should consult with a specialist or contact the manufacturer of the drug or device.
Obstetric Vasculopathies
First Edition: 2013
9789350904602
Printed at
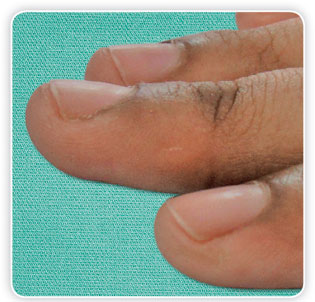
Nail is a hard covering of all finger and toe tips. They may be altered due to external or internal (systemic) factors. The nails in humans are considered as an aesthetic outgrowth, but its real function is to protect the soft ends of the phalanges or digits. They help to pick up small objects and are an important tool for scratching. In other species, this structure is slightly different, for example, crocodiles have a thimble-shaped structure that covers the whole tip of their digits, whereas hawks and owls have talons, which are highly curved claws specialized for prey capture, and horses and cows have hooves that protect their feet (Figures 1.1A to C). Comparative analysis of nail, claw, and hoof morphogenesis reveals relatively subtle differences in mesenchymal and epithelial pattern underlying these adult differences in distal limb appendage morphology.1
Nails have evolved from claws of reptiles. Primitive snakes like pythons and boas have vestigial hind limbs, which are tiny, clawed digits known as anal spurs. Claws are typically curved ventrally (downwards in animals) and compressed sideways. They serve a multitude of functions including climbing, digging, and fighting and have undergone numerous adaptive changes in different animal taxa. Claws are useful on large-diameter branches, whereas wide fingertips with nails and epidermal ridges are required for habitual locomotion on small-diameter branches. With the evolution of grasping hands and feet in primates, claws were no longer necessary for locomotion, and instead a reduction in the thickness of deep layer of the claw led to the advent of nails.2

Figures 1.1A to C: (A) Thimble-shaped structure covering the digit of crocodile; (B) Talons in birds; (C) Hoof
A study predicted morphoclines in fingertip morphology among four small-bodied (<1 kg) New World monkeys in order to test previous functional and adaptive explanations for the evolution of flattened nails, expanded apical pads, and grasping extremities within the order primates. The observed morphoclines demonstrate that a gradient in form from claw to nail like tegulae exists among these taxa. Thus, the distinction between claw and nail bearing platyrrhines is essentially arbitrary. According to Cartmill's (1972) functional and adaptive model for the loss of claws in primates, expanded apical pads are required for habitual locomotor and postural behaviors on small-diameter supports whereas claws are more useful for positional behaviors on large-diameter substrates.3
A nail is homologous to a claw but is flatter and has a curved edge instead of a point (Figure 1.2). A nail that is big enough to bear weight is called a ‘hoof’. Some marsupials also have nails and this is a good example of convergent evolution. It shows that flat nails are an important goal for evolution. Appearance of nails led to the development of critical functions, including finger pads that allow for sensitive touch and the ability to grasp.
The issue of whether nails or claws were present on the digits of the last common ancestor of living primates is central to the understanding of the ecological context in which the order originated. The combined new and old data indicate that the last common ancestor of the extinct primates had lost the typical mammalian claws of its ancestors and developed nails on all pedal digits except digit II, which bore a toilet-claw.4 Toilet claw is an intermediate evolutionary step between claws and nails. Their shape is similar to claws, but their tip is not as pointed.
Teilhardina Brandti, a lemur like early primate that lived about 55 million years ago, was the first primate to exhibit nails on all digits. Its nails allowed the lemur-like animal to grasp onto branches and move through the trees with more agility. The fossils are the first evidence of primates with nails on all digits.5
As civilization progressed and social interactions grew, nails have become objects of adornment and beauty. Good nails are considered to be sign of good health. Nail manicure has been there for more than 4000 years and women take care of their nails more than men.
3
Evolution of nailpolish: There is not an exact record of the invention of fingernail polish, but it is believed to have originated in China, somewhere around 3000 BC Early batches were made from mixtures of bees’ wax, gelatin, egg whites and gum Arabic. Members of the Egyptian upper class were also using fingernail polish around this same time; their mixture resembled lacquer paint, and was used to represent money and prosperity. Around 600 BC, the royal colors of China were metallic, gold and silver. These were also the colors of choice for nail polish. The lower class in China was not allowed to wear polish on their fingers, and could be sentenced to death if they were caught. In the 1920s, Michelle Menard was inspired by the invention of new automobile paint, and she used this inspiration to modernize fingernail polish, giving it the look that we are now familiar with.6
References
- Hamrick MW. Development and evolution of the mammalian limb: adaptive diversification of nails, hooves, and claws. Evol Dev. 2001;3(5):355–63.
- Hamrick MW. Functional and adaptive significance of primate pads and claws: evidence from New World anthropoids. Am J Phys Anthropol. 1998;106(2):113–27.
- Soligo C, Müller AE. Nails and claws in primate evolution. J Hum Evol. 1999;36(1):97–114.
- Oldest Evidence of Nails in Modern Primates. Science. Daily; 2011.
- http://www.ehow.com/ The History of Fingernail Polish.
Nails are ectodermal appendages covering the dorsal aspects of the digits. It is a horn-like envelope providing protection to the terminal phalanges of fingers and toes in humans, most primates, and a few other mammals. Nails are akin to the claws, present in numerous other animals and are made of a tough protein called keratin, similar to animal hooves and horns.1 Nail is a subject of global importance for dermatologists, podiatrists and surgeons. It is imperative to understand the anatomy and structure of the nail for better understanding of various nail diseases, prior to undertaking any nail surgery or therapy of nail disease.2
Functions of the Nail
The nail organ is an integral part of the digital tip in humans. It is a highly versatile tool (Box 2.1) with a relatively inflexible keratinous nail plate that covers and protects the finger tip, distal phalanx and the surrounding soft tissue from injury.1,2 Nails cover approximately one-fifth of the dorsal surface of the finger and up to 50% of the digit in the great toe.3 Toe nails also contribute to the pedal biomechanics.4 Finger nails enhance the precise delicate movements of the distal 5digit through counter pressure exerted on the pulp of the finger; the nail than acts as a counter force when the end of the finger is touching an object, thereby enhancing fingertip sensitivity.1–3
Despite the fact that the exposed part of the nail is comprised of dead cells, it is attached to a very sensitive portion of skin full of nerves. Any contact with the nail sends signals directly to these nerves, increasing sensitivity.1 The flat nail surface helps in the extended precision grip required, for example, in pulling out a fine splinter from the finger.1, 3 It aids in peripheral thermoregulation via the glomus bodies in the nail bed and matrix.2,5 The finger nails are also used for scratching, grooming and ar e an efficient natural weapon.4 Therefore, an abnormal alteration in the anatomy of the nail unit may interfere with the aforementioned functions. Finally, the nail contributes to the aesthetic appeal of the extremity resulted in a large evolving field of nail cosmetology. Painting the nails with nail lacquer is a common practice dating back to at least 3000 BC.1
Comparative Anatomy
The anatomy of nail unit can be compared from two aspects. One of them is comparison of nail with other ectodermal structures (hair, tooth) and other is phylogenetic comparison with claws and hoofs.
Nail and Other Appendages
An appendage is formed as a result of interaction between mesoderm and ectoderm, which corresponds to dermis and epidermis in differentiated state. Various appendages are related to each other as reflected by morphological and biochemical analysis. Hair and tooth are most closely related appendages to the nail. This is further highlighted by the concomitant involvement of nail, tooth, hair and sweat glands together in various ectodermal dysplasias.
Various diseases demonstrate inter relationship between appendages. Morphological similarities also exist between them. Achten noted that nail unit was similar to hair follicle in some aspects with the hair bulb being analogous to the intermediate nail matrix and cortex to the nail plate.6 Scanning electron microscopic studies show that structure of nail is more similar to compacted cuticular cells than cortical fibers. In pachyonychia congenita, alopecia affected region of scalp shows dyskeratosis of outer root sheath, thus attracting comparison with the nail bed.
Manabe and O'Guin also demonstrated that matrix, lingual papilla and other epithelial components of tooth can also be compared with nail unit as they share some morphological similarities and similar keratin expression as well.7 The various appendages have specific constituents such as keratin and trichohyalin. This is supported by the work of Deiko and Jidoi who demonstrated nine types of keratin expression in human nail and hair.8 Amongst these, keratins with moleculer weight 76, 73, 64, 61 and 55 kDa were common to hair and nail. Keratin with moleculer weight 61 kDa was specific to hair, and two components, both with 6molecular weight of 50 kDa, were specific to nail. Subsequently, Heid et al studied keratin expression in appendages using gel electrophoresis, immunoblotting, peptide mapping and complementary keratin analysis. They demonstrated that whilst nail plate contained both soft epithelial and hard hair or nail keratins, plucked hair contained only hard keratins.9 Although, small quantities of hard keratins are also found in embryonic thymus and lingual papilla, they can generally be considered to be a feature of the hair or nail differentiation. In dyskeratosis congenita altered keratin expression underlies the nail and oral mucosal changes and this reinforces the similarities in keratin expression in various appendages.10
Evolution
The nails of primates and hooves of the running mammals evolved from the claws of the reptiles. Claws are curved ventrally, pointed at ends, and have sideways compression. The underlying bone has the same shape as the claw. In contrast the nails are flat; less curved and do not point or extend beyond the tip of the digit. Thus, claws aided the more primitive animals in carrying out actions like climbing, digging and fighting in comparison to the improved manual dexterity nails provided to higher primates.1,11
Terminology
A brief synopsis of commonly used terminology used for description of the nail is provided in Table 2.1 (Figures 2.1 and 2.2).1,2,12,13
Embryology
The nail apparatus develops and matures from the primitive epidermis primarily between the ninth and twentieth week of intrauterine life.11 Nail development can be divided into two components, morphogenesis and tissue differentiation.14
Morphogenesis
In a developing embryo individual digits are identifiable from 8th week of gestation. Epithelium that will become a future nail unit at first is indistinguishable from adjacent epidermis. At the 9th week of gestation the dorsal tip of digit is covered by epidermis and an invagination of this primitive skin gives rise to the nail anlage.14 Nail anlage is the first embryonic element of nail unit. It is followed by appearance of primary nail field at 10th week (Figure 2.3), which is a distinct region overlying the tip of terminal phalanx. This field is surrounded by a well-defined proximal, lateral and distal groove. The primary nail field grows downwards and proximally by a wedge of germinative matrix cells extending back from the tip of the digit. These germinative matrix cells forming the nail matrix primordium are present proximal to both distal groove and ridge. These structures give rise to vestigial distal groove and hyponychium respectively.14 Later, the far boundary of the matrix is delimited clinically by a whitish zone in the shape of a hemiellipse that extends a little beyond the proximal nail fold to form the lunula.15
During 13–14 Weeks
Proximal nail field along with its surrounding tissue grows relatively slowly that results in the nail field becoming depressed and the epidermis overlaps the side and proximal end to form 7the proximal and lateral nail folds.11,14
|
At 13th week nail field is well demarcated, with the matrix primordium underlying a proximal nail fold and four components of the epithelium of a developing nail unit are visualized histologically, namely, the basal, spinous, granular, and cornified layers. By 14th week, the proximal part of a nail bed comes to be covered by a firm plate of cornified cells that is derived from the matrix and represents the developing nail plate (Figure 2.3) that can be visualized underneath the proximal nail fold. The nail plate cornifies considerably before any other cutaneous epithelium.14,15 By 16th week, the morphogenesis is almost complete and a fetal nail is discernible.2 8



17 Weeks to Birth
At 17 weeks, nail plate covers most of nail bed and the distal ridge has flattened. By 20 weeks, nail unit and finger grow in tandem, with nail plate abutting distal ridge; the region that represents the epithelium of the nail bed loses its granular zone; and the matrix cells show postnatal type of cell division and differentiation.3,14,15 By the 36th week, the nail plate completely reaches the tip of the digit by growing and extending to the distal groove (Figure 2.3) and there is well-formed cuticle and lateral nail folds. The finger nails appear longer than the toe nails.3,15 At birth the nail plate may curve over the volar surface of the finger and give rise to koilonychia. This is normal in the very young and will reverse with age.12,14
Tissue Differentiation
Keratin synthesis starts early and it can be identified from early stages of differentiation. At 12–13th week, the nail matrix analge, which is a thin epithelial wedge is considered to represent the ventral matrix primordium. Keratin represents 80% of intracellular structural protein of epithelial cells. At 15th week, hard keratin is present throughout nail bed and matrix. However, at 22th week, proportions of keratinocytes having hard keratin in nail bed is low, while it is significantly higher in the matrix. Nail differentiation is mostly complete by the 25th week; although some chemical alterations in nail constituents may continue till birth.12,14
Nail Anatomy
The nail at the tip of the digit is associated with tissue components like the bone, distal interphalangeal joint and its capsule, ligaments, tendons, arteries, veins, lymphatic vessels, nerves, and specialized nervous end organs.2 The extensor and flexor tendons cross the distal interphalangeal joint and the former attach proximal to the nail matrix. Further, lateral tendons join the base of distal phalanx to the ungual process spines and fibrous septae attached to the periosteum providing an anchor to the nails.13 A human nail is principally made up of four parts: the matrix, the plate, the nail bed and the nail folds.1,2 The matrix acts as a base for the rest of the nail, containing nerves as well as lymph and blood vessels and produces the rest of the nail plate.1 The matrix is mostly located under the proximal nail fold and the only part of the matrix that is visible to the naked eye is the white, crescent portion of the nail known as the lunula.13 Above the matrix is the nail bed, which is made up of the dermis and epidermis and is firmly attached to the nail plate.1,2 The visible portion of the nail, or the nail plate, is comprised of keratin and amino acids.1 The bone of the finger determines the shape of the nail which is evidenced by the altered nail shape in patients with syndactyly or when lateral osteophytes at the base of the distal phalanx of toes produce pincer toenails.2
Nail Plate
Nail plate or nail body (Figure 2.1) is a compact keratinized epithelial structure covering the nail bed and intermediate matrix continuously produced during the life time. It is durable, chemically resistant, and partially translucent. The plate appears pink because of the underlying capillaries 10and its transverse shape is determined by the shape of the underlying bone. It is curved in both the longitudinal and transverse axis thus allowing it to be strongly embedded in nail folds and the free edge is useful as a tool.12 This feature is more marked in toe nails as compared to fingers and the curvature shows great individual variations. A relatively flat big toenail has a lower risk of development of an ingrown nail in comparison to a nail with prominent transverse curvature.2 The upper surface of nail plate is smooth and shiny and may have a variable number of longitudinal ridges that change with age resulting in loss of nail plate lustre with age.2,12 These ridges are sufficiently specific to each individual to allow forensic identification and distinction of identical twins.12 The nail shine may be attributed to the proximal matrix and surgical or traumatic damage may result in a dull appearing nail surface.2 The intermediate layer of the nail plate is much thicker, with less evident flattening of cells. It also has longitudinal ridges on its ventral surface which corresponds to complementary ridges on the dorsal aspect of nail bed. These ridges may be best examined using polarized light and can be used for forensic identification as well. These layers of nail plate can be distinguished by distinct birefringence in polarized light and particular staining pattern using Giemsa stain. The nail plate gets thickened as it grow distally as is observed after analysis of nail specimens, however, in vivo ultrasonographic studies suggest there may be 8.8% reduction in thickness distally. A thickened nail plate may imply a long intermediate matrix. Other factors influencing its thickness include linear rate of nail growth, vascular supply, subungual hyperkeratosis and drugs.12
Nail Matrix
The nail matrix is the germinative part of nail unit and is solely responsible for production of nail plate. It is divided into three parts: dorsal section contributing to most of the superficial layers of the nail plate, whereas, intermediate region forms the deeper layers. The ventral region is the most distal part of the nail matrix. It is located on the proximal dorsal aspect of the distal phalanx and just distal to the interphalangeal joint (Figure 2.2).12 Most part of it is covered by proximal nail fold and it is visible as band with parallel margins that are convex distally; thus its lateral corners are more proximal than the central part and give rise to the so called lateral matrix horns.12,13 It is of clinical relevance while performing a lateral longitudinal nail biopsy or a wedge excision for an ingrown nail. The dorsal expansion of the lateral ligament attaches the lateral matrix horns to the distal interphalangeal joint.2 The most distal part of matrix is the lunula, which is visible as whitish half-moon shaped structure situated between the free margin of proximal nail fold and nail bed. Lunula is normally visible only in the thumb and middle finger and is absent in the little finger (Figure 2.1).1,12 It may be concealed by the proximal nail fold.
The width and thickness of the nail plate is determined by the size, length, and thickness of the matrix, while the shape of the fingertip determines if the nail plate is flat or arched. The proximal 50% of the matrix contributes almost 80% of the nail plate cells; thereby surgery of the distal matrix has a lower risk of scarring.2,11 The matrix grows from the proximal-to-distal direction and; therefore, matrix biopsies should always have their long axis in the transverse direction to avoid a longitudinal scar that would result in a split in the nail.2 Further, a longitudinal biopsy of greater than 3 mm width will result in permanent nail dystrophy.2,14 With age, the matrix proliferation rate gradually decreases.12
The matrix epithelium is composed of at least two to three actively dividing, basal keratinocytes layers. These cuboidal cells are aligned in diagonal fashion thus allowing them to grow in an upward and outward direction. During process of maturation these cells loose 11nuclei, become flatter and get integrated into nail plate as onychocytes. These cells undergo maturation similar to corneocytes, however, they do not require keratohyalin granules. The matrix also contains few melanocytes along with few pigments containing keratinocytes. The density of melanocytes is same in both the proximal and distal matrix. Melanocytes located in proximal matrix are dormant while few melanocytes present in distal matrix are functional and thus most longitudinal melanonychia's originates in the distal matrix. These melanocytes are normally inactive in fair skinned individual, but may become activated by various endogenous and exogenous causes like hormonal disorders, trauma, drugs and photochemotherapy.3,12
The dermis of nail matrix is a relatively loose connective tissue layer of up to 1 mm in thickness and overlies the very distal fibers of extensor tendon insertion. It has very little subdermal fat.12
Nail Bed and Hyponychium
Nail bed is the region of nail which extends from the distal margin of lunula to the hyponychium (Figure 2.2).12 It was also considered as ventral or sterile matrix. The latter terminology had originated because it was believed that it did not contribute to the nail plate substance except for a thin layer of keratin, which ensured a firm attachment with the nail plate and permited it to slide over the nailbed.2 However, the epidermal keratinocytes of the nail bed have been seen to differentiate into nail plate cells which get incorporated into the ventral nail plate. Indeed, approximately 79% of nail thickness was contributed by the nail matrix, and 21% by the nail bed in a study on 20 big toe nails.16 Thus, the nail bed also contributes to the emerging nail plate. After removal of nail plate a unique pattern of longitudinal epidermal ridges stretching to the lunula is revealed. Undersurface of the nail plate after nail avulsion also shows a complementary set of ridges which are absent in the matrix epithelium. The blood vessels of nail bed are oriented in the same axis and this explains the splinter hemorrhages in nail bed and also why fusiform nail bed biopsies should always be performed in a longitudinal direction.2,12 Nail bed loses these longitudinal ridges shortly after loss of overlying nail plate. Probably ridges are generated at the margin of the lunula on the ventral surface of nail to be imprinted upon the nail.12
The epidermis of nail bed is thinner at most of region while it becomes thicker at nail folds where it forms rete ridges. It has no granular layer except in disease conditions. It also has sparse dermis, with little fat, firm collagenous tissue adhered to underlying periosteum and no sebaceous and follicular appendages. Sweat ducts are present at the distal margin of nail bed.12 Polarization microscopy shows that the keratin fibers run obliquely from the matrix and nail bed up to the nail plate, which may explain why the proximal nail avulsion technique is the least traumatic.2
Hyponychium and Onychodermal Band
The onychodermal band is an ill-defined transverse band above the nail bed approximately 1 to 1.5 mm in width, deep pink in color, which marks the transition to the hyponychium (Figure 2.2). Its integrity provides protection to the nail bed.2 The hyponychium lies between the distal ridge and the nail plate. The distal ridge is visible by 10th week of gestation.12 The hyponychium is comprised of a tough keratin layer that seals the subungual space and provides barrier function to the penetration of foreign bodies, dirt and the invasion of pathogens that cannot digest keratin. Thus, the integrity of the hyponychium is vital for a healthy nail bed and nail plate adhesion. Additionally, it may pose as an obstacle to penetration by a surgical instrument, such as an elevator during nail avulsion. The white appearance of central band 12represents transmission of light from the digit tip through the stratum corneum and up through the nail. It is not perceptible in some individuals while it is highly prominent in others. The surrounding pulp skin is richly innervated and contains nervous end organs, such as Meissner's and Vater-Pacini bodies.2
The hyponychium and onychodermal band may also give rise to subungual hyperkeratosis in response to trauma, infections and some diseases like pachyonychia congenita and pityriasis rubra pilaris. Hyponychium and nail bed can also give rise to pterygium inversum unguis, which is characterized by fibrotic scar tissue extending from free edge of nail plate to nail bed. It is seen in scleroderma, leprosy and traumatic injuries. The hyponychium and overhanging free nail act as a recess and thus as a reservoir for microbes, relevant in surgery and for the dissemination of infection. The various microbes include Staphylococcus epidermidis, yeast and moulds.12 Additionally, transmission of Helicobacter pylori from hand-to-mouth corresponding to a high incidence of carriage of these underneath the nail and seroprevalence for anti H. pylori antibodies has been reported.17
Nail Fold
Nail unit has got proximal and lateral nail folds (Figure 2.1). These nail folds enclose more than 75% of its periphery. They also provide a physical seal against the penetration of exogenous materials to subungual and proximal regions and correctly direct the nail growth.12 The proximal nail fold is of crescentic shape, sharply angulated at the free margin and has three parts.2,12 Its upper part is normal glabrous skin, while its distal margin at nail plate forms cuticle. The dorsal aspect of proximal nail fold is devoid of hair follicle, sebaceous structures and dermatoglyphic findings and ventral nail fold also lacks rete ridges. In healthy nail conditions, cuticle is firmly adhered to dorsal aspect of nail plate, achieving a seal.12 The cuticle is formed by the horny layer of the epidermis of the undersurface of the proximal nail fold which is attached to the surface of the nail plate. As the nail plate grows, the keratin from under the proximal nail fold gets partially detached from the nail plate to mostly form the cuticle. Thus, the loss of the cuticle can be attributed to the absence of proximal nail fold and nail plate attachment, cessation of nail growth, or thickening of the free margin of the proximal nail fold.1,2 In various dermatoses (chronic paronychia, collagen vascular disorders), cuticles can be affected and thus act as portal for entry of different allergens and microbes. Its ventral aspect is opposed to the dorsal aspect of nail. The proximal nail fold has shorter rete ridges and also has a granular layer. It shows differential expression of keratin on its dorsal and ventral aspects, which can be different from other components of nail unit as well. The proximal nail fold plays an important role in the following.12
- It may contribute to formation of nail plate through putative dorsal matrix on its ventral aspect.
- It may influence the direction of nail plate growth by directing it obliquely over the nail bed.12
- Nail fold capillaries studies can provide important information regarding various diseases and their prognosis.18
- It can also affect nail plate in various nail fold pathologies.12
A distal nail fold forms only in the absence of the nail plate as can be commonly seen after traumatic or surgical avulsion of the big toenail; but it usually disappears again following regrowth of the nail plate. However, in chronic disease if it becomes fibrotic, it serves as an impediment to the outward growth of the nail plate and may require surgical wedge excision from the pulp of the digit.213
The lateral nail folds are extensions of skin surface of sides of the digits and join the nail bed on its medial aspect. Its epidermal structure is comparable to normal skin. It can be affected in various dermatoses and traumatic conditions to give rise to soft tissue hypertrophy.12
The other cells that deserve mention include:
Langerhans Cells
Langerhans cells are dendritic antigen processing and presenting cells. They are more numerous in proximal than in the distal nail matrix. Similar to epidermis, these cells are predominantly located in the suprabasal layers. However, they may occasionally be seen within the basal layer of the nail matrix epithelium.3,12 They are more common in the proximal than in the distal matrix. Langerhan cells present in the proximal nail matrix region shows reduced expression of MHC class II in contrast to the distal nail epithelium and periungual skin; thus making nail immune system different from skin immune system and making it a relatively immune privilege site. This may serve to suppress inflammatory damage to the frequently traumatized proximal regenerative unit to ensure integrity of the nail.19
Merkel Cells
Merkel cells also been demonstrated in the nail matrix. Their density is possibly influenced by age; with these cells being more numerous in fetal than in adult nails.12 Merkel cells are neuroendocrine cells that are sparsely distributed in the epidermis, oral mucosa, vaginal mucosa, palms, finger pads, proximal nail folds, dorsa of the feet, eccrine glands and hair follicles. In a study on fetal and adult nails, Merkel cells were detected in the ventral matrix of all the specimens; they were sparsely distributed in both the proximal and the distal portions of the matrix and were not restricted to the basal zone of the epidermis but were also found in the suprabasal layers of the nail matrix epithelium. Merkel cells are responsible for light touch and are likely an indispensible part of the somatosensory system.20
Vascular Supply
The nail organ has a rich blood supply.2,3 The radial and ulnar arteries supply deep and superficial palmar arcades which act as large anastomoses between the two vessels (Figure 2.4). These arcades gives branches which run along the phalanges. Each digit is supplied by four arteries, two on either side.21 The proper digital arteries, the small dorsal and bigger volar arteries, originate close to the metacarpophalangeal joint from the common digital arteries.13

Consequently, flap should be harvested from the metacarpal joint toward the interphalangeal joint, to preserve the point of rotation proximally to the proximal third of the proximal phalanx in order to keep safe at least three to four nutrient cutaneous branches. The proper dorsal digital arteries are small and are branches of the radial artery. These dorsal arteries anastomose with superficial and deep palmar arches and the palmar digital vessels before passing distally into the finger. The main source of blood supply to fingers is the ulnar proper palmar digital arteries, which in turn, receive contributions from superficial and deep palmar arcades. The palmar arches are located underneath the maximal padding of finger pulp and tucked into a recess behind phalangeal bone. This protective position of palmar arches prevents occlusion of blood supply from sustained pressure while the fingers are held in a maintained grip.21,22 The vessels give rise to capillaries which run obliquely in the matrix and the nail bed. It is postulated that the direction of the capillaries is responsible for the direction of the growth on the nail plate, cuticle and the proximal nail fold. The formation of hang nails with a direction parallel to the nail surface may be attributed to the above.2
The superficial arcade lies just distal to the distal interphalangeal joint and it supplies the nail fold and extensor tendon insertions and intermediate nail matrix. The subungual region is supplied by distal and proximal subungual arcades, arising in turn, from an anastomosis of the palmar and dorsal nail fold arches. These vessels are tortuous which protects them from kinking and occlusion which is highly probable in an articulated longitudinal structure.18,21
Venous Drainage
Venous blood is drained from fingers by superficial and deep venous systems. The deep venous system corresponds to the arterial supply with the exception that the large collecting veins lie in the lateral nail folds of the nail and form an arch in the proximal nail fold.2,12 Superficial venous system comprises of dorsal and palmar digital veins. These veins show prominent branching network especially over dorsal aspect of finger.21,22 Little is known about the lymphatic drainage of the nail organ.2
Impairment of arterial supply can have a profound effect upon the finger pulp and nail unit. Impaired arterial supply in patients with peripheral vascular disease can result in paronychia, brittle fingernails, gangrene, Beau's lines and yellow discoloration. Prolonged immobilization of digits can cause diminish blood supply and thus decrease rate of growth. Conversely, increased nail growth has been seen with arteriovenous anomalies due to increased blood flow.22
Glomus Bodies
Small muscular arteries connect with the neurovascular glomus bodies.2 Glomus body is a small conglomeration of plexus of cavernous blood vessels and is also called the “peripheral heart of Masson”.3,11 It is an end organ apparatus in which there is an arteriovenous anastomosis bypassing the intermediary capillaries. Each glomus body is an encapsulated oval organ around 300 μm long composed of a tortuous vessel joining an afferent artery and venule, a rich nerve supply, a capsule and the Sucquet–Hoyer canal. The Sucquet–Hoyer canal is surrounded by cuboidal epithelial and smooth muscle or pericyte origin (Zimmerman type). Digital nail beds contain 93-501 glomus bodies per cm.3 They lie parallel to the capillary reservoirs which they pass.11,22 Glomus bodies increase in number towards the distal nail bed. They are vital in the maintenance of peripheral circulation under cold conditions.3,11 They contract asynchronously with associated arterioles such that, arterioles constrict and the glomus bodies dilate.1115
Nail Fold Vessels
The nail fold capillary network is similar to cutaneous plexus comprising of capillary loops in tiers of uniform size, with peaks equidistant from the base of cuticle. At the microvascular level, there are three patterns. Within the matrix, the vessels are longitudinal with a helicoid twisting; in the nail bed and proximal nail fold, they are longitudinal without any tortuosity. This pattern is reflected in the appearance of splinter hemorrhage. Finally, in the digit pulp, the vessels follow the pattern of dermatoglyphics.3
The venous arm is more dilated and tortuous than the arterial arm. There is also wide variation in morphology amongst general population. The capillary density in toe nail fold is higher than the finger nails. Nail fold capillaries can be visualized using a 4x magnifying lens, dermatoscope or an ophthalmoscope. These nail fold capillaries are affected in connective tissue disorder and bears prognostic significance. Various pathological changes include venous plexus visibility, density of capillaries, avascular fields, hemorrhages, giant capillaries and cessation of blood flow following cooling. Nail fold capillaries dilatation is more commonly seen in limited variety of systemic sclerosis, however, capillary drop out are preferentially seen in diffuse cutaneous systemic sclerosis. These can also be used to distinguish primary versus secondary Raynaud's as the latter will show capillary fold abnormalities. The underlying postulated mechanisms include impaired fibrinolysis, macroglobulinemia and cryoglobulinemia. Further, nail fold biopsy may be useful in detecting amyloid deposit or subintimal hyalinosis.18,22
Nerve Supply
In the hand, sensory supply is by median and ulnar nerve predominantly and partly by radial nerve. Median nerve supplies the volar surface of thumb, index, and middle finger as well as radial half of ring finger. Ulnar nerve supplies the ulnar half of ring finger and little finger whereas radial nerve supplies only proximal half of dorsal aspect of digit 1 through 3 and the radial half of dorsal aspect of proximal half of ring finger (Figure 2.5). Thus a median nerve block is required for surgeries over first 3½ finger nails and an ulnar nerve block for rest of the fingernails.12,22

Paired proper volar and dorsal nerves run at the sides of the flexor tendon and with the dorsal neurovascular bundles. Digital block anesthesia takes advantage of the relative fixity of the proper digital nerves adjacent to the proximal phalanx. However, injection of a large amount of anesthetic drug in this confined space may result in vascular spasm resulting in digital necrosis.13 There is no definitive consensus as to which digits has which type of innervations of their tips; however, it is generally assumed that the index, middle, and ring fingertips get their innervations from the palmar digital nerves which divides distally into three branches to the proximal nail fold, the matrix, and the nail bed, whereas the thumb, little finger, as well as the other toe tips is innervated by the dorsal nerves (Figure 2.6).2,11 The former is the rationale to perform the transthecal anesthesia for nail surgery of the long fingers because the volar nerves run in close proximity to the flexor digitorum tendon; however, recently transthecal anesthesia also has been found to be effective in the little finger and big toe. It has been proposed that the distal three branches also can be anesthetized by a distal wing block.2 However, further systemic research is required to further clarify the sensory innervations as it is important for understanding of transthecal block anesthesia.
Biochemistry
The nail plate, like hair consists primarily of filamentous proteins, the keratins, embedded in an amorphous matrix containing proteins rich in cysteine; besides water, lipid and trace elements.4,11 Keratins belong to the intermediate family of proteins that form the cytoskeleton of all epithelial cells.11 Keratins have been classified as soft epithelial or hard trichocyte keratins. The latter owing to their high sulphur content impart a rugged physical quality and are characteristically detected in the nail and hair. Keratins can be segregated into acidic and basic proteins on electrophoresis and are present in tissue as heterodimers of coupled acidic and basic protein which subsequently are assembled into protofilaments.3


The high stability of nail keratins can be attributed to the central helical core of proteins and the numerous disulphide bonds present.11
There is considerable regional variation in the expression of various keratins within the nail (Figure 2.7).11 Immunohistochemistry of the normal nail epithelium demonstrates that the nail bed and matrix principally contain K5/K14 which is the keratin synthesized in normal basal layer epithelium. In addition, K 6/K16 and K17 have been demonstrated in the nail bed and not in the nail matrix which is remarkable as nail bed has a low proliferative rate and K6/K16 are characteristic of high proliferation activity evident in wound healing and psoriasis. The presence of this hyperproliferative keratin in nail bed imparts a potential to this structure to become hyperkeratotic in disease states.3,11 Indeed, missense mutation of the initiation peptide of K16 and K17 in some kindreds results in thickening of nail plate in pachyonychia congenita.3,23 Expression of keratins 6, 16, 17 extends to the digital pulp and is thought to provide resistance to trauma.21 Suprabasal keratins (K1/K10) are usually absent in the nail except in the proximal nail fold and germinative matrix but may be expressed where a granular layer develops in nail diseases like psoriasis or onychomycosis. Trichocyte keratins have also been detected in the nail unit.3,11 There are at least 10 hard keratins; of which Ha-1 is the largest fraction and is detected in the matrix.3
Nonkeratin proteins include involucrin, which is detected in the upper matrix and is necessary for the formation of cellular envelop; actin in the matrix and vimentin and desmin in the vessels. In addition, filaggrin has been demonstrated in the human nail and it is postulated that along with trichohyaline it may stabilize the keratin network. The basement membrane contains collagen VII, fibronectin, chondroitin sulphate and tenascin.22
The lipid content of the nail is between 0.1-1% and the predominant type is cholesterol. The water content is reduced as compared to the skin (varying from 7-12%). This low water content contributes to the rigidity of the nail. The nail is highly permeable to water and to a lesser extent alcohol. Some medicated lacquers may penetrate sufficiently to allow drug delivery. The other trace elements detected include calcium, sodium, magnesium, phosphorus, iron and copper.11
To conclude a thorough knowledge of the nail structure including biochemical composition, vascular and nerve supply is mandatory for a clear comprehension of diseases of the nail and for a successful and uneventful surgery on the nail apparatus.18
References
- Nail anatomy. [Online]. URL http://en.wikipedia.org/wiki/Nail_(anatomy). Accessed 3.7.2012
- Haneke E. Surgical anatomy of the nail apparatus. Dermatol Clin. 2006;24(3):291–6.
- de Berker DAR, Baran R. Disorders of nails. In: Burns T, Breathnach S, Cox N, Griffiths C (eds) Textbook of Dermatology. 8th Edition. Oxford: Wiley-Blackwell; 2010. p 65.1-65.57.
- Tosti A, Piraccini BM. Biology of nails. In: Freedberg IM, Eisen AZ, Wolff K, Goldsmith LA, Fitzpatrick TB (Eds). Dermatology in general medicine. 5th edition. New York: McGraw Hill; 1999. p 239-44.
- Janis JE (Eds). Nail bed injuries. Essentials of Plastic Surgery: A UT Southwestern Medical Center Handbook. St. Louis, Mo: Quality Medical Publishing, Inc.; 2007. p 560-7.
- Achten G. Normale histologie und histochemie desnagels. In: Jadassohn J (ed). Handbuch der Haut- und Geschlechtskrankeiten, Vol 1. Berlin: Springer-Verlag; 1968. p. 339–376.
- Manabe M, O'Guin WM. Existence of trichohyalin keratohyalin hybrid granules: co-localisation of 2 major intermediate filament-associated proteins in nonfollicular epithelia. Differentiation. 1998;58: 65–75.
- Dekio S, Jidoi J. Comparison of human hair and nail low-sulfur protein compositions on two dimensional electrophoresis. J Dermatol. 1989;16:284–8.
- Heid WH, Moll I, Franke WW. Patterns of expression of trichocytic and epithelial cytokeratins in mammalian tissues. II. Concomitant and mutually exclusive synthesis of trichocytic and epithelial cytokeratins in diverse human and bovine tissues. Differentiation. 1988;37:215–30.
- Ogden GR, Chisholm DM, Leigh IM, Lane EB. Cytokeratin profiles in dyskeratosis congenita: an immunocytochemical investigation of lingual hyperkeratosis. J Oral Pathol. 1992;21:353–57.
- Raja babu KK. Nail and its disorders. In: Valia RG, Valia AR (Eds). IADVL textbook and atlas of Dermatology. 2nd edition. Mumbai: Bhalani publishing house; 2001. p.763-98.
- de Berker DAR, André J, Baran R. Nail biology and nail science. Int J Cosmet Sci. 2007;29(4):241–75.
- Mclean WH, Rugg EL, Lunny DP, Morley SM, Lane EB, Swensson O, et al Surgical anatomy of the nail unit. Dermatol Surg. 2001;27(3):257–60.
- Lewis B L. Microscopic studies of fetal and mature nail and surrounding soft tissue. Arch Derm Syphilol. 1954;70:732–44.
- Embryologic, Histologic, and Anatomic Aspects. In: Histologic Diagnosis of Inflammatory Skin Diseases. [Online]. URL https://derm101.com/content/13357. Accessed on 1.7.2012.
- Johnston M, Schuster S. Continuous formation of nail along the bed. Br J Dermatol. 1993;128: 277–80.
- Dowsett SA, Archila L, Segreto VA, Gonzalez CR, Silva A, Vastola KA, Bartizek RD, et al. Helicobacter pylori infection in indigenous families of Central America: serostatus and oral and fingernail carriage. J Clin Microbiol. 1999;37(8):2456–60.
- Hasegawa M. Dermoscopy findings of nail fold capillaries in connective tissue diseases. J Dermatol. 2011;38(1):66–70.
- Paus R, Peker S, Sundberg JP. Biology of hair and nails. In: Callen JP, Horn TD, Mancini AJ, Salasche SJ, Schaffer JV, Schwarz T, Stingl G, Stone MS (eds). Dermatology. 2nd Edition. New Delhi: Elsevier Ltd; 2008. p 965-86.
- Cameli N, Ortonne JP, Picardo M, Peluso AM, Tosti A. Distribution of Merkel cells in adult human nail matrix. Br J Dermatol. 1998; 139: 541.
- Baserga M, Bonacci E, Cammarota MG, D'Amico N. Nailfold capillaroscopy in the study of microcirculation in childhood. Minerva Pediatr. 1996;48(7-8):297–301.
- Dawber RPR, de Berker DAR, Baran R. Science of the nail apparatus. In: Baran R, Dawber RPR, de Berker DAR, Haneke E, Tosti A (Eds). Diseases of the nail and their management. 3rd editon. Oxford: Blackwell science ltd; 2008. p 1-47.
- Mclean WHI, Rugg EL, Lunny DP, Morley SM, Lane EB, Swansson O, et al. Keratin 16 and 17 mutations cause pachyonychia congenital. Nature Genet. 1995;9:273–8.
Introduction
The nail unit is a unique appendage of skin which is designed to provide protection to the tip of digits and to strengthen the grip for holding things. It consists of nail matrix (NM), nail bed (NB), hyponychium, nail fold (NF) and the nail plate (NP). Nails also enjoy immense cosmetic importance and recent times are witnessing a great increase in the number of several nail art techniques for enhancing the beauty of nails. Derived from cells in the nail matrix which divide to form the nail plate, nail bed, nail matrix, nail fold and the hyponychium, the nail apparatus is a dynamic unit that continues to grow during life time (finger nails at a rate of 1 cm in 3 months and toe nails 1cm in 1 year).
Nail disorders encompass a wide variety of conditions exhibiting unique changes in different parts of the nail apparatus. Complaints related to the nail apparatus may be the only presenting complaints and call for a systematic approach to clinch the pathology or at times nail pathology is secondary to a primary cutaneous disorder or a systemic disease and both require a detailed history and complete clinical examination. Since the morphological 20changes brought about by different nail disorders are co-shared, hence it is imperative that relevant investigations be carried out to arrive at the correct diagnosis. The chapter shall be dealing with a stepwise approach to different nail diseases focusing on collection of sample and investigations.
Approach to various nail disorders should include a detailed history, clinical examination of nails, skin, hair and various systems and should be supplemented by simple office procedures, culture and microscopy, and other tests for clinching the diagnosis as and when needed.
History Taking
Detailed history should be taken from the patient which should include—duration of the nail diseases/changes, history of trauma, occupational history (chronic paronychia is more common in bartenders, beauticians and housewives). Personal history must be sought as to the number of times hands are washed, soap/detergent exposure, nail cosmetic and other topical agents used, exposure to dyes, nutritional aspects, history of acute diseases such as viral infections in the recent past, chronic diseases such as diabetes, malabsorption, peripheral vascular disease, connective tissue disease, thyroid dysfunction, alcoholism, drug intake, type of footwear used and trauma. A positive family history is noted in hereditary striate leukonychia.
Clinical Examination of Nail
Nail examination is usually neglected despite nails being an important source of clinical and diagnostic information. When examining the nails, one should examine all 20 nails with the digits relaxed. All nail polish and lacquer should be removed. Patient should avoid applying topical nail medicaments or cosmetics and should not trim the nail for some days to get longer nail for accurate nail examination. Use a hand lens preferably in natural day light. Skin, mucous membranes, hair and systemic examination should be done for evidence of disease. It is important to be aware of the common variations such as shape and size of nail, lunula which may differ in individuals. Pathological changes such as nail pits or splinter hemorrhages can be seen in normal individuals but are much fewer in number (involving 1 or 2 nails only). Nail ridges and grooves in one or two nails can be seen on the thumb nail and constitute a habit tic and mild roughness of nails is common in manual workers, labourers and old individuals.
The common nail disorders are enlisted in Table 3.1.
Diagnostic Tests in Nail Disorders
History and clinical examination provide useful clues to the provisional diagnosis which can be confirmed with the aid of certain simple procedures namely nail swab and nail scraping or clipping. Nail biopsy yields vital information but is considered in the end as it is time consuming and bears the risk of scarring. Advent of imaging techniques and dermatoscopy has opened newer vistas in the realm of nail disorders. These noninvasive techniques supplement the clinical findings. As healthcare practitioners, it is important to use every tool at our disposal to establish the correct diagnosis for patients.
Table 3.2 shows some common nail disorders with investigations indicated.
Nail Swab for Culture and Sensitivity Testing
The diagnosis of acute paronychia is confirmed by clinical examination and the purulent collection is sent for Gram stain, culture, and sensitivity to aid in treatment.
Direct Microscopic Examination
This is a rapid, simple and inexpensive technique to confirm the diagnosis of onychomycosis in a clinical setting.
Indications – KOH preparations are used to identify fungal elements in clinical specimens. The purpose is to provide descriptive morphological information to aid in the treatment of the infestation.
KOH digests proteins, lipids and most of the epithelia present but not the fungal cell walls which are resistant due to their polysaccharide chitin, a polymer of N-acetyl D-glucosamine. 10–20% KOH with or without dimethyl sulfoxide (DMSO) or other detergent is simple, cheap and most commonly used.
Specimen Collection with Precautions
Proper specimen collection is essential to avoid false-negative results and to eliminate contaminants. Figures 3.1A and B show the technique of specimen collection for direct microscopy. Separate samples should be obtained from fingernails and toenails, associated tinea pedis, or manuum.1 The specimen should be obtained when the patient has been off of both topical and systemic antifungal drugs for 2-4 weeks.2 The entire nail unit should be thoroughly cleaned with alcohol. The affected nail bed should be exposed by removing the onycholytic nail plate with a nail clipper and scraping the hyperkeratotic nail bed with a solid or disposable scalpel or curette and outermost debris should be discarded. Sampling of distal nail plate should be avoided as it frequently contains contaminants that may obscure the growth of pathogenic fungi and the hyphae at the distal end of the nail are less likely to be viable, hence less likely to grow on culture media.3 Fine shavings or minute clippings are preferred. Specimens must not be kept in moist media to avoid rapid multiplication of bacterial and fungal spores and should be processed within a week.2 Scrapings may be collected in a black paper or directly onto a slide. Potassium hydroxide 10% is added to the collected material and a cover slip is applied with little pressure to blot away the excess KOH and make the preparation even when examining 22under the microscope.
|
Should the mount dry then air pockets get formed under the cover slip, in that case one should add more KOH. For thick, hyperkeratotic specimens, leave the KOH preparation for ‘digestion’ and ‘clearing’ for 30 minutes to 2 hours. If there is only subungual debris or very small pieces, specimen can be examined within 10 minutes with 10-15% KOH. However, if large nail plate pieces are taken, they take a considerably longer time.3 For them, the sample should be broken into smaller parts initially itself and then incubated at 37°C for 1 minute and then examined.423

Figures 3.1A and B: (A) Technique of specimen collection for direct microscopy; (B) KOH is added to the nail scraping before microscopic examination
|
Results
- Initial examination is with low power magnification (10X) and low intensity of light with lowering of the condenser. Later, for a higher magnification (40X), the condenser should be higher for better illumination, to study the morphology of the fungus.
- Refractile, long, smooth, undulating, branching and septate hyphal filaments with or without arthroconidiospores are seen in dermatophyte involvement.
- The hyphal filaments seen by microscopy in nondermatophytic mold involvement of the nail, especially of the great toes, tend to be irregular, vesiculated, tortuous or pigmented.
- Dozens of hyaline, oval, budding (blastoconidiating) yeast cell forms with or without pseudo-hyphal filaments can be seen in candidal involvement.
- Fungal spore vary from 2-10 mm in diameter.

Figure 3.2 shows arthrospores in KOH s mear under high magnification.
Stains: Staining increases the sensitivity of direct examination by improving visualization of the fungal structures.
Table 3.4 shows some of the stains used.
Role of fluorochromes: They stain fungal cell wall (as they bind to chitin) and artefacts like some vegetable fibers. They greatly facilitate detection of hyphae and spores, only limitation being the requirement of fluorescence microscope. Some of the commonly used fluorochromes are calcofluor white (CW), Blankophor P Flussig, and Uvitek 2B. CW brightly fluoresce hyphae and conidia blue or green (depending on the filter used).
Conclusion: Direct microscopy cannot differentiate between species but can give a clue to the possible group of fungi. In expert hands, a positive KOH with clinical suspicion of onychomycosis is adequate evidence for diagnosis. A sensitivity between 50% and 80% has been ascribed to KOH examination.5–8
Fungal Culture
Culture was earlier considered the gold standard for diagnosis, being the only routinely available test which can identify the involved fungus. Reported sensitivity for culture varies from 25 to 80%.8
|
Up to 30% cases may have false-negative results especially when the sample is insufficient, taken from distal portions or is not crushed prior to inoculation.8, 9 Information regarding fungal vitality, as well as accurate identification of the pathogen is not available through direct examination alone, cultures are therefore important since identification at the species level which may be useful to initiate an appropriate treatment or for setting prophylactic measures relying on macroscopic and microscopic morphology.
Indications
- Suspected fungal infection (KOH preparation negative)
- To determine sensitivity to antifungal medications.
Specimen Collection with Precautions
- Clip nails up to yellowish, crumbly portion
- Clip a part of the crumbly portion and place on medium
- Gently scrape debris from under free edge of nail
Media
- Sabouraud's dextrose agar (SDA): Containing antibiotic(s) (chloramphenicol, gentamicin) and cycloheximide is commonly used as primary isolation medium. The incorporation of cycloheximide in the culture medium will prevent the growth of majority of molds and yeasts that could hamper the recovery of dermatophytes.
- Dermatophyte test medium (DTM) and dermatophyte identification medium (DIM).
- Specific media: Stimulate the conidiation and sometimes the production of pigments e.g. Borelli's lactrimel agar (BLA) and potato dextrose agar (PDA).
- Conidiation may also be stimulated on poor culture media e.g. Baxter's medium, Takashio's medium, malt agar or water agar.
- Phytone yeast extract agar (PYE) supplemented with antibiotics to inhibit the growth of bacteria is a nutritionally enriched medium.
- Many antifungal drugs currently used for treatment of dermatophytoses are retained for a long time within the horny layer of the epidermis and drug residues in the sample may inhibit the growth of the pathogen. To overcome this problem, a new medium called Combined deactivators-supplemented agar medium (CDSAM) (containing lecithin and polysorbate 80) was developed which minimised the carryover effect of antifungals.
Results
Nondermatophyte molds grow faster than dermatophytes and produce well-formed colonies within 1 week. Colonies of most dermatophytes are usually completely differentiated in 2 weeks. Cultures are incubated for three to four weeks and examined weekly. Fungal colonies are judged on the basis of growth patterns, color and microscopic formation of macro and microconidia or other typical growth features.12 If growth is seen on both types of media, the infective agent is probably a dermatophyte, whereas growth only on the cycloheximide-free 26medium indicates that the infective agent may be a nondermatophyte mold.13 Additional special culture media such as potato glucose agar or Urea Agar may be needed to definitively differentiate between dermatophyte species.12
Figure 3.3 shows the colony morphology of T. rubrum on the surface of SDA slant.
Conclusion: Cultures may remain negative inspite of the positivity of direct examination. These false-negative results may be related to an insufficient amount of material or a specimen poor in fungal elements, but also to a too short incubation time, a nonsuitable temperature or the presence of ‘contaminants’ which can prevent the development of the pathogen. False-negative results on Sabouraud's agar may also result from an anti-fungal treatment initiated before sampling.
Nailfold Capillaroscopy
Nailfold capillaroscopy (NFC) uses a lens that allows analysis of the capillary morphology and microcirculation of nailfold. It is used as a noninvasive, simple, repeatable, highly sensitive and inexpensive method of evaluating microvascular abnormalities in rheumatic diseases. Nailfold capillaroscopic analysis was mainly developed at the end of the last century, and the most recent development is computer-based nailfold video capillaroscopy system, which can record images, enhance image quality, and show real-time blood flow and velocity. In addition, laser Doppler imaging (LDI) is a relativity new method for measuring the microcirculation of peripheral perfusion. Ideally, patients should be seated indoors for at least 15 minutes and allowed to acclimatize to a room temperature of 20°C-24°C before the examination. After depositing a drop of immersion oil on the nailfold bed to improve resolution, all nailfolds in each finger should be examined. The nailfold capillaries of the fourth and fifth fingers of the nondominant hand are tested to achieve the best visibility. The skin in these areas is more transparent than that in other fingers.
Capillaroscopic Microvascular Morphology
The following microvascular morphology should be observed and documented: tortuosity, loop size, density, angiogenesis, capillary loss, microbleeding, subpapillary venous plexus, and architectural structure.

Figure 3.3: Colony morphology of T. rubrum: White colored cottony growth on the surface of SDA slant
The most important and well-defined capillary abnormalities detectable by capillaroscopy have been described in patients with systemic sclerosis (SSc). They are classified into three types: normal, nonspecific, or sclerodermatous; enlargement of capillary loops, loss of capillaries, disruption of capillary bed and distortion and budding of capillary or hemorrhage. The term ‘SSc pattern’ includes, all together, these sequential capillaroscopic changes typical to the microvascular involvement in SSc. The capillaroscopic aspects observed in dermatomyositis and in the undifferentiated connective tissue disease are generally reported as ‘SSc-like pattern’.
Figure 3.4 shows a nailfold capillaroscope.
Plain X-Ray
An X-ray investigation should be carried out on all swellings in or around the nail apparatus, particularly those affecting a single digit, to exclude osteoma. Role of X-ray also comes in connective tissue disorders, especially systemic sclerosis, in which phalangeal absorption, calcinosis, erosive arthropathy, osteolysisecially etc. can be seen.
Nail Unit Biopsy
Nail biopsy is a useful technique to obtain a diagnosis of a clinically ambiguous nail condition that is not diagnosable by history, clinical appearance, and routine mycology. The procedure consists of obtaining specimens of either the nail plate, nail bed, nail matrix, proximal or lateral nail fold, hyponychium, alone or in combination to be able to arrive at a precise diagnosis of a nail pathology. This analysis is efficient though constraining for the patients. It does not allow precise identification of the pathogen or direct examination, however, nail plate biopsy using PAS stain is a very sensitive technique (in fact current gold standard for diagnosis of onychomycosis and is indicated if other methods are negative and clinical suspicion is high).14

Indications
- To differentiate between onychomycosis and nail psoriasis.
- To differentiate between subungual hematoma and melanoma.
- To diagnose benign and malignant subungual and periungual tumors.
- To diagnose the cause of nail dystrophies, e.g. nail lichen planus or nail psoriasis.
Prerequisites for a Nail Biopsy15
- Knowledge of nail anatomy.
- Patient selection—Ideal candidate is one in whom either there are no skin lesions or he is not contributing towards a diagnosis, as skin biopsy is always a safer and easier procedure than nail biopsy.
- An informed written consent should be taken.
- Preoperative medication—Antibiotics, antifungal, and anti-inflammatory drugs should be given.
Contraindications
Peripheral vascular disease, uncontrolled diabetes or arterial insufficiency.
Table 5 shows sites for nail biopsy.
Instruments Required
- No. 10/15 surgical blade
- No. 3 BP scalpel handle
- Nail spatula
- Nail splitter
- Biopsy punches (3 mm/4 mm)
- Skin hook
- 26 G needle
- artery forceps
- Curved forceps
- Scissors
- Needle holder
- 6-0 vicryl suture
- 3-0 to 6-0 prolene suture
- Tourniquet.
Procedure16
1. Anesthesia: Proximal ‘ring block’ (at base of the digit) or distal ‘wing block’ (at proximal and lateral nail folds) with 1% xylocaine without adrenaline is given. Do not give more than 8-10 ML to avoid mechanical compression of the vasculature which might result in ischemia and digital necrosis.29
| |||||||||||||||||||||||||||||||||||||||||||||
2. Strict hemostasis: Bloodless field is achieved by proper exsanguination followed by basal tourniquet. The tourniquet should be released every 8-10 minutes to avoid ischemia.
3 a. Nail plate biopsy: It can be performed with shave or punch technique. In shave biopsy, scissors or scalpel can be used to remove wedge of tissue that includes the distal hyponychium and overlying dystrophic nail. In punch biopsy, 3 mm punch is driven through the nail plate upto the nail bed but not through it. The tip of 26 G needle is then driven through the center of the circularly incised nail plate upto the nail bed and is lifted out.
b. Nail bed biopsy:
- Single punch technique—Punch biopsy using 3 mm skin biopsy punch, is driven through the nail plate and the desired part of nail bed to the periosteum. The tip of 26 G needle is then driven through the nail plate of this cylindrical punch and its bound down tissue is then lifted out. The base is then cut with fine curved iris scissors.
- Two punch technique (Window technique)—A large sized punch, i.e. 4 mm is first used to drive, cut and remove only the circular 4 mm piece of nail plate. A smaller, i.e. 3 mm punch is then driven through the earlier made 4 mm window opening into the nail bed down to the periosteum and the tissue is then excised.
- Fusiform excisional biopsy—Partial or full nail plate avulsion is first carried out for better visualization of the nail bed. After marking, a fusiform excision directed longitudinally and 30extending deeply upto the periosteum is given with scalpel. Closure is done with absorbable 6-0 vicryl sutures.
c. Nail matrix biopsy: It can be done using either a 3 mm punch or by elliptical excision oriented transversely. Care should be taken to take the biopsy from the anterior segment of the matrix, thereby maintaining the distal lunular curve with nonviolation of the lunular edge. This will avoid nail plate deformities and yield better cosmetic results.
- Nail spatula is inserted between the nail plate and the proximal nail fold. Bilateral longitudinal incisions are taken from the junction of the lateral and proximal nail folds and extending 6 mm proximally upwards. With skin hooks, the proximal nail fold is reflected to see the extent and exact location of the pathological process.
- Nail plate may or may not be avulsed.
- 3 mm punch or transverse fusiform biopsies can then be taken from the anterior segment of the matrix. If longitudinal fusiform biopsy through the entire length of matrix is necessary, then it should not exceed 3 mm in width in order to avoid permanent deformity. The depth of the 3 incisions should be upto the periosteum. In transverse fusiform excision, the distal edge of the eclipse should be parallel to the curve of the lunula. While the punch incision is left to heal by secondary intention, both longitudinal and transverse fusiform incisions should be closed with 6-0 vicryl sutures. The reflected proximal nail fold is then returned to its natural position and sutured with 6-0 prolene.
d. En bloc nail unit biopsy: This biopsy serves to provide chronology of the pathological process as it involves longitudinal fusiform incision taken from proximal nail fold to tip of finger and includes lateral nail fold, nail plate, nail bed and matrix. Maximum width of incision should not be more than 3 mm and it should not extend bone deep. After excising, the tissue is released with use of iris scissors. The defect is closed with careful opposition of proximal nail fold, matrix and hyponychium using 3-0 and 6-0 prolene.
4. Dressing: Local pressure dressing with antibiotic ointment and removal of basal tourniquet should follow.
5. Postoperative medications: Antibiotics, and anti-inflammatory drugs are given for 7-10 days. Sutures are removed after 10 days.
Figures 3.5 A to H depict the stepwise procedure of nail matrix biopsy.
Complications: Pain, bleeding, infection, permanent nail dystrophy.
Conclusion: Nail biopsy is a useful diagnostic modality for nail disorders especially psoriasis, nail lichen planus, onychomycosis, etc. The trick lies in the area to be biopsied in different disorders. A competent dermatopathologist who is familiar with the basic histopathologic features of the nail is also an essential prerequisite. Proper embedding and sectioning of the NB specimen is essential prior to this. However, there is still a possibility of not achieving a diagnosis even after nail biopsy. It should be the preferred diagnostic tool, especially in cases where the diagnosis of onychomycosis is not certain and in those already on antifungal treatment.17
Dermatoscopy
Dermatoscopy is also known as dermoscopy and epiluminescence microscopy. It is the examination of skin using dermatoscope and is mainly used for distinguishing pigmented benign 31and malignant lesions.

Figures 3.5A to H: (A) Proximal ring block, (B) Strict homeostasis achieved by proper exsanguination followed by basal tourniquet; (C) Nail spatula is inserted between the nail plate and the proximal nail fold, (D) Bilateral longitudinal incisions are taken from the junction of the lateral and proximal nail folds and extending 6 mm proximally upwards, (E) With skin hooks, the proximal nail fold is reflected to see the extent and exact location of the pathological process, (F) 3 mm punch can then be taken from the anterior segment of the matrix, (G) The reflected proximal nail fold is then returned to its natural position, (H) 6-0 Prolene sutures given
In nail unit, it is mainly used for patients presenting with melanonychia.18 Park et al have introduced a handy portable hand-held digital dermoscope (USB Microscope M2, Scalar Corporation, Tokyo, Japan) which can be used to study the nail fold capillary changes while sitting in a high-volume outpatient setting.19 It has the advantages of obtaining microscopic images on a computer monitor in real time; this makes the system more practical than other conventional dermoscopy systems using a camera that requires the development process. In addition, it has a polarizing light mode that minimizes the light reflection from the stratum corneum caused by the difference in the reflective index between the air and the stratum corneum. Thus, it does not require mineral oil or other immersion agents to reduce the light reflection. To improve the quality of the dermoscopic image, gel is applied to the nail. The nail plate is examined from above as well as end-on (the free edge of the nail). Seen end-on:
- Pigment in the top of the nail plate has its origin in the proximal matrix.
- Pigment at the bottom of the nail plate has its origin in the distal matrix or nail bed.

Newer Diagnostic Modalities in Diagnosis of Nail Disorders
Nail apparatus has been deprived of investigative medical imaging until recently. However lately there has been a growing interest in noninvasive examination techniques. This includes USG, magnetic resonance imaging (MRI), optical coherence tomography (OCT), confocal laser scanning microscopy (CLSM) and improvised dermoscopy instruments. The main indication for these new techniques is the investigation of nail tumors.
I. Ultrasound
USG of nail requires high resolution ultrasound machines and high frequency ultrasound probe. It is a good tool to diagnose cystic tumors of nail including myxoid cyst, synovial cyst and collections like subungual hematoma or abscess. However it is not a good tool for the diagnosis of solid tumors like melanoma or squamous cell carcinoma.20
Blood flow in the nail unit can be studied with color Doppler and power angio. These techniques are useful in the diagnosis of vascular tumors like glomus tumor.
Newer technique called real time compound spatial imaging is evolving.21 It provides instantaneous integration of overlapping USG scans taken at different angles to produce a compound image.
II. Magnetic Resonance Imaging
High-resolution MRI provides an accurate analysis of the nail apparatus. Nail unit tumors have atypical presentations as the lesions in nail matrix present with secondary nail plate changes and nail bed tumors are obscured by the nail plate. It has been used mainly for the diagnosis of nail unit tumors especially glomus tumor.22, 23 In most cases the tumor is located in the subungual area, in the supporting tissue of the nail bed or matrix. These locations are 33the most difficult to depict with USG when the tumor is smaller than 3 mm. Other indications include myxoid cyst, implantation epidermoid cyst, ganglion cyst, onychomatricoma, exostosis, fibrokeratomas and osteochondromas.
III Optical Coherence Tomography (OCT)
In OCT the infrared light reflected from the skin is measured and the intensity is imaged as a function of position. This technique provides images of tissue pathology in situ with a high axial resolution.24 Fungal elements are detectable as highly scattering elongated structures inside the nail plate, in the middle of the areas of homogeneous decrease in signal intensity.4 The low scattering areas represent the surrounding lacunae of the hyperkeratotic nail plate. The results of OCT are comparable to the findings of PAS-stained specimen and have been found to be superior to KOH preparations and cultures.25 Thus, OCT is a reliable, easy to use, noninvasive and nondestructive method to visualize fungal elements in vivo, even in cases with false negative KOH-preparation and culture. Furthermore, it offers the opportunity to screen several areas within a nail plate and hence, detect persisting fungal elements during local or systemic therapy.
IV Confocal Laser Scan Microscopy
Confocal laser scan microscopy is a new noninvasive diagnostic tool which is becoming increasingly popular. It can visualize cell structures of the skin up to a depth of 300 μm in vivo.18 It is based on the principle of increasing optical resolution and contrast of a micrograph by using point illumination and a spatial pinhole to eliminate out-of-focus light in specimens that are thicker than the focal plane. It also enables the reconstruction of three-dimensional structures from the obtained images. Researchers have found it to be faster and more accurate than the conventional microscope used in potassium hydroxide (KOH) preparations in the diagnosis of onychomycosis.26, 27
V Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF MS)
This technique is based on the detection of biochemical characteristics which are a result of the activity of mycological infections or noninfectious diseases. These are represented by proteolytic degradation products of native nail proteins.28 The technique analyses the protein patterns of nail samples by using small amounts of peptides derived from tryptic digests of collected samples. The peptide patterns of affected samples are identified by comparison with known peptide spectra from nail disorders stored in an already existing data base. The technique does not require any living or nonliving fungal material to prove or to rule out onychomycosis. It is also able to discriminate between onychomycosis and nonfungal nail disorders offering a distinct advantage over the conventional methods of KOH and culture which only prove or rule out presence of fungi.
VI Phase Contrast Hard X-ray Microscopy
This technique uses phase contrast microscopes utilizing synchrotron radiation which can provide a precise image of an extremely small object because of its brightness and high spatial resolution (upto 70 nm).29 The major advantage with this technique of microscopy is that, just 34like histopathology, it provides direct evidence of fungal invasion of nail plate, showing that the fungi are pathogenic.4
VII Polymerase Chain Reaction (PCR)
Given the degree of uncertainty of conventional methods for diagnosis of onychomycosis, various molecular biological techniques using PCR assay have been evaluated.4 They can provide a rapid, stable and accurate alternative for identifying pathogenic fungi both from the nail samples and from the fungal colonies. The methods used in samples from cultured colonies include arbitrarily primed PCR, PCR-restriction fragment length polymorphism (RFLP), double-round PCR, real-time PCR and PCR-direct sequencing.30 PCR is specific, requires no morphologic expertise, has relatively good sensitivity, and gives faster results.18
References
- Baran R, Hay R, Haneke E, Tosti A (Eds). Onychomycosis: The current approach to diagnosis and therapy. London: Informa Healthcare; 2006.
- Singal A, Khanna D. Onychomycosis: Diagnosis and management. Indian J Dermatol Venereol Leprol. 2011;77(6):659–72.
- Hay RJ, Ashbee HR. Mycology. In: Burns T, Breathnach S, Griffiths C, Cox N (Eds). Rook's Textbook of Dermatology. (8th edn). UK: Wiley-Blackwell Publisher, 2010;36.1-36.93.
- Grover C, Khurana A. Onychomycosis: newer insights in pathogenesis and diagnosis. Indian J Dermatol Venereol Leprol. 2012;78(3):263–70.
- Wilsmann-Theis D, Sareika F, Bieber T, Schmid-Wendtner MH, Wenzel J. New reasons for histopathological nail-clipping examination in the diagnosis of onychomycosis. J Eur Acad Dermatol Venereol. 2011; 25: 235–7.
- Shenoy MM, Teerthanath S, Karnaker VK, Girisha BS, Krishna Prasad MS, Pinto J. Comparison of potassium hydroxide mount and mycological culture with histopathologic examination using periodic acid-Schiff staining of the nail clippings in the diagnosis of onychomycosis. Indian J Dermatol Venereol Leprol. 2008;74: 226–9.
- Gianni C, Morelli V, Cerri A, Greco C, Rossini P, Guiducci A, et al. Usefulness of histological examination for the diagnosis of onychomycosis. Dermatology 2001; 202: 283–8.
- Lawry MA, Haneke E, Strobeck K, Martin S, Zimmer B, Romano PS. Methods for diagnosing onychomycosis: A comparative study and review of the literature. Arch Dermatol. 2000; 136: 1112–6.
- Weinberg JM, Koestenblatt EK, Tutrone W, Tishler HR, Najarian L. Comparison of diagnostic methods in evaluation of onychomycosis. J Am Acad Dermatol 2003; 49: 193–7.
- Shemer A, Trau H, Davidovici B, Grunwald MH, Amichai B. Nail sampling in onychomycosis: Comparative study of curettage from three sites of the infected nail. J Dtsch Dermatol Ges. 2007;5: 108–11.
- Shemer A, Davidoci B, Grunwald MH, Trau H, Amichai B. Comparative study of nail sampling techniques in onychomycosis. J Dermatol. 2009;36: 410–4.
- Seebacher C, Brasch J, Abeck D, Cornely O, Effendy I, Ginter-Hanselmayer G, et al. Onychomycosis. J Dtsch Dermatol Ges. 2007; 5: 61–6.
- Chang A, Wharton J, Tam S, Kovich OI, Kamino H. A modified approach to the histologic diagnosis of onychomycosis. J Am Acad Dermatol. 2007; 57: 849–53.
- Nazarian RM, Due B, Deshpande A, Duncan LM, Misdraji J. An improved method of surgical pathology testing for onychomycosis. J Am Acad Dermatol. 2012;66(4):655–60.
- Grover C, Chaturvedi UK, Reddy BS. Role of nail biopsy as a diagnostic tool. Indian J Dermatol Venereol Leprol. 2012;78(3):290–8.
- Savant S. In: Savant S, editor. Textbook of dermatosurgery and cosmetology 2nd (edn). Mumbai: ASCAD; 2008. p 235-53
- Rich P. Nail biopsy: Indications and methods. Dermatol Surg. 2001; 27:229–34.
- Dogra S, Yadav S. What's new in nail disorders? Indian J Dermatol Venereol Leprol. 2011; 77(6):631–9.
- Park JH, Lee DY, Cha HS, Koh EM. Handheld portable digital dermoscopy: Routine outpatient use for evaluating nail-fold capillary changes in autoimmune connective tissue diseases. J Eur Acad Dermatol. Venereol. 2009; 23: 207.
- Wortsman X, Jemec GB. Ultrasound imaging of nails. Dermatol Clin. 2006; 24: 323–8.
- Wortsman XC, Holm EA, Wulf HC, Jemec GB. Real-time spatial compound ultrasound imaging of skin. Skin Res Technol. 2004; 10: 23–31.
- Holzberg M. Glomus tumor of the nail: A ‘redherring’ clarified by magnetic resonance imaging. Arch Dermatol. 1992;128:160–2.
- Matloub HS, Muoneke VN, Prevel CD, Sanger JR, Yousif NJ. Glomus tumor imaging: Use of MRI for localization of occult lesions. J Hand Surg Am. 1992; 17: 472–5.
- Pierce MC, Strasswimmer J, Park BH, Cense B, de Boer JF. Advances in optical coherence tomography imaging for dermatology. J Invest Dermatol. 2004; 123: 458–63.
- Abuzahra F, Spöler F, Först M, Brans R, Erdmann S, Merk HF, et al. Pilot study: Optical coherence tomography as a non-invasive diagnostic perspective for real time visualization of onychomycosis. Mycoses. 2010; 53: 334–9.
- Kaufman G, Horwitz BA, Duek L, Ullman Y, Berdicevsky I. Infection stages of the dermatophyte pathogen Trichophyton: Microscopic characterization and proteolytic enzymes. Med Mycol. 2007; 45: 149–55.
- Hongcharu W, Dwyer P, Gonzalez S, Anderson RR. Confirmation of onychomycosis by in vivo confocal microscopy. J Am Acad Dermatol. 2000; 42: 214–6.
- Pföhler C, Hollemeyer K, Heinzle E, Altmeyer W, Graeber S, Müller CS, et al. Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry: A new tool in diagnostic investigation of nail disorders? Exp Dermatol. 2009;18:880–2.
- Lee O, Ha S, Lee G, Kim J, Huang J, Jin K, et al. Phase contrast hard X-ray microscopy using synchrotron radiation for the diagnosis of onychomycosis. Microsc Res Tech. 2010; 73: 1110–4.
- Ebihara M, Makimura K, Sato K, Abe S, Tsuboi R. Molecular detection of dermatophytes and nondermatophytes in onychomycosis by nested polymerase chain reaction based on 28S ribosomal RNA gene sequences. Br J Dermatol. 2009;161:1038–44.
Introduction
Dermatoscopy (also known as dermoscopy or epiluminescence microscopy or skin surface microscopy) is a noninvasive in vivo method of rapid, magnified examination of skin and its appendages. It often leads to visualization of features imperceptible to naked eye. The dermatoscope essentially consists of a magnifying lens (usually ×10) with an in built illuminating system and a transparent contact plate. Some dermatoscopes in addition capture and process images and are called digital epiluminescence dermatoscope. Videodermatoscopy is a modification where images are obtained with a video camera and images can be visualized on a monitor connected to it.
There are two methods of dermatoscopy : contact and noncontact. The contact method which has better illumination and resolution is commonly used for examination of nail. The traditional dermatoscopes used nonpolarizing light and needed a linkage fluid between the instrument and skin surface. The modern dermatoscopes have eliminated the need for linkage fluid by using polarized light to minimize skin surface reflections. But for examination of nail apparartus it is recommended to use a gel as immersion medium because of its decreased viscosity that permits it to stay on the nail plate and fill any concavities without rolling off. Many newer dermatoscopes have option of both polarized and nonpolarized light.37
History
Skin surface microscopy was first started by Kolhaus in 1663 for studying the small vessels in nail folds.1,2 In 1878, Abbe described the use of immersion oil in light microscopy3 and this principle was transferred to skin surface microscopy by the German dermatologist, Unna in 1893.4 The term “Dermatoscopy” was coined by the German dermatologist Johann Saphier in 1920.5 Goldman in 1950s published a series of interesting articles on new devices which he called “Dermoscopy” and was the first dermatologist to use this technique for evaluation of pigmented skin lesions.6–9 Rona MacKie, in 1971 identified for the first time, the advantage of surface microscopy for improvement of preoperative diagnosis of pigmented skin lesions and for the differential diagnosis of benign versus malignant lesions.10
Nowadays the dermatoscopes commercially available are the ones without capturing facility (DELTA 10©, MINI2000 Dermatoscope©), or with image capturing facility (Dermatoscope©, Videoepiscope©, DermLite Foto©, DELTA 20©). Most recently digital cameras have been designed that are attached to computers which allow easy storage, retrieval and follow-up. Few instruments have in built analytical abilty (DermoGenius Mole Map©). Latest development is introduction of dermatoscopes that use a smartphone for easy visualization and storage of images (e.g. Canfield Dermscope®).
Principle
Light is either reflected, dispersed, or absorbed by the stratum corneum because of its refraction index and its optical density, which is different from air.11 Therefore, deeper underlying structures cannot be adequately visualized. However, when various immersion liquids are used, they make the skin surface translucent thereby reducing the reflection so that the underlying structures become readily visible. The application of a contact plate flattens the skin surface and provides an even surface. Optical magnification is used for examination. Taken together, these optical means allow the visualization of certain epidermal, dermo-epidermal, and dermal structures.
Uses
Dermatoscopy increases the diagnostic accuracy compared to visual inspection. It helps in quick and effective examination of various anatomic structures of nail such as nail plate, hyponychium, free edge of nail plate, proximal nail fold, nail bed and matrix. It is useful to evaluate the different conditions causing nail pigmentation, helps differentiate benign from malignant lesions, helps in diagnosis of psoriasis, oncychomycosis and certain nail tumors. It is widely used for nail fold capillaroscopy to help in diagnosis and evaluation of systemic sclerosis and dermatomyositis (Figures 4.1A and B).
Dermatoscopic Semiology
Semiology is the study of signs and symbols. Dermatoscopy of nail shows some typical patterns which are frequently associated with a particular lesion.
- Blood spot—appears as blue-purple (recent) or brown-black (older lesion). In absence of other symptoms, they indicate subungual hemorrhages. Their presence does not rule out melanoma.38Figures 4.1A and B: (A) Normal nailfold capillaries at 20 X magnification; (B) Normal nailfold capillaries at 100 X magnification (Courtesy: Wg Cdr V Vasdev, Command Airforce Hospital, Bengaluru)They may also be seen in amelanotic melanoma and few squamous cell carcinoma.
- Brown longitudinal parallel lines with regular pattern, regular coloration, spacing and thickness indicate melanocyte hyperplasia seen in nail matrix nevi.
- Brown to black longitudinal lines with irregular thickness, spacing, coloration and disruption of parallelism goes in favor of melanoma.
- Homogenous gray lines indicate epithelial hyperpigmentation without melanocytic hyperplasia seen in ungual lentigo, ethnic pigmentation, drug and radiation induced pigmentation, trauma induced pigmentation, Laugier-Hunziker syndrome.
- Micro-Hutchinson's sign observed as pigmentation of proximal nail fold is diagnostic of melanoma.
- Linear micro-hemorrhages are mainly seen in onychomatricoma, achromic malignant melanoma, squamous cell carcinoma. They may be observed in few cases of hemangiomas and glomus cell tumors.
- Longitudinal erythronychia is usually seen in onychomatricoma, hemangioma and glomus cell tumor.
- Longitudinal leuco or xanthonychia are seen in nail tumors like squamous cell carcinoma, onychomatricoma, hemangioma, glomus cell tumor.
- Subungual distal hyperkeratosis is commonly seen in onychomatricoma and squamous cell carcinoma.
- Triangular distal onycholysis is quiet often found in glomus cell tumor, onychomatricoma, squamous cell carcinoma and hemangioma.
- Red spots are seen in amelanotic melanoma, yellow spots are observed in subungual exostosis and squamous cell carcinoma whereas purple-blue spots are found in blue nevus, glomus cell tumor and amelanotic melanoma.
- Longitudinal superimposition above the lunula is indicative of hemangioma, onychomatricoma and glomus cell tumor.

Dermatoscopic Examination of Nail Pigmentation
The differential diagnosis of nail pigmentation is vast and often difficult on clinical examination. Besides many patients are reluctant for biopsies of nail matrix as the procedure is painful and may result in permanent nail dystrophy and physicians may sometimes lack confidence of 39performing nail biopsies or the required specimen may be inadequate for histopathology. Hence the use of noninvasive techniques such as dermatoscopy can aid in evaluation and diagnosis of nail pigmentation, which in turn, will reduce the need for unnecessary surgeries. It can also help in choosing the appropriate technique and site of biopsy.
Nail pigmentation can be broadly classified as melanocytic and nonmelanocytic.12 In nonmelanocytic lesions such as fungal infections or subungual hematoma the pigment tends to be distributed homogenously. In melanocytic lesions, melanin is found in cellular inclusions,13 which under dermatoscopy appear as small granules measuring less than 0.1 mm in diameter.
Nail Pigmentation of Nonmelanocytic Origin (Nail Hyperchromia)
Exogenous Pigmentation
These include multiple causes. The most common causes are contact with chemical agents, topical application of therapeutic agents such as silver nitrate, anthralin, tobacco and cosmetics such as henna and hair dyes.14–16
Subungual Hematoma
Dermatoscopically, blood spots shows homogenous blue-purple (recent) or brown-black pigmentation (older lesions). Reddish to reddish black globules are seen along the proximal and lateral margins of the pigment. The proximal margin is usually well defined and rounded. The distal part shows streaks of pigment. The hematoma will progressively grow out distally as the nail grows. On rare occasions it may be caused by neovascularization within a tumor and hence its presence does not rule out diagnosis of melanoma. Hence any subungual hematoma that does not grow out or that which recurs at the same site requires special attention and further examination with radiography to rule out exocytosis or biopsy to rule out malignancy.
Fungal or Bacterial Infection
Nails infected with Trichophyton rubrum or with dematiaceous fungi such as Scytalidium dimidiatum are pigmented. They show homogenous brown to black pigmented band that is devoid of visible melanin inclusions and longitudinal streaks.
Nail Pigmentation of Melanocytic Origin
The most frequent causes of longitudinal melanonychia are shown in Table 4.1.
Nail Pigmentation Caused by Epithelial Hyperpigmentation
It is also known as melanocytic macule of the nail.17 Dermatoscopy shows presence of gray homogenous lines. There are multiple causes of epithelial hyperpigmentation and their corresponding dermatoscopic findings are listed below.
Longitudinal melanonychia as a result of focal melanocytic activation is induced by drugs and radiation.
Clinically it appears as horizontal or longitudinal bands or as diffuse nail darkening. It may affect one or more nails of the hands and feet. It may be associated with hyperpigmentation 40of the skin. It usually starts within 1–2 months of starting the offending drug and progressively fades once the agent is stopped.
|

Figures 4.2A to G: Schematic representation of 7 dermatoscopic patterns observed in longitudinal melanonychia:35 (A) Blood spots; (B) Brown coloration of background; (C) Regular lines; (D) Irregular lines; (E) Grayish background + ghin grayish lines; (F) Micro-Hutchinson's sign; (G) Microscopic grooves
Endocrine longitudinal melanonychia is commonly seen in Addison's disease. It may also be seen in Cushing's syndrome after adrenalectomy,18,19 hyperthyroidism,20 acromegaly, and during pregnancy.21 The clinical and dermoscopy findings are very similar to drug- and radiation-induced longitudinal melanonychia. It may involve multiple digits. In Addison's disease, longitudinal melanonychia is typically associated with cutaneous and mucosal hyperpigmentation.
Longitudinal melanonychia associated with HIV infection unrelated to AZT treatment has been described.22–24 The nail pigmentation usually affects multiple nails and is associated with pigmented macules of the palms, soles, and mucous membranes.
Longitudinal melanonychia associated with inflammatory nail disorders occasionally develops in nails affected by lichen planus,25,26 onychomycosis,27 chronic radiodermatitis, pustular psoriasis, or Hallopeau's disease. It is usually associated with nail scarring and abnormalities of the surface of the nail plate. The clinical and dermoscopy aspect of this entity is not specific.
Laugier-Hunziker Syndrome is an acquired disorder of pigment system characterized by longitudinal melanonychia28 and macular pigmentation of lips, mouth and anogenital area. It is characterized by presence of single or double band with a diameter of 1–2 mm or as homogenous pigmentation of lateral nail plate. It may also show pseudo-Hutchinson's sign.
Longitudinal melanonychia associated with nonmelanocytic nail tumours is seen rarely when the melanocytes are activated by the tumors. This is commonly seen with Bowen's disease.29,30 Biopsy is mandatory in such cases.
Nutritional longitudinal melanonychia can be seen with vitamin B12 and folic acid deficiency. It appears as a bluish black pigmentation. It is associated with hyperpigmentation over the knuckles and distal phalanges.
Traumatic longitudinal melanonychia is predominantly seen after repeated minor trauma such as nail biting, picking, chewing, breaking or rubbing of proximal nail fold which leads to repetitive nail matrx injuries.
Ethnic nail pigmentation is a physiological pigmentation of nails seen in individuals with skin type V and VI.31, 32 They present as single or multiple bands involving one or more digits (Figure 4.3).
Nail Pigmentation Caused by Melanocytic Proliferation
Clinically, it appears as a single dark pigmented band. On dermatoscopy the brown background pigmented band is composed of multiple thin lines. Depending on dermatoscopic pattern following diagnosis should be considered.
Regular Dermatoscopy Pattern
It is seen in nevi of nail matrix which may be congenital or acquired (Figure 4.4). It may appear in children and young adults. It may appear as light to dark brown or black, longitudinal, parallel, homogenously pigmented bands. It may clinically simulate a melanoma and may also be associated with pseudo-Hutchinson's sign in which one can see the nail matrix pigment 42through a translucent lunula.


Dermatoscopically, nevi of nail matrix show brown longitudinal parallel lines with regular spacing and thickness. This has been described as “regular pattern”.35,13
Irregular Dermatoscopy Pattern
It is seen in nail matrix melanoma. It affects middle aged to elderly individuals. It clinically presents as a broad band, dark brown to black color with fuzzy or blurred lateral borders. In 43the rapidly growing melanomas the lines within the band are not parallel and the diameter of the band is wider at the proximal end. In advanced stages dystrophy or even loss of nail plate may be seen. Pigmentation of the nailfold cuticle and the surrounding skin is knows as Hutchinson's sign. Dermatoscopicaly, nail matrix melanoma shows brown background coloration of the band. The individual lines forming the band show different degress of pigmentation, varying thickness and spacing. Some lines may end abruptly while some show loss of parallelism. This has been described as “irregular pattern.” Blood spots can also be seen due to neovascularization of the tumor. Any lesion with irregular dermatoscopy pattern should be biopsied.
Nail plate abnormalities such as pitting, nail crumbling, onycholysis, salmon patches, splinter hemorrhages and nail bed hyperkeratosis commonly seen in psoriasis are better defined with the use of a dermatoscope.36 The findings of dermatoscopy of nail plate in psoriasis is described in Table 4.2.
The hyponychium displays dilated tortuous, elongated and irregularly distributed capillaries on dermatoscopy which can be used to assess severity of the disease.37 In 2008, Iorizzo et al. showed that capillary density is positively correlated with the severity of the condition. This study also showed that quantitative analysis of the capillaries correlates with response to treatment. Few studies have showed that dermatoscopy of the hyponychium is the best diagnostic tool for confirming a diagnosis of psoriasis in patients with onycholysis alone or mild hyperkeratosis of the nail bed.38 Dermoscopy of the proximal nail fold is also useful for evaluating the severity of the disease, this site being appropriate for identifying quantitative and morphological abnormalities of the capillaries. The number and diameter of the capillaries are found to be significantly reduced in cases of psoriasis.39–41 In 1982, Zaric et al reported a reduction in the size of the capillaries of the proximal nail fold in patients with skin psoriasis and psoriatic arthritis compared to a control group. In 2000, Bhusham et al found a reduction in capillary density in the proximal nail fold of patients with nail psoriasis or psoriasis with nail and joint involvement compared to a control group. Only in patients with psoriatic arthritis, irrespective of whether or not this was associated with nail involvement, was a reduction also found in the diameter of these capillaries. In conclusion dermatoscopy is a noninvasive, quickly applied and inexpensive test that may aid diagnosis of nail psoriasis in inconclusive cases and improve the follow-up of the patient with respect to his/her response to treatment.
|
Dermatoscopy in Connective Tissue Disorders
Dermatoscopic examination of nails in systemic sclerosis and dermatomyositis show presence of dilated capillaries, avascular areas, disruption of the normal capillary bed architecture and areas of hemorrhage (Figures 4.5A and B). The negative predictive value of capillary changes for the diagnosis of systemic sclerosis and dermatomyositis is much higher than the positive predictive value, since similar but less dramatic nailfold capillary changes have been observed in SLE and more recently in other clinical settings (e.g. Henoch-Schönlein purpura,42 ankylosing spondylitis,43 familial mediterranean fever.44 In addition to assisting in the diagnosis of autoimmune connective tissue diseases, morphological and quantitative changes in nailfold capillaries have been suggested to parallel systemic disease activity/severity and signal response to treatment.45 Changes observed in nailfold capillaries in patients with dermatomyositis are very similar to those that are encountered in systemic sclerosis. Such nail fold capillary changes are less frequent in SLE (Figures 4.6A to C). It is presumed that the nailfold capillary changes seen in patients with classic dermatomyositis and clinically amyopathic dermatomyositis are virtually identical.

Figures 4.5A and B: Dermatomyositis: (A) Dilated capillaries, avascular areas and hemorrhage along with ragged cuticle; (B) Bushy capillaries(Courtesy: Figure B Wg Cdr V Vasdev, Command Airforce Hospital, Bengaluru)

Figures 4.6A to C: SLE: (A) Nonspecific nailfold capillary changes in SLE; (B) Nonspecific dilatation and branching in a case of SLE; (C) Nailfold hemorrhages in APLA syndrome(Courtesy: Wg Cdr V Vasdev, Command Airforce Hospital, Bengaluru)

Figures 4.7A to D: Systemic sclerosis: (A) Mega-capillaries in early systemic sclerosis; (B) Gross distortion of capillary architecture in advanced systemic sclerosis; (C) Giant capillaries in a case of systemic sclerosis; (D) Sclerodactyly: Avascular areas, dilated capillaries and hemorrhages(Courtesy: Figures A to C Wg Cdr V Vasdev, Command Airforce Hospital, Bengaluru
Therefore, detection of nailfold capillary changes can be of special value in early, clinically indeterminate inflammatory skin changes of dermatomyositis in a patient shortly before the development of muscle weakness (i.e. premyopathic dermatomyositis) or a patient destined never to develop muscle weakness or develop muscle weakness after prolonged periods of time (i.e., clinically amyopathic dermatomyositis).46,47 Another setting where recognition of nailfold capillary changes can be of clinical value is when evaluating a patient presenting during the early, incompletely expressed phase of an autoimmune connective tissue disease. An example would include the appearance of isolated Raynaud's phenomenon in a patient destined to later develop systemic sclerosis (Figures 4.7A to D).
Dermatoscopy of Nail Tumors
Nail tumors are rare and difficult to diagnose with the naked eye. Dermatoscopy serves as important tool in such cases for early diagnosis as well as intraoperatively to confirm complete excision of the tumor.
Amelanotic melanoma on dermatoscopy shows disappearance of lunula with polychromia in majority of cases. Longitudinal fractures, blood spots, irregular linear telangiectasias and disappearance of nail plate is seen in majority cases. Few cases are associated with liner micro-hemorrhages, purple-blue and red spots.
Dermatoscopic examination of squamous cell carcinoma shows presence of subungual distal hyperkeratosis, longitudinal leuco-xanthonychia and polychromia. Triangular distal onycholysis, convex deformity of nail plate, yellow spot with linear microhemorrhages may be associated. Some cases may show triangular lunula or total disappearance of lunula.46
Onychomatricoma is associated with subungual distal hyperkeratosis, linear microhemorrhages, convex deformity of nail plate, longitudinal superimposition above the lunula and longitudinal leuco-xanthonychia. Triangular distal onycholysis, longitudinal erythronychia and irregular linear telangiectasias may be seen in few cases.
Pain during dermatoscopic examination is a feature of subungual glomus cell tumor. Findings on dermatoscopy include purple-blue spot, convex deformity of nail plate, triangular distal onycholysis, parallel longitudinal regular red lines with disappearance of the lunula. Few cases may show longitudinal erythronychia or leuco-xanthonychia.
Subungual hemangioma shows longitudinal erythronychia with longitudinal superimposition above the lunula on dermatoscopy. In some cases linear microhemorrhages and longitudinal leuco-xanthonychia may be present.
The main dermatoscopic feature of blue nevus of the nail (rare entity) is an isolated purple- blue spot, whereas, subungual exostosis appears as an isolated well-circumscribed yellow spot.
This list of uses and indications in not all-inclusive and still expanding. In summary nail dermatoscopy is one more advancement in diagnostic tools in the hands of dermatologists. In addition to its help in diagnosing disorders, it has a role in prognostic assessment as well as in judging result of therapeutic intervention.
References
- Stolz W, Braun-Falco O, Bilek P, Landthaler M, Burgdorf WHC, Cognetta AB. Color atlas of drmatoscopy. 2nd edition. Berlin: Blackwell Wissenschafts-Verlag; 2002.
- Gilje O, O'Leary PA, Baldes EY. Capillary microscopic examination in skin siease. Arch Dermatol. 1958;68:136–45.
- Diepgen P. Geschichte der Medizin. Berlin: De Gruyter; 1965.
- Unna P. Die Diaskopie der Hautkrankheiten. Berl Klin Wochen. 1885;42:1016–21.
- Saphier J. Die Dermatoskopie. I. Mitteilung. Arch Dermatol Syphiol. 1920;128:1–19.
- Goldman L. Some investigative studies of pigmented nevi with cutaneous microscopy. J Invest Dermatol. 1951;16:407–26.
- Goldman L. Clinical studies in microscopy of the skin at moderate magnification. Arch Dermatol. 1957;75:345–60.
- Goldman L. A simple portable skin microscope for surface microscopy. Arch Dermatol. 1958;78:246–7.
- Goldman L. Direct skin microscopy as an aid in the early diagnosis of precancer and cancer of the skin in the elderly. J Am Geriatr Soc. 1980;28:337–40.
- MacKie RM. An aid to the preoperative assessment of pigmented lesions of the skin. Br J Dermatol. 1971;85:232–8.
- Anderson RR, Parrish JA. The optics of human skin. J Invest Dermatol. 1981;77:13–9.
- Haneke E, Baran R. Longitudinal melanonychia. Dermatol Surg. 2001;27:580–4.
- Marghoob AA, Braun RP, Kopf AW. Atlas of dermoscopy. New York: Taylor Francis; 2005.
- Baran R, Dawber RPR, De Berker DAR, Haneke E, Tosti A. Diseases of the nail and their management. 3rd edition. Oxford: Blackwell Science; 2001.
- Jeanmougin M, Civatte J. Nail dyschromia. Int J Dermatol. 1983;22:279–90.
- Platschek H, Lubach D. Braune Haar und Nagel Verfärbungen. Hautarzt. 1989;40:441–2.
- Bissel GW, Surakomol K, Greenslet F. Longitudinal banded pigmentation of nails in primary adrenal insufficiency. JAMA. 1971;215:1666–7.
- Bondy PK, Harwick HJ. Longitudinal banded pigmentation of the nails following adrenalectomy for Cushing's syndrome. N Engl J Med. 1969;281:1056–7.
- Daniel CR III. Nail pigmentation abnormalities. Dermatol Clin. 1985;3:431–43.
- Baran R, Perrin C, Braun RP, Thomas L. The melanocyte system of the nails and its disorders. In: Nordlund JJ, Boissy RE, Hearing R, King R, Ortonne JP (Eds). The pigmentary system. 2nd edition. New York: Oxford University Press; 2005.
- Cribier B, Mena ML, Rey D, Partisani M, Fabien V, Lang JM, et al. Nail changes in patients infected with human immunodeficiency virus: a prospective controlled study. Arch Dermatol. 1998;134:1216–20.
- Glaser DA, Remlinger K. Blue nails and acquired immunodeficiency syndrome: not always associated with azidothymidine use. Cutis. 1996;57:243–4.
- Panwalker AP. Nail pigmentation in the acquired immunodeficiency syndrome (AIDS). Ann Intern Med. 1987;107:943–4.
- Hirsch RJ, Weinberg JM. Evaluation of pigmented lesions of the nail unit. Cutis. 2001;67:409–11.
- Juhlin L, Baran R. Longitudinal melanonychia after healing of lichen planus. Acta Derm Venereol. 1989;69:338–9.
- Tosti A, Argenziano G. Dermoscopy allows better management of nail pigmentation. Arch Dermatol. 2002;138:1369–70.
- Baran R. Longitudinal melanotic streaks as a clue to Laugier-Hunziker syndrome. Arch Dermatol. 1979;115:1448–9.
- Lambiase MC, Gardner TL, Altman CE, Albertini JG. Bowen disease of the nail bed presenting as longitudinal melanonychia: detection of human papillomavirus type 56 DNA. Cutis. 2003;72:305–9.
- Defiebre BK Jr. Bowen's disease of the nail bed: a case presentation and review of the literature. J Hand Surg [Am]. 1978;3:184–6.
- Leyden JJ, Spott DA, Goldschmidt H. Diffuse and banded melanin pigmentation in nails. Arch Dermatol. 1972;105: 548–50.
- Monash S. Normal pigmentation in the nails of the Negro. Arch Dermatol. 1932;12:876–81.
- Skowron F, Combemale P, Faisant M, Baran R, Kanitakis J, Dupin M. Functional melanonychia due to involvement of the nail matrix in systemic lupus erythematosus. J Am Acad Dermatol. 2002;47(Suppl):S187–8.
- Baran R. Longitudinal melanonychia in localized scleroderma. J Am Acad Dermatol. 2004;50:E5.
- Ronger S, Touzet S, Ligeron C, Balme B, Viallard AM, Barrut D, et al. Dermoscopic examination of nail pigmentation. Arch Dermatol. 2002;138:1327–33.
- Tosti A, Piraccini BM, de Farias DC. Nail diseases. In: Micali G, Lacarrubba F (Eds). Dermatoscopy in clinical practice: beyond pigmented lesions. London: Informa Healthcare Ltd; 2010.
- Iorizzo M, Dahdah M, Vincenti C, Tosti A. Videodermoscopy of the hyponychium in nail bed psoriasis. J Am Acad Dermatol. 2008;58:714–5.
- Tosti A, Pirraccini BM, Farias DC. Nail dermoscopy. In: Micali G. Videodermatoscopy in Clinical Pratice. London: Informa Healthcare; 2009.
- Ohtsuka T, Yamakage A, Miyachi Y. Statistical definition of nailfold capillary pattern in patients with psoriasis. Int J Dermatol. 1994;33:779–82.
- Zaric D, Clemmensen OJ, Worm AM, Stahl D. Capillary microscopy of the nail fold in patients with psoriasis and psoriatic arthritis. Dermatologica. 1982;164:10–4.
- Martino F, Agolini D, Tsalikova E, et al. Nailfold capillaroscopy in Henoch-Schonlein purpura: a follow-up study of 31 cases. J Pediatr. 2002;141:145.
- Wendling D, Risold JC. Nailfold capillaroscopy and ankylosing spondylarthritis: incidence of anomalies, but absence of diagnostic and prognostic value. Rev Med Interne. 1994;15:448–51.
- Dinc A, Melikoglu M, Korkmaz C, Fresko I, Ozdogan H, Yazici H. Nailfold capillary abnormalities in patients with familial Mediterranean fever. Clin Exp Rheumatol. 2001;19 (Suppl 24):S42–4.
- Silver RM, Maricq HR. Childhood dermatomyositis: serial microvascular studies. Pediatrics 1989;83:278–83.
- Sontheimer RD. Dermatomyositis: An overview of issues of interest to dermatologists [review]. Dermatol Clin. 2002;20:387–408.
- Sontheimer RD. Would a new name hasten the acceptance of amyopathic dermatomyositis (dermatomyositis sine myositis) as a distinctive subset within the idiopathic inflammatory dermatomyopathies spectrum of clinical illness? J Am Acad Dermatol. 2002;46:626–36.
Consultation for the primary nail disorder is uncommon. Most of the time child presents with skin disease where nail changes may be part of it. Occasionally child presents with isolated nail problem. Nail disorders in children can be classified as1
- Physiologic alterations – Needs no treatment
- Congenital and Inherited Conditions
- Infections – Onychomycosis, Paronychia, Wart
- Dermatological Disease – Eczema, Psoriasis, Lichen planus, Trachyonychia
- Systemic or Iatrogenic nail changes
- Trauma – Acute and Chronic
Nail changes may be present at birth and/or are signs of hereditary or congenital disorder. Presence of nail changes may be a clue of a syndrome or a systemic disease. Iglesias et al reported rate of nail changes in 11% of pediatric dermatology patients.2
Physiological Alteration
Infants can have transverse depression of the fingernails between 8 and 9 weeks.3 The other transient changes can be: a small degree of onycholysis, deviation from the midline and distal thickening. Most of these changes disappear by 14–16 weeks.
Young children upto the age of 5–6 years can have mild koilonychias or malalignment or thickening of toe nails. Nail biting may be seen in 30% of children. Most of the time it is transient. Biting habit may lead to paronychia, ingrowth of nail, transmission of infection like wart.
Congenital and Inherited Conditions
Inamdar and Palit have reviewed this subject in great detail.4
There are certain nail changes specific in genodermatoses like Pachyonychia Congenita, Nail Patella syndrome. At times nail changes may be one of the manifestation like in Congenital mucocutaneous candidiasis.50
|
Dermatological Diseases
The common nail diseases in children are the same as in adults: eczema, psoriasis, lichen planus and alopecia areata. Twenty nail dystrophy is common in children. Most of them start as pitting on nail plate.
Twenty nail dystrophy is poorly defined term.5 It can represent one of the above mentioned diseases. Trachonychia is identified as rough nail surface with longitudinal striations. This may later on lead to longitudinal splitting. It may affect few nails at a time. Histology is suggestive of spongiosis topical or intralesional steroids and at times oral steroids are used to treat Twenty nail dystrophy. It is important to treat aggressively if LP is the aetiological diagnosis to prevent scarring.
0.6% to 2.3% of psoriasis patient only show nail changes.
Onychomycosis is uncommon in children. Most of the time it is superficial white onychomycosis. Periungual tumours are most commonly warts. It may affect nail matrix and damage nail plate.
Leuconychia is patchy pattern of partial, transverse white streaks. Parents tends to believe it as lack of calcium. Most of the time it is due to mild trauma. It can be also seen in thyroid disorder and autoimmunity.
References
- Richert B and Andre J. Nail disorders in children. Am J Clin Dermatol. 2011; 12: 101–112.
- Iglesias A, Tamayo L et al. Prevalence and nature of nail alterations in pediatric patients. Peddiatr Dermatol. 2001:18;107–109.
- Berker David de. Childhood Nail Diseases. Dermatol Clinics. 2006;24: 355–363.
- Inamdar A and Palit A. Nails: Diagnostic clue to genodermatoses. Indian J Dermatol Venereol and Leprol. 2012;78:271–8.
- Tosti A, Bardazzi F et al. Idopathic trachyonychia (tweny-nail dystrophy); a pathological study of 23 patients. Br J Dermatol. 1994; 131: 866–872.
The congenital and hereditary nail diseases include a number of conditions in which nail abnormalities are present at birth or develop during infancy. Nail changes may be the earliest signs by which a hereditary ectodermal syndrome can be recognized. Telfer et al classified congenital and hereditary nail disorders into nail matrix defects, nail fold defects, nail bed defects and combined ectodermal-mesodermal defects. Selected nail diseases are classified in Table 5b.1.1
|
Change in Nail Matrix Form and/or Size
Anonychia
|
|
Anonychia refers to absence of nails. Total or partial absence of nail at birth is rare. It may occur as an isolated inherited trait or may be associated with other developmental defects.3 Isolated anonychia may present either in an autosomal dominant form that affects only the thumbs or in a recessively inherited variant affecting all the digits and toes. The gene RSPO4 was identified as responsible for inherited anonychia. Mutations occur in the secreted Wnt-signalling component, R-Spondin 4 that is necessary for embryologic development and regulation of cell morphology, proliferation and motility.4 Anonychia is usually accompanied by rudimentary nails on other digits. Anonychia may be a consequence of fetal exposure to systemic medications in early pregnancy or a sign of a genetic syndrome (Table 5b.2). Hypoplasia of the nails can occur in children whose mothers have been exposed to anticonvulsants, alcohol or warfarin.
Acquired anonychia can occur as a result of severe inflammatory involvement of nail unit (Table 5b.3).
Micronychia and Macronychia
Nail hypoplasia is a congenital deformity that can be sporadic, inherited or associated with syndromes. Nail that appears smaller is called micronychia and larger is called macronychia. 54
|
It can be unilateral or bilateral and can involve one or more digits. The causes of micronychia are listed in Table 5b.4.
Macronychia is associated with Von Recklinghausen's disease, epidermal nevus syndrome, Proteus syndrome, Klippel-Trenaunay-Weber syndrome and Maffuccis syndrome.5
Polyonychia
The presence of two or more separate nails on one digit is termed polyonychia. It may be inherited as an isolated autosomal dominant trait or associated with trisomy 13 or Lawerence-Moon-Biedl syndrome.
Nail-patella syndrome (Syn: HOOD syndrome - Hereditary Osteo-Onychodysplasia, Fong's syndrome)
Nail patella syndrome is an autosomal dominant inherited condition described by Chatelain in 1820 and Little in 1897. The incidence is 1 in 50,000 and occurs in all ethnic groups throughout the world. It has been associated with mutations in the LMX1B gene that encodes a transcription factor that regulates collagen synthesis.6 It is characterized by nail dystrophy, hypoplastic or aplastic patella, elbow dysplasia, webbing of the digits, exostosis of iliac crest and nephropathy.
Nail abnormalities occur in 98% of cases and are present from birth. Nail changes are persistent throughout life. The finger nails may be absent or hypoplastic, fragile, split and longitudinally ridged. The nail abnormalities are most severe on the ulnar side of the thumb, decreasing to the index and little finger. Toe nails are rarely affected. Anonychia or micronychia and triangular lunula with distal apex in the midline are highly predictive of nail patella syndrome.7 Absence of skin creases on the dorsal aspects of distal interphalangeal joint is a more specific sign of this disorder.
Associated features are hypoplasia or aplasia of the patella resulting in subluxation, hypoplasia of proximal radius and ulna (limitation of elbow movement), iliac horns and exostosis of iliac crests present in 70% of patients are pathognomonic features. In children the diagnosis is best confirmed by the presence of iliac horns on pelvic X-ray. Nephropathy develops in approximately 40% of cases. This leads to renal insufficiency.
DOOR Syndrome (Deafness-Onycho-Osteodystrophy-Mental Retardation)
The hallmarks of this syndrome are sensorineural hearing loss, hypoplastic or absent nails on the hands and feet, small or absent distal phalanges of the hands and feet, and mental retardation (Figures 5b.1 and 5b.2). Onychodystrophy is present since birth.
DOOR syndrome is associated with characteristic, coarse facial features with large nose with wide nasal bridge, bulbous tip and anteverted nares, a long prominent philtrum and downturned corners of the mouth. The natural history is one of a deteriorative course, with progressive neurological manifestations including sensorineural deafness, seizures from infancy, optic atrophy, and a peripheral polyneuropathy.


The majority of patients with DOOR syndrome have elevated levels of 2-oxoglutarate in the urine and plasma.8
Focal Dermal Hypoplasia (Goltz-Gorlin Syndrome)
Focal dermal hypoplasia is a rare developmental disorder primarily involving the skin, skeletal system, eyes and face. The characteristic skin lesions are streaky areas of linear hypoplastic appearing skin, with telangiectasia, hyperpigmentation and hypopigmentation. Skin involvement with skeletal abnormalities supports the clinical diagnosis of focal dermal hypoplasia.
Skeletal abnormalities include syndactyly, ectrodactyly and hypoplasia or aplasia of digits. Nails are thin and spoon shaped. Dystrophy, anonychia (50% case) and grooving of both fingernails and toenails is frequently present. There may be no lunulae (Figure 5b.3).9
Trichorhinophalangeal Syndrome
Trichorhinophalangeal syndrome first described by Giedion in 1966 is characterized by triad of fine, sparse, slowly growing scalp hair, a pear shaped bulbous nose, and brachyphalangia with radiologically demonstrable cone shaped epiphyses of hands and feet. Nail may be dystrophic, hypoplastic, brittle, slow growing, koilonychotic or leukonychotic.10 57

Figure 5b.3: Focal dermal hypoplasia: Ectrodactly of right feet with syndactly of left feet with grooved and hypoplastic nails
Ectodermal Dysplasia
Nails are affected in 50% of the patients in hypohidrotic or anhidrotic ectodermal dysplasia. Anonychia, brittle, thin or shrivelled, ridged or discolored nails may be present. Dystrophy of nails is an important component of hidrotic ectodermal dysplasia (Figure 5b.4). Nails are thickened, striated and discolored. Hypoplastic nails are seen in various types of ectodermal dysplasia (Table 5b.5).11

|
Racquet Nails (Brachyonychia)
Racquet nail is an autosomal dominant developmental anomaly. It may affect any finger but the thumbs are more commonly involved. Girls are more frequently affected than boys. It usually occurs as an isolated phenomenon or associated with other abnormalities. The distal phalanx is shortened and wide. In affected individuals, the epiphyses of the terminal phalanx of the thumbs close prematurely, at the age of 7-10 years. Disorders associated with brachyonychia include cartilage-hair hypoplasia, acro-osteolysis, Larsen's syndrome, Rubinstein-Taybi syndrome, pyknodysostosis, acrodystosis and multiple malignant cylindromas.
Rubinstein-Taybi Syndrome
Rubinstein-Taybi syndrome (RSTS) was originally described by Rubinstein and Taybi in 1963. The major diagnostic criteria are broad short terminal phalanges of the thumbs and halluces, a 59characteristic facial appearance with beaked or straight nose, antimongoloid slant of palpebral fissures, hypertelorism, grimacing smile and mental retardation.
On the hands and feet broad and radially deviated thumbs, broad terminal phalanges of other fingers, broad halluses with or without varus/valgus angulation with broad and sometimes duplicated nails, polydactyly, syndactyly, clinodactyly have been found in RSTS.10
Change in Nail Matrix Position
Ectopic Nails (Onychoheterotopia)
Onychoheterotopia is misplaced nails. It is an extremely rare condition that can be congenital or acquired. Ectopic nails have been described on the palmar surfaces of the fingers and on the heel. They are associated in some cases with acquired or congenital growth anomalies or with polydactyly.13
Congenital Malalignment of the Great Toenail
Congenital malalignment of the great toenails was first described by Samman in 1978. It is a common disorder but no prevalence data are available. The disorder is transmitted as autosomal dominant with variable expression. It is possibly caused by an abnormality in the ligament that connects the matrix to the periosteum of the distal phalanx. The nail plate of the hallux is laterally deviated with respect to the longitudinal axis of the distal phalanx. This results in nail matrix damage with Beau's lines and onychomadesis. Embedding of the malaligned nail plate into the lateral nail folds may give rise to ingrowing toe nails. The condition often improves spontaneously. However, if the nail deviation is marked, surgical rotation of the misdirected matrix is indicated.13
Congenital Onychodysplasia of the Index Fingers (COIF Syndrome/ Iso-Kikuchi Syndrome)
It is a rare distinctive nail disorder that has been mostly reported from Japan. Most cases are sporadic but autosomal dominant cases have been reported. COIF may be unilateral or bilateral. The nails of the index finger are short, absent or small. It may present with anonychia or asymmetric ulnar micronychia with or without polyonychia. The nail plates are thin, have a rolled appearance or have partial onychogryphosis and malalignment. Radiographs of the underlying phalanx disclose a characteristic Y-type bifurcation or a sharpened tip of the distal phalanx.14
Changes in Nail Matrix Function
Onychogryphosis may be seen in patients with ectodermal dysplasia, Thost-Unna type of palmoplantar keratoderma, CHILD syndrome and fucosidosis. Clubbing of the fingers can be seen in syndromes like acro-osteolysis, cartilage-hair hypoplasia, keratoderma palmoplatare, Nakajo syndrome, Oto-onycho-peroneal syndrome and Peutz-Jeghers syndrome.15 Isolated koilonychia may be inherited as an autosomal dominant trait or it may be associated with other syndromes.
Koilonychia may be seen in various ectodermal dysplasia, ichthyosis, palmoplantar keratoderma, focal dermal hypoplasia, incontinentia pigmenti, LEOPARD syndrome, monilethrix, nail-patella syndrome, Cronkhite-canada syndrome, Nezelof's syndrome, and Oliver-McFarlane syndrome.
Leukonychia are inherited as autosomal dominant traits or can sometimes be familial. Congenital leukonychia totalis is a rare developmental anomaly where the nail plate is milky or porcelain-white. In one study the genetic defect in hereditary leukonychia was linked to chromosome 12q13.16 Total or partial leukonychia has been found to be associated with palmoplantar keratoderma with deafness, congenital hypothyroidism and LEOPARD syndrome.
Dyskeratoses Congenita (Zinsser-Cole-Engman Syndrome)
The mucocutaneous features, skin pigmentation, nail changes, and leukoplakia usually appear first between the ages of 5 and 10 years. Nail changes are progressive and ranges from pitting, ridging, thinning, and pterygia formation to complete nail loss. There may be recurrent episodes of suppurative paronychia.15
Trichothiodystrophies
Nail changes seen in these disorders are onychauxis, subungual hyperkeratosis, onychoschizia, longitudinal grooving, koilonychia, unguis inflexus and yellowish discoloration of nails.1761
Changes in Nail Matrix and Nail Bed
Pachonychia Congenita (Figures 5b.5 and 5b.6)
Pachyonychia congenita (PC) is characterized by universal nail hypertrophy and dyskeratosis of the skin and mucous membranes. Thick, yellowish brown-colored nails present at birth or developed during neonatal period with or without natal teeth are pointers to the diagnosis of Pachyonychia congenita. Dystrophy of all nails is a feature common to all the three variants of PC. Upward angulation of the distal free edge of the thickened nail plate (progressive distal thickening) is a distinctive feature and helps differentiate it from other disorders with thick nails.18


Figure 5b.6: Thickened toenails in PC(Courtesy: Dr Ravi Hiremagalore, Department of Pediatric Dermatology, Manipal Hospital, Bengaluru)
Type 1 Pachyonychia congenita (Jadassohn-Lewandowsky syndrome) – Nails are normal at birth but becomes discolored, especially at proximal ends. These changes are more in finger nails than in toe nails. It is associated with painful palmoplantar keratoderma with oral leukokeratosis.
Type 2 Pachyonychia congenita – Nail thickening is more uniform. It is associated with natal teeth and multiple steatocystomas.
Type 3 Pachyonychia congenita – Nail thickening is less severe than type 1 and 2 PC. Nail dystrophy may appear late in childhood or adulthood.
Genodermatoses with Secondary Nail Changes
Nails may be the primary site of affection in some genodermatoses whereas in others it is merely part of the syndrome. Nail involvement in genodermatoses may be categorized into three groups (Table 5b.6).19
Epidermolysis Bullosa
Nail changes in epidermolysis bullosa (EB) results from abnormalities of the nail matrix and nail bed that follow the pathogenic alterations at the dermo-epidermal junction. Nail involvement has been included among the criteria for scoring EB severity as early nail dystrophy and loss are correlated with disease severity and progression particularly in junctional EB and recessive dystrophic EB (Figures 5b.7 and 5b.8). Nail changes are milder in EB simplex. Nail involvement is uncommon in localized EB simplex (EBS) and is not a feature of EBS migratory circinate or EBS with pyloric atresia. Nail involvement in different subtypes of EB is given in Table 5b.7.20
Acrodermatitis Enteropathica
Nail changes are secondary to paronychial inflammation and occurs in 96% of children. Longitudnal ridges, multiple Beau's lines and dystrophy are common.
Tuberous Sclerosis
Subungual and Periungual fibromas (Koenen's tumor/Garlic-clove fibroma) are seen in approximately 50% patients with tuberous sclerosis complex (TSC). They are multiple, elongated, pink or flesh colored tumors with hyperkeratotic tips, arising from beneath the proximal and lateral nail folds (periungual) producing longitudinal midline depression on nail plate. Occasionally longitudinal midline groove on the nail plate may be the only finding in these patients and may result from cryptic subungual fibroma, impacting the nail matrix.2163
|


| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Aldrich et al have reported occurrence of red comets in 25% of adult patients with TSC in their series and considered this as a characteristic finding. These are partially blanchable linear red streaks with bulging at the distal end and surrounding pallor. Red comets are located at the middle of the nail plate and extend upto distal one-third without involving the free margin. The lesions are persistent, nonprogressive and asymptomatic. These signify presence of telangiectasia with extravasated blood.21
Cuticular hyperkeratosis is sometimes seen and may present as subclinical Koenen's tumor. Macrodactly may be seen.
Incontinentia Pigmenti
Nail changes that occur are pitting, transverse and longitudinal ridging. Nails may be dystrophic. Diffuse yellowing and thickening of nail plates may develop. Onycholysis and a lytic deformity of the underlying terminal phalanges may occur.22 Tender subungual and periungual tumors have been observed in adolescent children.
Darier Disease (Follicular Dyskeratosis)
Nail changes occur in 92% of patients with Darier disease. ‘V’-shaped notch on the free edge of the nail plate along with alternate longitudinal red (erythronychia) and white (leukonychia) bands are the distinct features of Darier's disease. Splinter hemorrhages may be associated. Histologically, there is hyperplasia of the nail bed epithelium with multinucleated giant cells but not suprabasal clefts.
Nail changes in genodermatoses along with other associated features can aid to the diagnosis.
References
- Tefler NR, Barth JH, Dawber RPR. Congenital and Hereditary nail dystrophies - an embryological approach to classification. Clin Exp Dermatol 1988;13:160–3.
- Baran R, Dawber R. P.R. Diseases of the nails and their management. Blackwell Science, second ed. 1994.
- Hopsu-Havu VK, Jansen CT. Anonychia congenital. Arch Dermatol. 1973;107:752.
- Bergmann C, Senderek J, Anhuf D, et al. Mutations in the gene encoding the Wnt-signaling component R-spondin 4 (RSPO4) cause autosomal recessive anonychia. Am J Hum Genet. 2006;79:1105–9.
- Baran R, Dawber RPR. Physical signs. In: Baran R, Dawber RPR, editors. Diseases of the nails and their management. 2nd ed. Oxford: Blackwell Scientific Publications; 1994.p.35-90.
- Bongers EM, Gubler MC, Knoers NV. Nail-patella syndrome. Overview on clinical and molecular findings. Pediatr Nephrol. 2002;17:703–12.
- Kamath S, Bhagwandas K. Nail-Patella syndrome with an emphasis on the risk of renal and ocular findings. Pediatr Dermatol 2010;27:95–114.
- James AW, Miranda SG, Culver K, Hall BD, Golabi M. DOOR syndrome: clinical report, literature review and discussion of natural history. Am J Med Genet 2007;143:2821–31.
- Temple IK, MacDowall P, Baraitser M, Atherton DJ. Focal dermal hypoplasia (Goltz syndrome). J Med Genet 1990;27:180–7.
- Fistarol SK, Itin PH. Nail changes in genodermatoses. Eur J Dermatol. 2002;12:119–28.
- Irvine AD, Mellerio JE. Genetics and genodermatoses. In: Burns T, Breathnach S, Cox N, Griffiths C, editors, Rooks Textbook of Dermatology. 8th ed. Oxford: Wiley-Blackwell; 2010.p.15.1-15.97.
- Kopera D, Soyer P, Kerl H. Ectodermal calcaneal nail. J Am Acad Dermatol. 1996;35:484–5.
- Baran R. Significance and management of congenital malignment of the big toe nail. Cutis. 1996;58:181–4.
- Miura T, Nakamura R. Congenital onychodysplasia of the index fingers. J Hand Surg. 1990;15:793–797.
- Norgett EE, Wolf F, Balme B, et al. Hereditary ‘White nails’ a genetic and structural study. Br J Dermatol. 2004;151:65–72.
- Itin PH, Pittelkow MR. Trichothiodystrophy: Review of sulphur-deficient brittle hair syndromes and association with the ectodermal dysplasia. J Am Acad Dermatol. 1990;22:705–17.
- Tosti A, Lorizzo M, Piraccini BM, Starace M. The nail in systemic diseases. Dermatol Clin 2006;24:341–7.
- Inamdar AC, Palit A. Nails: Diagnostic clue to genodermatoses. Indian J Dermatol Venereol Leprol 2012;78:271–8.
- Tosti A, Farias DC, Murrell DF. Nail involvement in Epidermolysis bullosa. Dermatol Clin 2010;28:153–7.
- Aldrich SL, Hong CH, Groves L, Olsen C, Moss J, Darling TN. Acral lesions in tuberous sclerosis complex: Insights into pathogenesis. J Am Acad Dermatol 2010;63:244–51.
- Landy SJ, Donnai D. Incontinentia pigmenti (Bloch-Sulzberger syndrome). J Med Genet. 1993;30:53–9.
Nail disorders comprise approximately 10% of all dermatological conditions and affect a high percentage of the geriatric population.1,2 This is due in part to impaired circulation and particular susceptibility of the senile nail to faulty biomechanics, trauma, infections, neoplasms, concurrent dermatological or systemic diseases and their treatments.2 Various physiological as well as disease associated changes and disorders are seen in the aging nail. Many of these are extremely painful, affecting stability, ambulation and other functions like picking up of fine objects, tactile sensation, and protective function.2,3 The prevention and management of these conditions require periodic cutting of the nails and appropriate medical care. Unfortunately this is difficult for the elderly because of thickness of the nails, difficulty in accessing the feet, poor vision and sometimes, a lack of motivation for personal care.3 The aesthetic aspect of the nails is of significance even in the elderly, as it may affect interaction within the family and also with others in the society.70
Etiology
The senile changes are presumably due to impaired peripheral circulation.3 Frequently arteriosclerosis is the cause, though it may not be marked.3 The ability of an extremity to withstand trauma is severely limited when arterial insufficiency is present.3 Alterations in elastic tissue in the nail bed dermis and blood vessel walls in the subungual area have also been noted.3 Though nail plate is an efficient sunscreen, UV radiation may play a role in such changes.3 Trauma, faulty biomechanics, infections, concurrent dermatological or systemic diseases and their treatments are also contributory factors.2,4
Senile Changes in Nails
The following changes are observed in human nails as part of aging process:
i. Alteration in Chemical Composition
With aging, the calcium content of the nails increases whereas iron decreases.3
ii. Alteration in Histology
The nail plate keratinocytes enlarge. There is an increase in the number of “pertinax bodies”, which are retained keratinocyte nuclei appearing as acidophilic masses. The nail bed dermis shows thickening of the blood vessels and degeneration of the elastic tissue, especially beneath the pink part of the nail.5
iii. Alteration in Nail Growth
In the elderly, the rate of nail growth decreases progressively between 25 to 100 years of age, by approximately 0.5% per year.5 Factors which may be responsible for decreased growth rate in the elderly include actinic effects on the nail matrix, circulatory impairment, nutritional deficiency, hormonal changes, and local and systemic infections.3
iv. Alteration in Color
The senile nails may appear pale, dull, opaque, with the color ranging from yellow to brown or gray.5 Lunula may be decreased or absent altogether.6
“Neapolitan nail”, which can be seen in up to 20% of the persons older than 70 years, are characterized by three bands similar to the colors of the Neapolitan ice-cream, i.e. a proximal white portion with absent lunula, a central normal pink band and an opaque distal free edge.5
v. Alteration in Contour
The senile nails usually have an increased transverse curvature and a decreased longitudinal curvature.3,7 Flattening of the nail plate (platyonychia), spooning (koilonychia), pincer nail deformity (involution) are found more frequently.571
vi. Alteration in Surface Texture
Normally, the nails have a smooth surface. The senile nail may have increased longitudinal striations due to altered turnover rate of the matrix cells. The striations are termed “onychorrhexis” if they are superficial and “ridges” or “sausage-link ridges” or “beading” if deep.5 Aging is the commonest cause of onychorrhexis.10 Beau's lines (transverse ridges) and pits are also found frequently.9 The nails may be rough (trachyonychia) with splitting and fissuring.5
vii. Alteration in Thickness and Consistency
In the elderly, the nail plate thickness may increase, decrease or may remain unchanged. Fingernails tend to soften, whereas toenails seem to become tougher.3,5
Nail Disorders Among Elderly
Brittle Nails (Fragilitas Unguium)
Brittle nails are common in persons older than 60 years and about 20% of randomly selected population was affected in one study. Females were affected more in a ratio of 2:1.8 They manifest as excessive longitudinal ridges, roughness of the nail plate (trachyonychia), horizontal lamellar splitting of distal nail plate (onychoschizia or onychoschisis) (Figure 6.1). and irregularity of the distal edge of the nail plate (castle battlement appearance).
Onychodystrophies from Faulty Biomechanics and Trauma
Bony deformities of the digits or foot-to-shoe incompatibility (ill fitting shoes) can cause faulty biomechanics leading to onychodystrophies such as nail plate hypertrophy (onychauxis), onychogryphosis, onycholysis, ingrowing toe nails (onychocryptosis), onychophosis, subungual hyperkeratosis, subungual corn (onychoclavus) and subungual hematoma.5,9

Onychauxis/Pachyonychia
Onychauxis denotes localized hypertrophy of the nail plate and pachyonychia is diffuse hypertrophy of the nail plate. Onychauxis manifests as hyperkeratosis, discoloration, loss of translucency of the nail plate, and may be associated with subungual hyperkeratosis, resembling onychomycosis.5
Onychauxis may be associated with aging as well as several disorders more common in the geriatric population.4 This may be complicated with distal onycholysis, pain, increased susceptibility for onychomycosis, subungual hemorrhage and subungual ulceration.5
Onychogryphosis
This refers to an enlargement and thickening of the nail plate which appears “ram's horn-like” or “oyster-like”, mostly involving the great toenail (Figure 6.2). The nail plate appears uneven, thickened and brown to opaque, often with multiple transverse striations and hypertrophy of the underlying nail bed. This is mainly due to infrequent cutting of the nails. Other etiologies include trauma, hypertrophy of the nail bed and bony deformities like hallux valgus.4,5 The nail plate initially grows upwards and thereafter deviates laterally towards the other toes, the direction of growth being influenced by pressure from footwear and matrix activity. Few patients develop subungual gangrene due to pressure effects, especially in presence of diabetes mellitus or peripheral vascular disease.4
Onychophosis
This refers to localized or diffuse hyperkeratosis on the lateral or proximal nail folds, in the space between the nail folds and nail plate, and also subungually. It results from repeated minor trauma, nail fold and adjacent soft tissue deformities such as nail fold hypertrophy, onychomycosis, onychocryptosis, xerosis, etc. The first and the fifth toes are commonly affected.4,5

Onychoclavus (Subungual Heloma/Corn)
It is a hyperkeratotic process in the nail area, mostly under the distal nail margins, due to bony deformity or abnormal foot function, with resultant repeated trauma and localized pressure on the distal nail bed and hyponychium. It occurs mostly in the great toe, appearing as a dark spot under the nail plate. Intense tenderness will be present usually and overlying nail plate may be elevated or split. It should be differentiated from subungual melanoma, subungual exostosis, foreign body or an epidermoid cyst.4,5
Onychocryptosis (Ingrown Nails)
This condition results when part of the nail plate pierces the lateral nailfold. Three major types are known: overcurvature of the nail plate (pincer nail), subcutaneous ingrowing toenail and hypertrophy of the lateral nail fold. Clinically, it manifests as inflammation of the nail fold, often with granulation tissue formation, sepsis, pain at rest and tenderness of the involved digit.4,5
The causes include improper cutting of the nails, external pressure due to pointed toed or high heeled footwear, long toes and other deformities, hyperhidrosis, poor foot hygiene, prominent nail folds, presence of a spicule, etc.10 In the elderly with impaired arterial circulation and sensation, infection, osteomyelitis and gangrene may supervene.4,5
Splinter Hemorrhages and Subungual Hematomas
Splinter hemorrhages, which are most commonly traumatic in the elderly, were found in 16% of 220 elderly patients older than 65 years.4 They are black in color and located in the middle or distal third of the fingernail. In contrast, splinter hemorrhages induced by systemic disorders are red in color and proximal in location.4,5
Subungual hematomas are also usually traumatic, but may be found in elderly patients on anticoagulant therapy or patients of amyloidosis, bullous pemphigoid and diabetes mellitus.4 They are red and painful when of recent onset, and dark blue and non-tender when old. Characteristically, these are carried forward with the growth of the nail.
Infections/Infestations
The nail apparatus may get primarily infected or involved in infections of the adjacent structures.
Onychomycosis
The prevalence of onychomycosis increases with age, reaching nearly 20% in patients over 60 years.11 It is especially common in the elderly, many a times involving both toenails and fingernails. Great toenail is the commonest to be involved. The subtypes of onychomycosis are distal or distal lateral subungual onychomycosis (DSO or DLSO), proximal subungual onychomycosis (PSO), white superficial onychomycosis (WSO), candidal onychomycosis and endonyx onychomycosis. The first three types are usually caused by dermatophytes such as Trichophyton rubrum and Trichophyton mentagrophytes. The non-dermatophyte molds such as Scopulariopsis brevicaulis, Hendersonula toruloidea and Scytalidium hyalinum are found more frequently in the elderly.4 Mixed saprophyte infections of the nail are more common in this age group.74
Paronychia
It is infection or inflammation of the nail fold, which can be acute or chronic.
Acute paronychia is the bacterial infection of the nail folds, usually caused by Staphylococcus aureus or Pseudomonas species. Most cases are trauma induced and involve only one nail. The nail folds are erythematous, tender and contain pus.12
Chronic paronychia, caused by Candida species or gram negative bacteria (Proteus species or Klebsiella species), presents as red, swollen, boggy, tender nail folds with loss of cuticle and a patent proximal nail groove. Multiple transverse ridges may be seen in the nail plate.4,9
Subungual Scabies
Sarcoptes scabiei mites may inhabit the subungual hyperkeratotic debris, leading to persistent infestations or epidemics of scabies.13
Periungual Warts
They are due to infection with human papilloma virus. These occur especially in persons receiving immunosuppressive therapy.4,5
Neoplastic Conditions
Subungual Exostosis
This is a benign, tender, nodular, hyperkeratotic bony proliferation, involving the medial side of the great toe most commonly. This is associated with onychodystrophy / onychoclavus of the overlying nail.14 Trauma and faulty biomechanics is the commonest cause in the elderly.
Myxoid Pseudocysts (Mucous Cysts or Periungual Ganglion)
They are probably the commonest benign tumours. They are commoner in females and usually involve the proximal nail fold of fingers. They are asymptomatic, soft to firm, cystic/fluctuant, sometimes causing transverse nail depressions.
Subungual Melanoma
It is common in the elderly, mostly affecting the great toe. The peak incidence was in eighth decade in one study.3
Others
Bowen's disease, squamous cell carcinoma, basal cell carcinoma and glomus tumor are also more frequent in this age group.3
Nail Changes in Elderly Due to Skin Diseases
Various skin conditions like Psoriasis, Lichen Planus, Eczemas, Darrier's disease and Alopecia areata can present with their characteristic nail changes in elderly population.75
Nail Signs of Systemic Diseases
Conditions Involving Proximal Nail Fold
Bywater's Lesions
These are small areas of palpable purpura in the proximal or lateral nail fold or both. They are classically associated with rheumatoid vasculitis, but also associated with small vessel vasculitis and Wegener's granulomatosis.15
Osler's Nodes
These are small, red, tender nodules over the finger pulp or nail fold or both, which are seen in subacute bacterial endocarditis.16
Nail Fold Telangiectasis
These can be visualized in the proximal nail fold because capillary loops thin to a row of single loops at the distal most portion of the fold, near the cuticle. Overt disruption of the capillaries can be seen with naked eye, but specific telangiectatic patterns can be seen using magnification.16 Dilated capillaries with bordering avascular areas are a specific pattern. Distortion and budding of capillaries, enlargement of loops and loss of capillaries are associated with dermatomyositis, scleroderma and overlap diseases.16 Tortuous, meandering capillaries, a less specific pattern, is associated with systemic lupus erythematosus and Raynaud's phenomenon.16
Conditions Involving Lunula
Lunular Dysmorphology
Macrolunula
Enlarged lunula is seen normally in some Indians. It is also noted in some nail disorders like habit-tic deformity and median nail dystrophy, endocrine conditions, mainly hyperthyroidism or after application of hydrocortisone to the cuticle.
Microlunula (Diminished Size) or Alunula/Anolunula (Absence of Lunula)
These can be associated with atherosclerosis, iron deficiency anemia, HIV, leprosy, multiple myeloma, chronic obstructive pulmonary disease, renal failure, rheumatoid arthritis, scleroderma, nerve injury, lymphedema, malnutrition, endocrine diseases like acromegaly, Frohlich's disease, hyperthyroidism, hypothyroidism, hypopituitarism, porphyria cutanea tarda, erythropoietic protoporphyria, focal dermal hypoplasia (Goltz syndrome), nail-patella syndrome, pachyonychia congenita and penicillamine therapy.6
Lunular Dyschromia
Blue (Azure) Lunula
This is seen in Wilson's disease, hemoglobin, M disease, hereditary acrolabial telangiectases, argyria, combination therapy involving cyclophosphamide, vincristine, vinblastine, 76dactinomycin, doxorubicin, dacarbazine, 5-fluorouracil, bleomycin, other drugs like zidovudine, quinacrine, phenolphthalein purgative, etc.6
Red Lunula
This may be seen in congestive heart failure, endocrine (diabetes mellitus), gastrointestinal, hematologic, hepatic, infectious (lymphogranuloma venereum), neoplastic, neurologic, pulmonary, renal and rheumatologic disorders. Other conditions include carbon monoxide poisoning, chronic idiopathic lymphedema, malnutrition, senile macular degeneration, alcoholism, tobacco addiction, and drug therapy with azathioprine, corticosteroids, hay fever, pollen antigen, procainamide, antilymphocyte globulin. Cutaneous disorders associated with red lunula include alopecia areata, vitiligo, habit-tic deformity of nail, median nail dystrophy, trachyonychia, chronic urticaria, nail-patella syndrome, lichen sclerosus et atrophicus and psoriasis. It may also be idiopathic.6
Yellow Lunula
This is seen with topical exposure to insecticides and weed killers like paraquat and tetracycline therapy (after 1 month therapy).6
Others
Black lunula is seen in trauma, brown in busulfan therapy, gray or opaque in hyperthyroidism, leprosy, green in pseudomonas infection and purple in idarubicin and cytarabine therapy.
Longitudinal lunular bands may be seen in Darier's disease, glomus tumor and with various drugs.6
Conditions Involving Nail Bed
Chromonychia
Diffuse, bluish discoloration of the nail bed is characteristically associated with ingestion of silver and antimalarial drugs. A small, painful, bluish macule in the nail bed indicates glomus tumor. Pallor of the nail bed is seen in anemia. Cherry red nail bed is a sign of carbon monoxide poisoning.16
Splinter Hemorrhages
Splinter hemorrhages in multiple nails, especially if distributed close to lunulae are a sign of systemic disease. They are classically associated with subacute bacterial endocarditis, but most frequently they are traumatic. Other causes include mitral stenosis, vasculitis, scurvy, anemia, leukemia, Burger's disease, hypertension, arterial thrombi, cryoglobulinemia, hemochromatosis, thrombocytopenia, fungal infections, rheumatic fever, rheumatoid arthritis, dermatomyositis, Behcet's disease, Reiter's syndrome, systemic lupus erythematosus, acrocyanosis, chronic glomerulonephritis, dialysis patients, cirrhosis, hepatitis, diabetes, thyrotoxicosis, hypoparathyroidism, malignancies, and drugs like tetracyclines, psoralens and ketoconazole. Simultaneous involvement of all nails is pathognomonic of trichinosis.16
Apparent Leukonychia
White appearance of the nails due to pathology in the subungual tissue and nail bed is known as “apparent leukonychia”, in contrast to “true leukonychia” which is due to matrix involvement and 77“pseudoleukonychia” which is seen due to superficial onychomycosis and keratin granulations after nail enamel application.17 Various presentations include:
Terry's Nails
They are characterized by a proximal white color with a distal normal pink band of 0.5-3 mm width(Figure 6.3) They are seen in cirrhosis of liver, chronic congestive heart failure, adult onset diabetes mellitus and malnutrition.16
Half-and-Half Nails of Lindsay
These have a proximal dull white area with the distal 20–60% red, pink or brownish portion, and are seen in uremic patients18 (Figure 6.4).
Muehrcke's Lines
These are two transverse, narrow, white bands of pallor present parallel to the lunula, representing an abnormality of the vascular nail bed. Pressure applied on the distal plate causes the bands to disappear.


They are seen in hypoalbuminemia (less than 2.2 g/100 ML), nephrotic syndrome, glomerulonephritis, malnutrition, acrodermatitis enteropathica or following chemotherapy.16
Quencke's Pulse
It is a visible capillary pulse over the nail bed or nail fold, seen in aortic insufficiency.16
Onycholysis
It is a separation of the nail plate from nail bed beginning distally and progressing to the proximal end.16 It occurs mainly due to exogenous factors like trauma, local allergy and occupational exposure to irritants, fungi and drugs. Onycholysis due to drugs may be photo-induced as in case of benoxaprofen, chloramphenicol, chlorpromazine, chlortetracycline, demethylchlortetracycline (painful), doxycycline (painful), minocycline, tetracycline, oral contraceptives, psoralens, fluoroquinolones, thiazides, 5-fluorouracil, captopril, etc. Non –photoinduced onycholysis occurs with bleomycin, doxorubicin, 5-fluorouracil, retinoids, tetracycline, captopril, gold, metronidazole, etc.
Endogenous causes include various dermatological diseases like psoriasis, lichen planus, Reiter's disease, dermatitis, hyperhidrosis, alopecia areata, porphyria cutanea tarda (photo induced), pemphigus vegetans and foliaceus, epidermolysis bullosa simplex, etc. neoplasms, notably, squamous cell carcinoma, mycosis fungoides, histiocytosis-X; systemic diseases including endocrine diseases, iron deficiency anemia, lupus erythematosus, etc.9,16 It may be idiopathic.16
Onychomadesis
This denotes complete onycholysis or spontaneous nail shedding, mostly occurring due to neurovascular change. It is seen in exanthems (measles and scarlet fever), hypocalcemia with arteriolar spasm, diabetes, other vascular diseases, athletes, and drug therapy with etretinate, carbamazepine, paratharmone, penicillin anaphylaxis, mercaptopurine, quinacrine and arsenic and lead poisoning.16
Conditions Involving Hyponychium
Pterygeum Inversum Unguis
It is a persistent adherence of the distal portion of the nail bed or hyponychium to the ventral surface of the nail plate that obliterates the normal distal separation of the hyponychium from the plate. It may be painful in up to 20% and may affect all 10 fingernails in up to 40% of cases.72 It is most commonly associated with lupus erythematosus and scleroderma and may also occur in other conditions with impaired circulation such as acrosclerosis, digital ischemia, Raynaud's phenomenon, diabetes, stroke, and leprosy.16
Conditions Involving Nail Plate
Onychorrhexis
Longitudinal ridging of the nails, apart from being more prominent in the elderly, is also associated with systemic diseases such as rheumatoid arthritis, sarcoidosis, amyloidosis, 79iron deficiency anemia, peripheral circulatory disorders, multicentric reticulohistiocytosis, follicular mucinosis, genetic abnormalities, mycotic diseases, poisoning (especially arsenic), scleroderma, hypothyroidism, hypoparathyroidism, gout, Raynaud's phenomenon, lupus, graft versus host disease, AIDS and zinc deficiency.10,73 Associated skin disorders are leprosy, cicatricial pemphigoid, pemphigus foliaceus, lichen nitidus, lichen planus and pityriasis rubra pilaris. Drugs causing onychorrhexis include azidothymidine, lithium, penicillamine and retinoids.16
Trachyonychia
This term is used to describe rough nail plates with a characteristic gray opacity, brittle and split ends, longitudinal ridging, and a rough sandpaper like surface. It is associated with alopecia areata (3.65% of patients overall and 15.4% of those with alopecia universalis) lichen planus, psoriasis, ichthyosis vulgaris or may be idiopathic idiopathic (20-nail dystrophy).16 Other associated conditions are dark red lunulae and knuckle pads, selective immunoglobulin A deficiency, ectodermal dysplasia, lithium, immune thrombotic purpura and autoimmune hemolytic anemia.16
Beau's Lines
This denotes transverse grooves or depressions of the nail plate occurring with acute systemic illness. The conditions which may induce Beau's lines are numerous and include febrile illness, infectious diseases like typhus fever, rheumatic fever, diphtheria, syphilis, parotitis, malaria, gonococcal arthritis, erythema nodosum leprosum, and mucocutaneous lymph node syndrome, nutritional disorders like protein deficiency and pellagra, myocardial infarction, peripheral vascular disease, Raynaud's disease, pulmonary embolism, diabetes, hypothyroidism, hypocalcemia, hypoparathyroidism, Sheehan's syndrome, diarrhea, chronic enterocolitis, subacute and chronic pancreatitis, sprue, severe gastritis, acrodermatitis enteropathica, surgery, chronic alcoholism, arsenic toxicity, hysteria, epilepsy, parturition, dysmenorrheal, chronic local skin disease including paronychia, eczema, pustular psoriasis, pemphigus foliaceus, trauma, carpal tunnel syndrome, and drugs including antimitotic drugs, dapsone, retinoids, carbamazepine, etc.16
Hapalonychia
This is a term for soft nails, which can be associated with local occupational causes, skin diseases like psoriasis and eczema, systemic diseases like hypochromic anemia, arsenic poisoning, infectious diseases, severe toxemia, rheumatoid arthritis, vitamin deficiency (A, B6, C), osteoporosis, osteomalacia, myxedema, leprosy, hemiplegia, hypopituitarism, peripheral, Raynaud's disease, scleroderma and multiple sclerosis.16
Chromonychia
Chromonychia can occur due to increased melanogenesis in the matrix (brown discoloration), imperfect keratinization (white discoloration), infection, or byproducts of metabolism or medications. Pigmentation is more likely due to internal causes when it is not possible to scrape the color off the nail plate surface. It is also of internal origin when the shape of proximal border of the discoloration corresponds to shape of the lunula, unlike external factors where the shape corresponds to shape of proximal nail fold.1680
Systemic diseases can produce diffuse, brown pigmentation of the nails due to increased melanin production. Adrenal insufficiency, pituitary tumors, acanthosis nigricans, vitamin B12 deficiency, hemochromatosis, hyperbilirubinemia, hyperthyroidism, hypopituitarism, porphyria and syphilis are the conditions which can produce it.16 Drugs causing similar pigmentation include anticancer drugs like melphalan, hydroxyurea, doxorubicin (adriamycin), busulfan, 5-fluorouracil, methotrexate, cyclophosphamide and bleomycin, tetracycline derivatives, 8-methoxypsoralen, antimalarials, sulfonamides, phenothiazines, phenindione, mercury, gold, phenytoin, timolol, and azidothymidine.16,19
Exogenous factors causing nail pigmentation include ink, photographic developer, shoe polish, nicotine (smokers), henna, anthralin, nail enamel, and certain dematiaceous fungi (diffuse brown pigmentation) namely Proteus mirabilis, Hormodendrum elatum, Alternaria grisea tenuis, Acrotherium niger, Botryoploidia theobromae, Hendersonula toruloidea.16
Longitudinal brown bands (longitudinal melanonychia) occur normally in African-American persons. Single or multiple bands can be seen in neoplastic or non-neoplastic conditions including various nevi, endocrine and other systemic disorders, fungal infections, skin diseases like lichen planus, lichen striatus, prurigo vulgaris and Laugier-Hunziker syndrome, malnutrition, vitamin D deficiency and all drugs which can cause diffuse pigmentation.16,19 Subungual melanoma can cause similar longitudinal pigmentation accompanied by pigmentation of the proximal nail fold, known as “Huthinson's sign”.16 “Pseudo Hutchinson's sign” refers to pigment visualized through the relatively transluscent cuticle and proximal nail fold, as seen in Laugier-Hunziker syndrome, minocylcline therapy, Peutz-Jegher's syndrome, trauma, biopsy, Bowen's disease, ethnic pigmentation, radiation therapy, malnutrition, AIDS, and congenital nevus.16
Transverse pigmented bands may appear if a treatment is recurrently started and stopped. They are mostly seen with radiotherapy, electron beam therapy, azidothymidine and cancer chemotherapy.16,19
Blue discoloration is seen in Wilson's disease and argyria. Diffuse blue discoloration is reported in bronchiectasis, minocycline, azidothymidine or idiopathically in “azure nails”.16
True Leukonychia
True leukonychia is whitening of the nails due to matrix involvement. It can be transverse, diffuse, longitudinal, or punctuate.
Diffuse leukonychia is associated with leprosy, hemochromatosis, hypocalcemia, and acanthosis nigricans.16
Transverse leukonychia is presence of transverse, opaque, white bands that tend to occur in the same relative position in multiple nails, due to parakeratotic cells incorporated in the nail plate by a compromised matrix. Like Beau's nails, the distance of these bands from proximal nail fold indicates the time of insult. They are characteristically seen in arsenic poisoning, known as Mees’ lines. Other conditions include thallium or carbon monoxide exposure, leprosy, malaria, trichinosis, herpes zoster, renal failure, after renal transplant, myocardial infarction, cardiac insufficiency, Hodgkin's disease, acrodermatitis enteropathica, pellagra, pneumonia, child birth, menstrual cycle, chemotherapeutic drugs, psoriasis, erythroderma, etc.16
Longitudinal bands of leukonychia are seen in candidiasis, Darier's disease, Hailey-Hailey disease, and quinacrine use.16
Punctate leukonychia may be traumatic or seen in case of contact with strong chemical solvents, fungal infections, cryotherapy, infections like measles, typhus, scarlet fever, rheumatic fever, diphtheria, syphilis, diabetes, arsenic and lead poisoning, psoriasis, dyshidrosis, etc.1681
Yellow Nail Syndrome
It is defined as the triad of yellow nails, lymphedema and pulmonary complications.16,20 The nails have a striking yellow color, increased transverse curvature, absent lunula and cuticle, a tendency to form a “hump” and a variable degree of onycholysis. The nail change may be independent of systemic disease. Slow rate of growth or lipofuscin pigment may be the cause of the nail color. Growth rate is less than 0.2 mm/week, and patients often remark that the nails have “stopped growing”.10 Patients have some type of edema, usually ankle edema and sometimes facial edema. Pleural effusion is part of the triad.16,20
Conditions associated with yellow nail syndrome are edema of the lower extremities including Milroy's disease, facial edema, pleural effusion, chronic bronchitis, sinusitis, bronchiectasis, chronic pulmonary infections, upper and lower respiratory chronic disease, chronic pulmonic and hepatic tuberculosis, giant cell interstitial pneumonitis, asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, cancer of the larynx, lymphoma, sarcoma, endometrial carcinoma, malignant melanoma, infiltrating ductal carcinoma of the breast, Hodgkin's disease, mycosis fungoides, carcinoma of the gall bladder, chronic sinusitis, chronic nasal obstruction and rock hard cerumen, recurrent cellulitis, syphilis, AIDS (controversial), leucopenia, hypogammaglobulinemia, complete absence of IgA, low levels of IgM, macroglobulinemia, thyroid disease, diabetes, breasts of unequal size, rheumatoid arthritis, Raynaud's disease, SLE, mental retardation, nephrotic syndrome, hypoplastic kidney, myocardial disease, drugs like D-penicillamine, bucillamine, and idiopathic.16
Clubbing (Hippocratic Nails/Watch Glass Nails)
In clubbing, there is increased transverse and longitudinal nail curvature with hypertrophy of the soft-tissue components of the digit pulp (Figure 6.5). Clubbing is said to be present if the angle between the nail plate and the proximal nail fold (Lovibond's angle) is 180° or more, compared to the usual 160°. Curth's angle at the distal interphalangeal joint is normally 180° but this is diminished to less than 180° in clubbing. Schamroth's window is normally seen when the dorsal aspects of two fingers from opposite hands are apposed, revealing a window of light. This window closes in clubbing.21
The cause of clubbing appears to be increased blood flow through the vasodilated plexus of nail unit vasculature. Altered vagal tone and microvascular infarcts have been implicated.21

Clubbing may be inherited or acquired. It is most commonly bilateral and often begins in the thumb and index finger. Bilateral clubbing occurs mostly (80%) due to cardiopulmonary disease. Disorders of the liver, gastro-intestinal tract and kidney may also present with bilateral digital clubbing. Endocarditis, congestive heart failure, cirrhosis of the liver, ulcerative colitis and chronic pyelonephritis are the conditions commonly associated. Unilateral clubbing is seen in lymphadenitis, pancoast tumor of the lungs and erythromelalgia. Uni-digital clubbing occurs in vascular lesions of the same extremity like aneurysm, arterio-venous fistula or peripheral shunt or tumors.16
The syndrome of acquired hypertrophic pulmonary osteoarthropathy, is a combination of clubbing, muscle weakness, peripheral neurovascular disease, bone and joint pain and swelling and hypertrophy of the upper and lower extremities.16 This can be hereditary (primary) as seen in pachydermoperiostosis (Touraine-Solente-Gole syndrome) or acquired (secondary), which is in turn of two types. First, hypertrophic pulmonary osteoarthropathy (Bamberger-Pierre-Marie syndrome) is characterized by hypertrophic osteoarthropathy confined to the lower extremities and is often caused by recurrent infections of lower limbs following bypass grafting. The second type is most often associated with malignant tumors of the chest, especially bronchogenic carcinoma.10 Other associations include suppurative pulmonary lesions, rheumatic fever, rheumatoid arthritis, infective arthritis, thrombophlebitis, congestive heart failure, nutritional edema, peripheral neuropathy, acromegaly and ulcerative colitis.16
Koilonychia
It is defined as spoon shaped nail plates. It is thought to occur because of relatively low distal matrix, compared with the proximal matrix, which causes nail plate growth to occur in a downward direction as it grows toward the nail bed. It may be idiopathic, inherited or acquired.
Acquired koilonychia is the commonest type, most commonly acquired from trauma, dermatological disease (especially psoriasis and onychomycosis), and distal ischemia (especially Raynaud's phenomenon). It has classically been a sign of iron deficiency anemia (Plummer-Vinson syndrome and following gastrectomy). It is also seen in post-hysterectomy patients, iron malabsorption by the intestinal mucosa, cystine deficiency, hemoglobinopathy SG, polycythemia, hemochromatosis, Banti's syndrome, coronary disease, polyglobias (erythropoietin producing tumors), syphilis, fungal disease, acromegaly, hypothyroidism, thyrotoxicosis, occupational exposure to gasoline, solvents, engine oils, acids, alkalies, thioglycolates (hair dressers), house wives, nail biting, frost bites, thermal burns, avitaminosis B2 and especially C, pellagra, malnutrition, Raynaud's disease, scleroderma, lichen planus, porphyria cutanea tarda, Darier's disease, incontinentia pigmenti, alopecia areata, psoriasis, acanthosis nigricans, after kidney transplantation, carpal tunnel syndrome, primary amyloidosis, and sometimes idiopathic.16
Evaluation of nails is an important component of all physical examinations in elderly, as nails may show changes that are markers for a wide range of systemic disorders. Awareness of the signs and symptoms of the aging nail is essential for better assessment and management of the onychologic concerns of the elderly patients.
References
- Drake LA, Dinehart SM, Farmer ER, Goltz RW, Graham GF, Hordinsky MK, et al. Guidelines of care for nail disorders. J Am Acad Dermatol 1996;34:529–33.
- Baran R, Dawber RPR. The nail in childhood and old age. In: Baran R, Dawber RPR, editors. Diseases of the nails and their management. 2nd Edition.Oxford: Blackwell Scientific Publications; 1994. p.81-96.
- Cohen PR, Scher RK. Geriatric nail disorders: diagnosis and treatment. J Am Acad Dermatol 1992;26:521–31.
- Cohen PR, Scher RK. Aging. In: Hordinsky MK, Sawaya ME, Scher RK, editors. Atlas of hair and nails. Philadelphia: Churchill Livingstone; 2000.p.213-25.
- Cohen PR. The lunula. J Am Acad Dermatol 1996;34:943–53
- Cohen PR, Scher RK. Nail changes in the elderly. J Geriatric Dermatol 1993;1:45–53.
- Scher RK. Brittle nails. Int J Dermatol 1989;28:515–6.
- Verbow J. Face, hair, nail and callosities. In: Skin diseases in the elderly. London: William Heinemann Medical Books Ltd; 1974.p.55-74.
- Mortimer PS, Dawber RPR. Trauma to nail unit including occupational sports injuries. Dermatol Clin 1985;3:415–20.
- Loo DS. Cutaneous fungal infections in the elderly. Dermatol Clin 2004;22:33–50.
- Rich P. Nail disorders: diagnosis and treatment of infectious, inflammatory and neoplastic nail conditions. Med Clin North Am 1998;82:1171–83.
- Scher RK. Subungual scabies. Am J Dermatopathol 1983;5:187–9.
- Salasche SJ, Garland LD. Tumors of the nail. Dermatol Clin 1985;3:521–30.
- Bywaters EGL. Peripheral vascular obstruction in rheumatoid arthritis and its relationship to other vascular lesions. Ann Rheum Dis 1957;16:84–103.
- Holzberg M. Nail signs of systemic disease. In: Hordinsky MK, Sawaya ME, Scher RK, editors. Atlas of hair and nails. Philadelphia: Churchill Livingstone; 2000.p.59-70.
- Grossman M, Scher RK. Leukonychia: review and classification. Int J Dermatol 1990;29:535–41.
- Lindsay PG. The half-and-half nail. Arch Intern Med 1967:583-7.
- Jeanmougin M, Civatte J. Nail dyschromia. Int J Dermatol 1983;22:279–90.
- Samman PD, White WF. The “yellow nail” syndrome. Br J Dermatol 1964;76:153–7.
- De Berker DAR, Baran R, Dawber RPR. Disorders of nails. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's textbook of dermatology. 7th Edition. Oxford: Blackwell science; 2004.p.62.1-62.62.
Lichen planus is a common inflammatory condition seen by the dermatologists, which involves skin, mucous membranes and nails. Lichen planus is derived from the word “lichen” that in greek means tree moss and “planus” that means flat. Overall prevalence of lichen planus is less than 1% in general population, with almost 10% of the patients having involvement of nails.1 Not much has been written about nail lichen planus (NLP) in literature, but this not so common condition involving nails can cause infiltration of nails and if not treated on time may produce nail matrix destruction and leave behind permanent scarring.
Epidemiology
Nail involvement is seen in approximately 10% of the patients with lichen planus and almost 25% of these patients with NLP have involvement of other sites either before or after the involvement of nails.2 Initially considered to be a rare presentation in childhood, but recent studies have shown that prevalence of NLP is 11% in childhood, similar to what is seen in adults. Extra-cutaneous involvement is less frequent (13.3%) in childhood NLP as compared to adults.3 85NLP predominantly involves males and involvement of fingernails is much more common as compared to toenails, both in adults and childhood.
Clinical Features
The nail apparatus consists of hard keratin layer, nail plate, nail bed, nail matrix, nail folds and the hyponychium. Nail matrix gives rise to most of the nail plate, proximal matrix giving rise to dorsal nail plate and dorsal matrix giving rise to intermediate and ventral nail plate. The clinical features of NLP depends on the part of the nail which is affected, with nail matrix being involved in 90% of the cases.4 Nail bed involvement is seen in 10% of the cases, with toenails being more frequently involved in cases with nail bed involvement.4 The various clinical features seen in NLP are mentioned in Table 7.1.
Nail Matrix Changes
Longitudinal ridging (onychorrhexis) and splitting are the most common clinical manifestation of NLP.5, 6 Nail plate appears opaque, brittle with multiple longitudinal ridges, furrows and distal margins of nails shows splitting (Figures 7.1 and 7.2).
Dorsal pterygium (“pterygium” in latin means wings) is the least common (17.9%) manifestation, but virtually pathognomonic for NLP.4 Pterygium initially may just present as a bulge in the proximal nail fold followed by gradual extension of the proximal nail fold over the nail plate. The nail plate becomes fissured because of the fusion of the nail fold to the nail bed and splits progressively as the pterygium widens. Further progression of the pterygium causes scarring of the matrix, hence even if the disease subsides later, the scar formed in the active phase prevents normal regrowth of the nail plate. Complete scarring of the nail matrix causes anonychia, which is a common manifestation of bullous and ulcerative lichen planus (Figure 7.3).
Chromonychia generally presents as punctate redness of lunula in most of the cases (31.3%) of NLP, but few cases of longitudinal erythronychia and melanonychia have also been reported in the literature.4 Another unusual presentation of NLP which is more frequently seen in children is “idiopathic atrophy of nails”.7
|


This presents as progressive atrophy of the nail plate and nail fold, involving most of the digits with minimal cutaneous features. Very few patients with NLP can also present with nail pitting, pits varying from few to too many in number giving a rough and dull appearance to the nail. Trachyonychia (20-nail dystrophy) is an uncommon manifestation of NLP, seen in 22.4% of the patients in a study conducted by Goettmann et al.4 It clinically manifests as rough and lustreless nails due to irregular pitting and multiple longitudinal striations.8 NLP presenting as trachyonychia can be distinguished from other causes of trachyonychia due to the presence of other features like nail splitting, pterygium formation and redness of lunula. 87

Figure 7.3: Longitudinal ridging (index finger nail), anonychia (middle finger) and pterygium formation (ring finger nail)
Nail Bed Involvement
Nail bed involvement in lichen planus is uncommon as compared to nail matrix involvement. Nail bed involvement can clinically present as violaceous papules in the nail bed, subungual hyperkeratosis and onycholysis.5, 6 Onycholysis can be present with or without subungual hyperkeratosis and if separation is complete it can result in complete shedding of the nail plate. “Pup tent” is a characteristic manifestation of NLP due to nail bed involvement, where clinically the nail plate splits and is longitudinally elevated with lateral edges sloping downward.
Unusual Clinical Presentations
Paronychia can be present sometimes giving a violaceous appearance to the proximal nail fold. Occasionally even tiny violaceous papules can be seen on the proximal and lateral nail folds. Diffuse yellowish discoloration can also be a rare clinical manifestation mimicking the yellow nail syndrome, this is most commonly found to be an association with bullous lichen planus.9 Anonychia can be a presentation of ulcerative lichen planus and can be the only manifestation of the disease.
Diagnosis
NLP can be easily picked up from clinical examination, but as NLP primarily is a scarring process involving the nails and hence in case of any doubt nail biopsy should be done for timely diagnosis and effective management. As nail matrix is involved predominantly, nail matrix biopsy is usually sufficient, but a nail bed biopsy might be required to differentiate NLP from nail psoriasis. A 3 mm punch biopsy will usually suffice, but other methods which can be employed are horizontal elliptical biopsy, tangential (shave) excision or a proximal nail fold-lunula double punch biopsy. The features of NLP in common with the cutaneous lichen planus are compact hyperkeratosis, hypergranulosis, irregular acanthosis, basal layer degeneration, presence of Civatte bodies, 88dense lichenoid infiltrate, melanin incontinence and collagen bundles in papillary dermis. The differentiating features between NLP and skin lichen planus are presented in Table 7.2.
Common Differential Diagnosis
Treatment
Nail lichen planus is a chronic cosmetically disfiguring condition for which optimal treatment has not been established. Steroids remain the mainstay of management, which can either be used as topical, intralesional or systemic therapies. Potent topical steroids can be used under occlusion for nail bed involvement.5 Intralesional and systemic therapy are found to be more effective for nail matrix involvement. Intralesional steroids are generally used only when a few fingers are involved. Monthly injections of intralesional triamcinolone acetonide (5–10 mg/ML) in the proximal nail folds have shown complete resolution after 6-8 months in finger nails and 9–12 months in toe nails.10–12 Side effects of intralesional therapy are pain, subungual hematoma, proximal nail fold hypopigmentation and atrophy. Intramuscular injections (0.5 mg/kg) of triamcinolone given monthly have shown remission in 3 to 4 months.12 Initial treatment with oral prednisolone for 3 to 4 weeks has been found to be effective in minimizing the inflammation. Oral steroids can be followed by a maintenance therapy with low dose oral steroids or potent topical steroids. Other therapeutic modalities which can be tried are systemic antimalarials, etretinate, psoralen and griseofulvin.5,13 After showing an initial response with therapy most of the patients have relapses and have to be managed accordingly. Pterygium is an irreversible condition and hence should not be treated.14
|
References
- Luis-Montoya P, Domínguez-Soto L, Vega-Memije E. Lichen planus in 24 children with review of the literature. Pediatr Dermatol. 2005;22:295–8.
- Tosti A, Peluso AM, Fanti PA, Piraccini BM. Nail lichen planus: clinical and pathologic study of twenty-four patients. J Am. Acad. Dermatol. 1993;28(5 Pt 1):724–30.
- Tosti A, Piraccini BM, Cambiaghi S, Jorizzo M. Nail lichen planus in children: clinical features, response to treatment, and long-term follow-up. Arch Dermatol. 2001;137:1027–32.
- Goettmann S, Zaraa I, Moulonguet I. Nail lichen planus: epidemiological, clinical, pathological, therapeutic and prognosis study of 67 cases. J Eur Acad Dermatol Venereol. 2011 DOI: 10.1111/j.1468-3083.2011.04288.x [cited 2012 Jul 4].
- Baran R, Holzberg M. Nails and dermatological diseases. In: Baran R, Dawber RPR, editors, Baran and Dawber's Disease of the Nails and their Management. 4th Edition. London: Wiley-Blackwell Ltd. 2005. p282-288.
- Tosti A, Piraccini BM. Biology of nails and nail disorders. In: Wolff K, Goldsmith LA, Katz SI, Gilchrist BA, Paller AS, Leffell DJ, editors, Fitzpatrick's Dermatology in General Medicine. 7th edn. USA: Mc GrawHill Ltd. 2008. p789-799.
- Tosti A, Piraccini BM, Fanti PA, Bardazzi F, Di Landro A. Idiopathic atrophy of the nails: clinical and pathological study of 2 cases. Dermatology (Basel). 1995;190(2):116–8.
- Ruiz-Villaverde R, Sánchez-Cano D, Pacheco Sánchez Lafuente FJ. Twenty-nail dystrophy and lichen planus. An Pediatr (Barc). 2007;66:195–6.
- Haneke E. Isolated bullous lichen planus of the nails mimicking yellow nail syndrome. Clin Exp Dermatol. 1983;8:425–8.
- Grover C, Bansal S, Nanda S, Reddy BSN. Efficacy of triamcinolone acetonide in various acquired nail dystrophies. J Dermatol 2005;32:963–8.
- Brauns B, Stahl M, Schön MP, Zutt M. Intralesional steroid injection alleviates nail lichen planus. Int J Dermatol. 2011;50:626–7.
- Piraccini BM, Saccani E, Starace M, Balestri R, Tosti A. Nail lichen planus: response to treatment and long-term follow-up. Eur J Dermatol. 2010;20:489–96.
- Evans AV, Roest MA, Fletcher CL, Lister R, Hay RJ. Isolated lichen planus of the toe nails treated with oral prednisolone. Clin Exp Dermatol. 2001;26:412–4.
- Kato N, Ueno H. Isolated lichen planus of the nails treated with etretinate. J. Dermatol. 1993;20:577–80.
Introduction
Psoriasis is a chronic skin disease that affects millions of people around the world. The nails have been found to be involved in up to 50% of cases, although studies have shown that life time incidence of nail involvement in psoriatic patients is approximately between 80–90%.1
It is interesting to know that between 5–7% of patients have affected nails without skin lesions. Nail psoriasis may be a sign of uncontrolled inflammation as well as a severe form of psoriatic disease process requiring more aggressive treatment. It is well known that the incidence of nail psoriasis is associated with longer duration of disease, with polyarticular disease, unremitting progressive arthritis as well as with enthesitis.2, 3, 4
Approximately 80% of the patients of psoriatic arthritis show concurrent nail involvement. The point of concern is that despite all this knowledge, nail psoriasis is a neglected aspect of treatment of the disease, as physicians often believe that the condition is difficult to treat. Many physicians are not willing to use systemic medication to treat nail disease with psoriasis. It is also challenging to deliver topical drugs to the various areas of the nail unit.91
There have been limited published data and very few larger, randomized controlled trials (RCTS) on treatment of psoriasis with reference to nail involvement.5
Structure of the Nail Unit with Reference to Nail Psoriasis
The nail unit is comprised of the nail plate, the proximal nail fold, the matrix, the nail bed and the hyponychium.6
Nail Plate
The nail plate is a rectangular translucent hard structure that overlies the digital ends of the digits. Seen through the nail plate at its proximal part, are white semi-circular structures called lunulae which depict the digital matrix.
Nail Folds
The lateral nail folds are extensions of the skin of the nails of the digits. They join the nail beds medially.
The proximal nail fold (PNF) is a continuation of the skin of the digit. It folds underneath itself and rests above the nail matrix. Thus, it has two surfaces– dorsal and ventral. At the junction of these two surfaces lies the eponychium or the cuticle, the function of which is to seal off the potential space between the nail fold and the nail plate.
Nail Matrix
This is the most important germinative layer of the nail unit and is responsible for the formation of almost the entire nail plate. It has three regions: the dorsal, the intermediate and the ventral sub-divisions. The dorsal matrix consists of the superficial layer of the nail plate while the intermediate forms the intermediate layer of the nail plate. The ventral matrix which is the most distal part of the matrix along with the most superficial part of the nail bed forms the deepest layer of the nail plate.
Nail Bed
It is the area beneath the nail plate extending from the lunula to the hyponychium. It consists of a thin epidermal layer (that forms part of the ventral nail plate) and the dermis, which is rich in blood vessels. There is no subcutis.
Hyponychium
This is the part of the nail unit that is situated underneath the free edge of the nail plate. It indicates the transition of the nail bed to the epidermis of the fingers and toes.
Psoriasis of the Nail
The nail lesions seen in psoriasis in the descending order of occurrence are as follows:7
- Nail Pitting
- Onycholysis
- Subungual hyperkeratosis
- Nail plate dystrophies
- Splinter hemorrhages
Pitting
Pits are superficial depressions within the nail plate. A pit in psoriasis indicates the former presence, in the proximal nail matrix, of clusters of parakeratotic cells as a result of the dyskeratinisation of psoriasis. As the nail grows outwards these parakeratotic cells slough off leaving a pit. Besides the nail matrix, the proximal nail fold (ventral surface) may also contribute to the process. The extent of the pit suggests the length of time the matrix is affected by psoriasis. The depth of the pit indicates the coinvolvement of the intermediate and ventral nail matrix.
If psoriatic lesions appear only on the intermediate and ventral matrix, a whitish appearance of the nail plate is seen instead of a pit. If psoriasis affects a wide area of the matrix, then transverse grooves appear on the nail surface as a manifestation of continuous pits (Figure 8.1).
Discoloration, Onycholysis
“Oil drops”– salmon colored spots on the nail indicate nail bed psoriasis. Parakeratotic process in the hyponychium results in onycholysis. The whitish color change seen on the nail plate in onycholysis occurs as a result of air entering the abnormal space between the nail plate and nail bed formed following exfoliation (Figure 8.2).7
Subungual Hyperkeratosis
This arises as a result of accumulation of parakeratotic cells under the nail plate. The origin of these cells is psoriatic activity in the hyponychium. Although subungual hyperkeratosis is seen in other diseases such as eczema and onychomycosis, the appearance of the scales can be a differentiating factor. Whereas in psoriasis it is likely to be silvery white, in the other diseases a yellow greasy appearance is evident probably as a result of a stronger inflammatory response and subsequent accumulation of a protein-containing exudate (Figure 8.3).



Thus in psoriasis both onycholysis and subungual hyperkeratosis are indicative of involvement of the same structure ie. the hyponychium. If the degree of psoriatic activity is severe, there is faster desquamation, then onycholysis is the picture, whereas if the activity is moderate and the parakeratotic cells are “retained”, then subungual hyperkeratosis is the effect.
Onychodystrophies
Beau's lines or transverse grooves may occur in nail psoriasis. These indicate “intermittent” psoriatic activity in the proximal nail fold areas. If severe damage is continuous or prolonged, then a state of onychorrhexis is evidenced, where the presenting features are longitudinal ridges and splits in the nail plate. Leukonychia represents deeper involvement of the nail matrix ie. of the intermittent and the ventral areas. If all the above dystrophies are seen together, it suggests the involvement of all parts of the nail plate8 (Figure 8.4).8
Splinter Hemorrhages
An uncommon manifestation, these indicate rupture of the nail bed dermal capillaries. As anatomically, these capillaries follow the longitudinal ridges of the rete pegs, their rupture is seen as linear “splinter” like hemorrhages. The commonest cause is trauma to the nail structure.94

Assessment and Management of Nail Psoriasis
Currently, the most comprehensive assessment of nail disease in psoriasis is the nail psoriasis severity index (NAPSI). However, this has to be evaluated in conjunction with a quality of life assessment such as the Dermatology life quality index (DLQI). These two parameters can therefore also be used to determine the efficacy of therapeutic measures. According to NAPSI, each nail is divided into four quadrants. Separate assessment is made of nail plate and nail matrix involvement, each with a score of 0–4 (0 – means no disease) for presence of pitting, leukonychia, nail plate dystrophy (nail matrix disease), oil drop sign, onycholysis, subungual hyperkeratosis, splinter hemorrhages (nail bed disease). If any sign is present in all 4 quadrants, the nail is given a score of 4 through to a score of 0 if there are no signs in any quadrant.
Current Treatment Options for Nail Psoriasis
The usefulness of existing treatments is handicapped by the difficulty in drug delivery to the site of inflammation as well as limited efficacy. Nail involvement is often refractory, slow healing, necessitating long periods of topical application and therefore low compliance. Due to these limitations, a standardized therapeutic regimen does not currently exist.
Topical Therapy
Corticosteroids and Vitamin D3 Analogs
Topical glucocorticoids and vitamin D3 analogs such as calcipotriol have been shown to be effective in improving the signs and symptoms of nail psoriasis. For nail matrix lesions, nail fold area application is effective, but for nail bed lesions the onycholytic nail needs to be trimmed back to the hyponychium (before applying treatment) as close as possible to the nail bed.9
Comparative studies have shown twice daily application of calcipotriol ointment to be as effective as twice daily betamethasone dipropionate in reducing subungual hyperkeratosis after 953–9 months in 58 patients with nail bed psoriasis.10 Further, it was found that a combination of calcipotriol ointment once daily for 5 days each week, followed by clobetasol propionate once daily for the other 2 days each week for 6 months followed by clobetasol alone for 6 further months showed between 70–80% improvement in nail disease.
Limitations
Adverse effects of long-term topical steroids – Skin atrophy and tapering of digit.
Steroid Injections
Triamcinolone acetonide (2.5%–10%) is injected with an insulin needle. The site depends upon the apparent origin of the nail dystrophy, usually given symmetrically pointing towards the midline of the nail. For matrix lesions (pitting of the surface, ridging and nail thickening/atrophy) the site of the injection is the middle and lateral proximal nail fold in the mid-thickness of the structure (may not require anesthesia). For nail bed lesions (onycholysis and subungual hyperkeratosis) access is via the lateral nail folds; the plane of injection being between the nail plate and the distal phalanx. Local anesthesia (ring block) is a must.
How often to inject? 2.5% concentration once in 3 months – for prolonged periods with careful scrutiny for atrophy (usually short term). 10% concentration – single injection can give benefits sustained for atleast 9 months.
Other Topicals
One percent 5 FU in propylene glycol or in 20% urea cream has been found useful in the case of nail pitting and nail thickening. However, it can dramatically exacerbate onycholysis. 0.1% Tazarotene gel applied with or without occlusion for 24 weeks showed significant improvement of almost all types of nail involvement including pitting.11 Topical cyclosporine, although difficult to make into a topical preparation (10% oily solution), has shown considerable improvement in isolated cases. However, further studies are needed. Anthralin – (0.4–2.0%) as a short contact therapy (30 minutes) showed “fair” results in a study conducted for 5 months. Staining of the nail was a minor side effect. Anthralin was found effective only in nail bed and hyponychial disease. Future research might include studies on tacrolimus and pimecrolimus, as also on rotational topical therapies.
Radiation Therapies
Several small studies have shown that local PUVA can benefit nail psoriasis.12 Superficial radiotherapy, electron-beam therapy as well as Grenz rays have been found to be of temporary benefit.
Systemic Therapies
Systemic therapy is seldom given for nail disease alone, but may be needed where there is pain or where the normal functions are jeopardized. However, there is presently very little evidence to prove their efficacy in improving nail disease. The commonly used systemic agents such as methotrexate, mycophenolate mofetil, hydroxyurea, 6-thioguanine and azathioprine have not been assessed for nail response.96
Acetretin has been used in the treatment of moderate to severe psoriasis with nail involvement. In a 10-week trial of skin, nail as well as joint psoriasis with cyclosporine 3.0 mg/kg/day or acetretin 0.52 mg/kg/day significant improvement from the baseline was seen.13 Low doses of acetretin 0.2 to 0.3mg/kg/day have also been found to result in good response. It is important to note that while acetretin is remarkably effective in thickened nail plate and subungual hyperkeratosis, it tends to cause normal thickness nails to become pathologically thin and ‘white’ during the treatment period.14
Combination Therapy
Use of more than one treatment modality may act by inhibiting more than one pathway of the disease and thus may show a better outcome. While treatment of cutaneous psoriasis with combination therapy has been widely studied and thus accepted, there is a lack of evidence with respect to nail disease.
In a single blinded study by Feliciani C et al,15 topical calcipotriol cream (50 μ/kg twice daily) along with oral cyclosporine (3.5–4.5 mg/kg/day) showed improvement in nail psoriasis in 79% compared to 48% receiving cyclosporine alone.
Biologic Therapy
Recently systemic therapy with biologics targeted against TNFα has been investigated in nail and joint psoriasis; however the trials need substantiation.
The drugs tried have been infliximab, etanercept, adalimumab, efalizumab and alefacept. Among these, currently, infliximab has the best evidence for efficacy of TNFα antagonist in nail disease.
In the well-controlled EXPRESS trial [European infliximab for psoriasis (Remicade) efficacy and safety study]16 a phase III multicenter, double blind, placebo controlled trial to evaluate long-term efficacy and safety of infliximab in psoriasis, there was complete clearance of nail disease in 44.7% of patients after 50 weeks. All forms of nail psoriasis showed improvement, most in lunula red spots and pitting, and least in nail crumbling.
Surgical Therapy
Surgical modalities are indicated for painful digits, usually toes, as a result of nail thickening and distortion. Also toe nails respond less to topical and intra lesional therapy. Nail avulsion by itself is not usually recommended, however avulsion followed by phenolic ablation of the nail matrix can provide permanent cure.
Regular podiatric methods to trim the nail can be effective. A useful modality for nail dystrophy is nail dissolution with 40% urea paste under occlusion for 4 to 6 weeks.
Pustular Psoriasis Localized to the Nail Unit and its Treatment
Isolated nail involvement with pustular psoriasis is seen in the form of Acrodermatits of Hallopeau with recurrent, sometimes painful, coalescing pustules around the distal digit. Usually a single digit is involved. Pustules form under the nail plate and periungual area. Other symptoms include onycholysis, onychomadesis and scaling of the nail bed and periungual skin. 97

A close differential diagnosis would be herpetic paronychia. Direct fluorescent antibody assay, viral cultures or PCR may be required for definitive distinction.17 The nails may also be involved as part of generalized pustular psoriasis. It is important to rule out infection (Figure 8.5).
The main topical therapy for pustular psoriasis of the nail unit is calcipotriol. Its benefit is seen in combination with betamethasone di propionate. Long-term benefit can be expected with Calcipotriol alone. Super potent topical corticosteroids can give good relief in the short-term. The place of biologics in standalone nail pustular psoriasis in not evidenced at present.
Conclusions and Future Trends
Nail involvement is highly prevalent in psoriasis and psoriatic arthritis and may be predictive of a more severe disease, indicative of a link between the skin disease and the joint involvement. Current topical, intralesional, systemic and phototherapies are relatively ineffective, difficult to administer and have adverse effects that can limit their long-term usefulness.
In future, intralesional injections of drugs other than corticosteroids, such as calcipotriol, methotrexate or even biologic drugs may be the trend. Nail focused therapies would include localized NBUVB, excimer laser and photodynamic therapy. By utilizing combination therapy, it will be possible to inhibit more than one pathway of the disease with better results.
References
- Samman PD, Fenton DA. The nails in disease, 5th ed. London: Butterworth-Heinemann Ltd., 1994.
- Lawry M. Biological therapy and nail psoriasis. Dermatol Ther 2007; 20: 60–67.
- de Jong EM, Seegers BA, Gulinck MK et al. Psoriasis of the nails associated with disability in a large number of patients: results of a recent interview with 1,728 patients. Dermatology 1996; 193: 300–303.
- McGonagle D, Tan AL, Benjamin M. The nail as a musculoskeletal appendage- implications for an improved understanding of the link between psoriasis and arthritis. Dermatology 2009; 218: 97–102.
- Zaias N. The embryology of the human nail. Arch Dermatol 1963; 87: 37–53.
- Zaias N. The nail in health and disease, 2nd ed. Norwalk: Appleton & Lange; 1990.
- Baran R, Dawber RPR. Diseases of the nail and their management. In: Baran R, Dawber RPR, editors. Oxford: Blackwell Science; 1984.
- Jiaravuthisan MM, Sasseville D, Vendor RB et al. Psoriasis of the nail: anatomy, pathology, clinical presentation and a review of literature on therapy. J Am Acad Deramtol 2007; 57: 1–27.
- Tosti A, Piraccini BM, Cameli N, Kokely F, Plozzer C, Cannata GE, et al. Calcipotriol ointment in nail psoriasis; a controlled double-blind comparision with betamethasone dipropionate and salicylic acid. Br J Dermatol 1998; 139: 655–9.
- Scher RK, Stiller M, Zhu Yi: Tazarotene 0.1% gel in the treatment of fingernail psoriasis; A double-blind, randomized, vehicle-controlled study. Cutis 68: 355-358, 2001.
- Dobson R, Thiers B. Year book of Dermatology Chicago, Year book Medical Publishers Inc. 1981, pp288.
- Mahrle G, Schulze HJ, Farber L, et al: Low-dose short-term cyclosporine versus etretinate in psoriasis; Improvement of skin, nail and joint involvement. J Am Acad Dermatol 32: 78-88, 1995.
- Baran R: Retinoids and the nails. J Dermatol Treat 1: 151-154, 1990.
- Feliciani C, Zampetti A, Forleo P, et al: Nail psoriasis: Combined therapy with systemic cyclosporine and topical calcipotriol. J Cutan Med Surg 2004; 8: 122–125.
- Reich K, Nestle FO, Papp K, et al: Infliximab induction and maintenance therapy for moderate-to-severe psoriasis: A phase III, multicentre, double-blind trial: Lancet 2005; 366: 1367–1374.
- Piraccini BM, Tosti A, Lorizzo M, et al: Pustular psoriasis of the nails. Treatment and long-term follow-up of 46 patients. Br J Dermatol 144: 1000-1005, 2001.
Synonym: Sand Paper Nails, Rough Nails
Definition: Trachyonychia literally means “rough” nails. Nails that are rough, opaque, thin with superficial ridging and with or without pitting and ragged cuticle qualify as trachyonychia (Figures 9.1 and 9.2). Koilonychia may be an accompanying feature.
Introduction
Trachyonychia or rough nails, presents both as an idiopathic disorder of the nails or secondary to few known dermatological diseases. Trachyonychia is derived from the Greek word trakos, (meaning rough) and denotes the prominent rough nail changes.1 Simultaneous involvement of either one nail or several nails can be observed. The term “twenty nail dystrophy” (TND) is specifically used to describe trachyonychia involving all 20 nails.2 These nails are noted with diffuse ridging, are lusterless, and in severe cases presents with sandpaper-like surface.
Alkiewicz in 1950 was the first to describe it and later it was termed as twenty-nail dystrophy of childhood in 1977 by Hazelrigg.3 It is much more common in children, with gradual onset and 100peaks during the ages between 3 to 12 years.


However, it can occur at any age. Trachyonychia can be a manifestation of a pleomorphic group of disorders or can be idiopathic. Trachyonychia has also been reported to be transmitted in an autosomal dominant fashion in few families .4
Classification
- Idiopathic Trachyonychia
- Secondary Trachyonychia
Idiopathic Trachyonychia
Trachyonychia may present as an idiopathic disorder of the nails with no other cutaneous or systemic findings or it can be caused by a variety of other disorders. Idiopathic trachyonychia far outnumbers secondary trachyonychia. It is also much more common than it is traditionally 101reported in the literature.2 The findings seen in idiopathic trachyonychia are brittle, thin nails, with excessive longitudinal ridging. This gives the nail plate a rough, opaque, and dull appearance. The cuticle is usually hyperkeratotic and ragged.
Depending on the severity, it is possible to distinguish two clinical varieties of trachyonychia:
- A severe type, characterized by opaque, sandpaper nails.
- Mild types characterized by shiny nails with superficial ridging and diffuse pitting. Koilonychia can be seen in both types.
Secondary Trachyonychia
Secondary Trachyonychia has been reported in association with several diseases. Its association with dermatological diseases such as alopecia areata,5 vitiligo,6 lichen planus,7 psoriasis8 and atopic dermatitis has been documented. Rare association with ichthyosis vulgaris9 and incontinentia pigmenti has been described.10
Alopecia areata (AA) is the most common disease in patients with trachyonychia, and affects 1–2% of the population worldwide, with a typical onset during childhood or adolescence. Trachyonychia has a prevalence of 3.65% in this patient population. However, severe forms of trachyonychia are noted secondary to lichen planus.5
Trachyonychia is seen in 10% of patients affected by nail lichen planus (LP). In these patients, nail LP is most often isolated. However, oral LP is the most common type of LP associated with nail LP. It has been suggested that the form of LP presenting as trachyonychia may be a separate entity as it tends to occur independent of the typical findings of nail LP such as thinning, splitting or nail atrophy. In fact, pterygium formation and scarring is rare in patients with trachyonychia caused by LP, and in general it portends a benign course, sometimes with spontaneous resolution.7
Trachyonychia in the setting of psoriasis has more thickening of the nail plate as opposed to the thinning noted in lichen planus. Similar to the cutaneous lesions of psoriasis, the Koebner phenomenon can worsen the disease.8
It is important to note that the diseases chronically involving the nail folds can also lead to trachyonychia.
Histopathology
Trachyonychia is a disease of the nail matrix, thus a pathological diagnosis requires a nail matrix punch or a longitudinal nail biopsy (LNB).11 However, the pathological diagnosis of trachyonychia is not really required as the disease has a benign outcome, even when caused by lichen planus. The most common histopathological feature associated with trachyonychia is spongiosis and exocytosis of the inflammatory cells into the nail epithelia. This is seen in trachyonychia associated with alopecia areata and in most cases of idiopathic trachyonychia. Patients with psoriasis and trachyonychia demonstrate similar pathologic changes as in the skin, with acanthosis, focal parakeratosis, and the accumulation of polymorphonuclear cells along the dorsal nail plate.
Differential Diagnosis
The most frequent differential diagnoses to consider are brittle nails, senile nails, alopecia areata, psoriasis, and lichen planus.8 Brittle nails show longitudinal and superficial splitting but 102not excessive ridging and roughness. Senile nails show mild longitudinal ridging and beading but these abnormalities are not diffuse involving the entire nail plate. Geometric pitting due to alopecia areata is very similar to shiny trachyonychia.
Treatment
Treatment of trachyonychia is mainly cosmetic as it is not a permanently scarring condition. In children with TND, a tendency towards spontaneous resolution is seen. One study had determined the rate of complete regression of patients diagnosed with trachyonychia regardless of treatment to be almost 50%. Of the twelve patients followed up in this study, two patients presented with alopecia areata, two others presented with psoriasis, and eight patients did not present with or develop accompanying skin or mucosal disease. Spontaneous resolution may also be seen in patients with trachyonychia associated with alopecia areata. Hence, caution should be exercised before embarking on any aggressive therapy in children. An attempt should always be made to establish the diagnosis before therapy
Tazarotene gel 0.1%, a topical retinoid used to treat chronic plaque psoriasis and acne, helped to improve trachyonychia in one patient with alopecia areata after daily use for three months.12 Topical chemotherapeutics have also been used with some success in psoriatic trachyonychia. In a case report of one psoriatic patient, topical 5-fluorouracil (5% cream) was used in short interval applications (20 minutes) from every other day to every fourth day with weekly maintenance with good clinical improvement. Periungual irritation is very common complication.
Psoralen plus ultraviolet A (PUVA) has been effective in one patient with TND who was treated for seven months at a dosage of 0.7/1.4 J/cm2 three times per week for 7 months. Of particular note is the fact that the untreated toenails remained dystrophic.13
Intralesional injection of triamcinolone into the proximal nail fold at a concentration of 2.5–10 mg/ML has been shown to be effective. Patient compliance with treatment continuation is poor secondary to procedure associated pain.14 Successful combination would be intra-matrix steroids administered under general anesthesia with ketamine and oral griseofulvin for six months. Griseofulvin is believed to play an anti-inflammatory role in patients with trachyonychia associated with lichen planus and is best paired with intra-matrix steroids.15
Systemic retinoids are another treatment option for trachyonychia and both acitretin and etretinate have been reported as being useful. The use of acitretin for this condition has also been reported at a higher dosage of 0.5 mg/kg. Possible side effects of systemic retinoids include nail-fragility, paronychia, or multiple periungual pyogenic granulomas.16
More aggressive therapy in the form of cyclosporine A has also been used. In one French study involving patients with psoriasis and trachyonychia, five psoriatic patients were treated with cyclosporine at a dose of 3 mg/kg/day. These patients were evaluated using optical profilometry to assess the “roughness” of the nails. Improvement of nail lesions was seen after two to three months of therapy and it lagged behind the cutaneous lesions.17
Vitamin supplementation of biotin at 20 mg/day has been successful in treating trachyonychia in two patients with primary biliary cirrhosis. Other reported systemic treatments include oral prednisolone (40 mg daily reduced to 30 mg daily after 2 weeks) with symptomatic improvement after 4 weeks of treatment and antimalarials (chloroquine phosphate at 250 mg twice daily) in 1 patient, with recurrence in 10 weeks after discontinuation of the antimalarials treatment. One successful treatment for a child with trachyonychia included systemic corticosteroids. This was 103achieved with an oral mini-pulse therapy of betamethasone as a single oral dose with breakfast on two consecutive days every week for two months.18
The various treatment modalities for trachyonychia often target the underlying disorder, such as AA, LP or psoriasis. It is important to note that trachyonychia may be self-limiting in many cases and as such, treatments should only be given when deemed essential. Furthermore, injections into the nail matrix should rarely be considered.
Conclusion
Trachyonychia is a chronic clinical condition that may present as an idiopathic finding or in association with many conditions, especially alopecia areata, psoriasis, and lichen planus. Determining the cause of trachyonychia is challenging. While the histopathological findings have been well documented, the diagnosis of trachyonychia can most often be made based on the associated distinguishing clinical presentations. Treatment is often unsatisfactory, although in general it should be aimed at the underlying cause. The most effective therapy for trachyonychia has not yet been universally accepted, but in most cases the nail signs improve spontaneously and treatment may be necessary in few individuals.19
Reference
- Scheinfeld NS. Trachyonychia: A case report and review of manifestations, associations, and treatments. Cutis 2003; 71:299–302.
- Tosti A, Bardazzi F, Piraccini BM, Fanti PA. Idiopathic trachyonychia (twenty-nail dystrophy): A pathological study of 23 patients. Br J Dermatol 1994; 131:866–72.
- Hazelrigg DE, Duncan WC, Jarratt M. Twenty-nail dystrophy of childhood. Arch Dermatol 1977; 113:73–5.
- Pavone L, Li Volti S, Guarneri B, La Rosa M, Sorge G, Incorpora G, Mollica F. Hereditary twenty-nail dystrophy in a Sicilian family. J Med Genet 1982;19:337–40.
- Tosti A, Fanti PA, Morelli R, Bardazzi F. Trachyonychia associated with alopecia areata: A clinical and pathologic study. J Am Acad Dermatol 1991;25:266–70.
- Peloro TM, Pride HB. Twenty-nail dystrophy and vitiligo: A rare association. J Am Acad Dermatol 1999;40:488–90.
- Scher RK, Fischbein R, Ackerman AB. Twenty-nail dystrophy: A variant of lichen planus. Arch Dermatol 1978; 114:612–3.
- Sehgal VN. Twenty-nail dystrophy trachyonychia: An overview. J Dermatol 2007;34:361–6.
- James WD, Odom RB, Horn RT. Twenty-nail dystrophy and ichthyosis vulgaris. Arch Dermatol 1981; 117:316.
- Scardamaglia L, Howard A, Sinclair R. Twenty-nail dystrophy in a girl with incontinentia pigmenti. Australas J Dermatol 2003; 44:71–3.
- Jerasutus S, Suvanprakorn P, Kitchawengkul O. Twenty-nail dystrophy: A clinical manifestation of spongiotic inflammation of the nail matrix. Arch Dermatol 1990; 126:1068–70.
- Soda R, Diluvio L, Bianchi L, Chimenti S. Treatment of trachyonychia with tazarotene. Clin Exp Dermatol 2005; 30:301–2.
- Halkier-Sorensen L, Cramers M, Kragballe K. Twenty-nail dystrophy treated with topical PUVA. Acta Derm Venereol 1990; 70:510–1.
- Khoo BP, Giam YC. A pilot study on the role of intralesional triamcinolone acetonide in the treatment of pitted nails in children. Singapore Med J 2000; 41:66–8.
- Sehgal VN, Abraham GJ, Malik GB. Griseofulvin therapy in lichen planus: A double-blind controlled trial. Br J Dermatol 1972; 87:383–5.
- Brazzelli V, Martinoli S, Prestinari F, Borroni G. An impressive therapeutic result of nail psoriasis to acitretin. J Eur Acad Dermatol Venereol 2004; 18:229–30.
- Pierard GE, Pierard-Franchimont C. Dynamics of psoriatic trachyonychia during low-dose cyclosporin A treatment: A pilot study on onychochronobiology using optical profilometry. Dermatology 1996; 192:116–9.
- Mittal R, Khaitan BK, Sirka CS. Trachyonychia treated with oral mini pulse therapy. Indian J Dermatol Venereol Leprol 2001; 67:202–3.
- Trachyonychia: A comprehensive review: Katherine A Gordon, Janelle M Vega, Antonella Tosti; Ind J of Dermatol Venereal Leprol, 2011, Vol 77: Issue 6; P. 640 – 645.
Nail Changes in Alopecia Areata
Cutaneous Lesions
Alopecia areata is a chronic inflammatory disease involving the hair follicles. Clinically it manifests as patchy nonscarring alopecia which may be unifocal, multifocal, total, universal or in an ophiasis pattern. Apart from hair, it can also involve other structures like eyes and nails, particularly in children.1
Nail Changes
The incidence of nail changes in alopecia areata ranges from 7% to 66%.2 These nail changes can either precede, accompany or follow the hair changes and these changes may persist for long time even after the hair changes subside but most of them heal spontaneously. Many studies have shown that the involvement of nails is directly proportional to the severity of the disease.3,4 So the involvement of nails in alopecia areata can be considered as an important prognostic indicator of disease severity.2106
The various nail changes observed include diffuse fine pitting, onychorrhexis, Beau's lines, koilonychia,5 longitudinal ridging, leukonychia punctata,6 onychodystrophy, onycomadesis and trachyonychia.7
Pits in alopecia areata are usually small, superficial and regularly distributed in geometric pattern (Figure 10.1) (Scotch plaid pattern/Tartan pattern8/glen plaid design9) as against the large, deep irregularly placed pits of psoriasis. The finding of shallow pits lined with residual adherent parakeratotic cells suggests that the pathogenesis of nail pits in alopecia areata is similar to that of psoriasis; a result of shedding of parakeratotic cell aggregates from the nail plate.6 Spotted lunula or red lunula has been described in association with severe alopecia areata.10 The spotted lunula is ascribed to defects in the tongue of matrical epithelium which lies under the nail plate and accounts for the lunula. An analogy is drawn with Wickham's striae.11
Trachyonychia though described in alopecia areata is not exclusive to alopecia areata, as it is reported in other dermatological conditions like lichen planus, psoriasis,eczema and pemphigus vulgaris. The affected nails are roughened and opaque with excessive longitudinal striations.
Histopathology
Distinctive pathologic features of mild to moderately dense lymphocytic infiltrate associated with exocytosis and spongiosis characterize trachyonychia as well as the other nail abnormalities caused by alopecia areata.12
Differential Diagnosis
- Pitting—psoriasis, Reiter's disease, eczema, contact dermatitis, lichen planus.
- Trachyonychia—lichen planus, psoriasis, eczema and pemphigus vulgaris.
- Red lunula13—rheumatoid arthritis, systemic lupus erythematosus, cardiac failure, hepatic cirrhosis, lymphogranuloma venereum, psoriasis, carbon monoxide poisoning, twenty-nail dystrophy, and reticulosarcoma.

Treatment
- Nail changes of alopecia areata resolve spontaneously once the hair signs resolve.
- Intralesional corticosteroids have been tried which give temporary benefit.
- Oral corticosteroids though beneficial, their use is restricted because of the need for long-term therapy and its associated complications.
- Contact sensitizers like dinitrochlorobenzene or squaric acid dibutyl ester used for alopecia also have shown to improve nail abnormalities.
Nail Changes in Eczema and Contact Dermatitis
Eczematous dermatitis may produce a wide variety of nail changes. An incidence of 20%14 is reported in a study conducted by Neera Puri et al on nail changes in various dermatoses. As the insult is from outside it primarily affects the nail plate and nail folds though matrix inflammation can occur in long standing cases as a secondary phenomenon from adjacent paronychia.
Atopic dermatitis is the most common eczema affecting the nails because of its high prevalence and chronicity.10 Nail involvement can also occur as a part of contact dermatitis. The common allergens, such as nickel, fragrance, rubber, chromate and medicaments, rarely have particular bearing on nail abnormalities. Selective exposure to such allergens or strong irritants is as important as chronic low-grade irritation from milder agents, such as water, seen in catering workers. The most common allergens are found in nail cosmetics such as enamel, sculptured nails, and preformed plastic tips are toluene, sulfonamide, formaldehyde resin, acrylates, and ethylcyanoacrylate.15
Clinical Features
Patients may have a genetic tendency for atopic eczema and/or pompholyx. The onset of nail changes may be at any age. Usually patients have a history of long-standing eczema especially of hands and feet. The nail changes include roughness, thickening, coarse and irregular plate pitting or grooving, transverse ridging, furrowing, nail shedding, onycholysis and subungual hemorrhages (Figures 10.2 to 10.4) Acute or chronic paronychial inflammation which affects nail matrix secondarily may lead to nail plate dystrophy. Smooth shiny or polished nails can be seen because of constant skin rubbing. In long standing dyshidrotic eczema, dystrophic nail changes may develop.
Various allergens and irritants can produce nail unit abnormalities. For example, organic solvents and motor oils can produce koilonychia.16 Reactions to artificial nails have included paronychia, onychodystrophies, and dermatitis at contact areas and at sites distant to the contactant. Erythema and painful pruritic vesicles of the paronychial tissue several hours after the application of sculptured nails have been reported.17 Cyanoacrylates used in prosthetic nails can provoke local and distant allergic reactions. Formaldehyde, occasionally used as a nail hardener, can provoke painful onycholysis if the patient becomes sensitized, or sometimes when acting solely as an irritant. Some allergens may cause nail dystrophy without associated inflammation. A combination of atopy and an exogenous irritant or allergic contact reaction is common.18 The resultant inflammation can involve the matrix, bed, plate, hyponychium and nail folds manifesting as brittle nails, subungual hyperkeratosis, onycolysis, splinter hemorrhages, chromonychia, paronychia, nail dystrophy.108



Differential Diagnosis
Onychomycosis, paronychia, psoriasis
Diagnosis
Diagnosis is mainly on clinical grounds. Eczematous lesions elsewhere in the skin clinches the diagnosis. Mycological examinations can be done in doubtful cases to rule out onycomycosis. Along with a proper clinical history focusing on nail practices, a thorough understanding of the common allergens and patch testing are necessary to diagnose contact dermatitis.
Management
- Advise patients to avoid further use of any possible aggravating factors.
- Protect hands with cotton-lined rubber gloves when in water.
- Advise frequent use of emollients.
- Topical steroids - a potent one may be necessary for the hands and feet.
- Tacrolimus or pimecrolimus, azathioprine, methotrexate or ciclosporin, phototherapy have been tried.
- If the eczema improves, nails will usually return to normal.
Scabies
Scabies is an ectoparasitic infestation caused by the mite Sarcoptes scabei var hominis primarily affecting the skin. Nail unit is not affected routinely in scabies, but mite can get lodged subungually due to scratching the burrows and cause reinfection.
Crusted or Norwegian scabies: The lesions of the Norwegian scabies have a predilection for areas of pressure and are strikingly different from those of ordinary scabies. The characteristic of this condition is the existence of dystrophic nails which are hyperkeratotic and accompanied by large, psoriasis-like accumulations of scales under the nails. Even after successful treatment of the hyperkeratotic lesions on the skin, the dystrophic nails persist. The mites survive in the subungual material and are a source of reinfestation.19 Complete destruction of the nail plate can occur as the plate becomes infested.
Differential Diagnosis
Psoriasis
Diagnosis
Diagnosis is confirmed by microscopic examination of material scraped from the lesion and from beneath the nails.
Treatment
- Proper scabicidal application and trimming back of nail plates.
- Manual removal of the subungual debris and brushing of finger tips under the free edges of the nail along with application of scabicidal agents.20110
- A combination of chemical reduction of the nail plate with topical 40% urea, partial nail avulsion and topical lindane lotion under occlusion has been effectively tried in a patient.21
Bullous Disorders
Nail involvement can occur in blistering disorders like immunobullous and mechanobullous diseases. Nail changes of mechanobullous disorders have been described elsewhere in the text.
Pathogenesis
Many studies of the basement membrane zone of the nail have shown that the antigenic expressions in the basement membrane zone of proximal nail fold, nail bed, matrix and hyponychium is similar to the normal skin.22,23 Immune reactants produced against skin basement membrane zone react with antigens of the nail unit. It remains unclear which factors determine the location of pemphigus lesions, but it may correlate with a different distribution pattern of pemphigus vulgaris (PV) antigen. It is possible that the nail bed may represent a distinctive antigenic target region for the circulating auto-antibodies.24
|


Diagnosis
- Biopsy of the nail matrix and nail bed for histopathology which shows the level of split.
- Direct immunofluorescence to detect immune reactants.
Treatment
- Treatment of secondary infections.
- Treatment of cutaneous and mucosal lesions with steroids and other immunosuppressives will improve nail abnormalities.35
Pityriasis Rubra Pilaris (PRP)
Pityriasis rubra pilaris (PRP) is a rare disorder that have in common circumscribed follicular keratoses, branny scale and an orange-red erythema, and palmoplantar keratoderma. Various types from 1 to V1 have been reported.
Nail changes are associated with Type 1 adult onset PRP, more commonly when palms and soles are affected. The nails are thickened and discolored distally, showing splinter haemorrhages. Nail dystrophy is less common in juvenile type V PRP. Onychogryphosis has been reported in juvenile type V PRP. Psoriasiform pitting can occur in circumscribed type 1V PRP. Wedge-shaped thickening has been reported in type V1 PRP associated with HIV.35
Differential Diagnosis
Psoriasis distal yellow-brown discoloration, subungual hyperkeratosis, nail plate thickening, and splinter hemorrhages indicate a diagnosis of type 1 pityriasis rubra pilaris rather than psoriasis, whereas onycholysis (particularly marginal), salmon patches, small pits, and larger indentations of the nail plate indicate a diagnosis of psoriasis.36
Histopathology35
Nail bed epithelium shows parakeratotic areas, acanthosis and focal basal liquefaction. Keratohyaline may be present. In dermis there is mononuclear inflammatory infiltrate. The hyponychium shows both orthokeratosis and parakeratosis.
Treatment35
- Retinoids, particularly etretinate has been used successfully.
- Combination of retinoid and PUVA can be tried.
- Infliximab has also been tried.
Paraneoplastic Acrokeratosis (Bazex Syndrome)
This is a rare condition, much commoner in males than females, which is associated particularly with squamous cell carcinoma of the upper respiratory or gastrointestinal tracts. Cutaneous features are predominantly acral in distribution with papulosquamous lesions, hyperpigmentation and keratoderma.
Nail changes include paronychia, nail dystrophy, onycholysis, irregular nail plate, subungual hyperkeratosis, erythema and tenderness of nail folds.
Diagnosis
Treatment
- It does not respond to any topical therapy.
- Treatment of underlying malignancy will improve the nail changes.
Darier's Disease
Darier's disease is an autosomal dominant condition characterized by a persistent eruption of hyperkeratotic papules, histological examination of which shows suprabasal acantholysis with a distinctive overlying dyskeratosis.
Nail Changes
Keratotic papules can be seen on proximal nail fold. Nail changes show short and wide nails, white and red longitudinal bands, V-shaped notch, scalloping of distal nail plate and subungual hyperkeratosis.37 A sandwich of red and white longitudinal bands, often with a V-shaped nick at the free margin of the nail, (Figure 10.7) is the most pathognomonic nail finding in patients with Darier's disease.38 A study conducted by Neera Puri has shown that the alternating red and white bands were seen in all the patients (100%) and V-shaped nicking at the free margins of nails was seen in 93.3% patients.39
Histopathology
Involvement of matrix results in parakeratotic cells which gets incorporated into nail plates resulting in longitudinal streaks. Multinucleated keratinocytes are also seen. Nail bed shows hyperplastic epithelium which may be 10–30 cell thick. Nail bed may also show multinucleated keratinocytes. Vasodilation responsible for red streaks may be seen in nail bed.
Differential Diagnosis
- Hailey-Hailey disease – though longitudinal bands are seen, typical sandwich of white and red lines is not seen here.
- Periungual warty papules has to be differentiated from Acrokeratosis verruciformis of Hopf.

Treatment
- Oral retinoids used for cutaneous lesions have no effect on nail changes.
- Surgical methods with skin grafts have been tried in dystrophic nails.41
Reiter's Syndrome
- Reiter's syndrome is a reactive dermatosis with a triad of arthritis, urethritis and conjunctivitis.
- Cutaneous changes include circinate balanitis and keratoderma blennorhagica.
Nail Changes
Nail involvement is noted in 20–30 percent.41 Finger nails are affected more than the toe nails. Nail involvement may be associated with keratoderma blennorrhagica or may occur as a separate entity. Early changes consist of a red, rolled edge of the nail fold. Subungual corny material accumulates and lifts the nail plate, which becomes yellow, opaque, ridged, and thickened. The nail is brittle and may eventually shed. The nail bed may show papular keratinized excrescences. The nail changes may persist indefinitely or clear. Occasionally inflammatory areas in the skin adjacent to the subungual keratotic material may be mistaken for paronychia. The yellowish waxy hyperkeratotic substance that accumulates under the distal end of the nail plate may discharge at intervals.42 Occurrence of Terry's nail43 and nail pitting44 has also been reported.
Histopathology
Similar to psoriasis.
Differential Diagnosis
Psoriasis
Treatment
- Resistant to treatment.
- Topical corticosteroids and NSAID's have been tried.
- In resistant cases methotrexate, retinoids and PUVA can be tried.
- Infliximab given for cutaneous lesions of Reiter's in an HIV patient has shown to improve nail changes.45
Apart from above mentioned dermatological conditions, there are various conditions that can involve nails. These conditions have been listed in Table 10.2.115
|
References
- Baran R, Tosti A. Nails. In: Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg IM, Austen FK, editors. Dermatology in general medicine, 4th edition New York: McGraw–Hill; 1993.p. 657-71.
- Gandhi V, Baruah MC, Bhattacharaya SN. Nail changes in alopecia areata: Incidence and pattern. Indian J Dermatol Venereol Leprol 2003;69:114–5.
- Sharma VK, Dawn G, Kumar B. Profile of alopecia areata in Northern India. Int J Dermatol 1996; 35: 22–27.
- Sharma VK, Kumar B, Dawn G. A clinical study of childhood alopecia areata in Chandigarh, India. Pediatr Dermatol 1996; 13: 372–377.
- Nicole C. Dombrowski, Wilma F. Bergfeld. Alopecia areata: What to expect from current treatments. Cleveland Clinic Journal of Medicine, Volume 72 Number 9, September 2005.
- Dotz WI, Lieber CD, Vogt PJ. Leukonychia punctata and pitted nails in alopecia areata. Arch Dermatol. 1985 Nov;121(11):1452–4.
- Tosti A, Morelli R, Bardazzi F, et al. Prevalence of nail abnormalities in children with alopecia areata. Pediatr Dermatol 1994; 112-115.
- Diseases of the skin appendages. James WD, Berger TG, Elston DM, editors. Andrews’ Diseases of the Skin Clinical Dermatology. 10th ed. Canada: Saunders Elsevier.
- Del Rosso JQ, Basuk PJ, Scher RK, Ricci AR. Dermatologic diseases of the nail unit. In; Scher, Daniel editors: Nails: Therapy. Diagnosis. Surgery. 2nd Edition. WB Sounders Company. Philadelphia 1997, p. 172-200.
- Bergner T, Donhauser G, Ruzicka T. Red lunulae in severe alopecia areata. Acta Derm Venereol. 1992;72(3):203–5.
- Shelley WB. The spotted lunula. A neglected nail sign associated with alopecia areata. J Am Acad Dermatol. 1980 May;2(5):385–7.
- Tosti A, Fanti PA, Morelli R, Bardazzi F. Trachyonychia associated with alopecia areata: a clinical and pathologic study. J Am Acad Dermatol. 1991 Aug;25(2 Pt 1):266–70.
- Wilkerson MG, Wilkin JK. Red lunulae revisited: a clinical and histopathologic examination. J Am Acad Dermatol. 1989 Mar;20(3):453–7.
- Neerja Puri, Tejinder Kaur. A study of nail changes in various dermatosis in punjab, india. Our Dermatol Online. 2012; 3(3): 164–170.
- Militello G. Contact and primary irritant dermatitis of the nail unit diagnosis and treatment. Dermatol Ther. 2007 Jan-Feb;20(1):47–53.
- Fisher AA. Contact dermatitis, ed 3. lea & Fibiger, Philadelphia, 1986.
- Mowad CM, Ferringer T. Allergic contact dermatitis from acrylates in artificial nails. Dermatitis. 2004 Mar;15(1):51–3.
- D.A.R. de Berker & R. Baran. Disorders of nails. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's Textbook of Dermatology, 8th edition Sussex: Wiley Blackwell; 2010.
- Bertrand Richert. Parasitic infections of the nails. Dermatology online Journal. Volume 9, number 1. Available from http://dermatology-s10.cdlib.org/91/abstracts/nail/17C.html.
- Scher RK. Subungual Scabies. Am J Dermatopathol 5:187,1983.
- De Paoli RT, Marks VJ. Crusted (Norwegian) scabies: treatment of nail involvement. J Am Acad Dermatol. 1987 Jul;17(1):136–9.
- Sinclair RD, Wojnarowska F, Leigh IM et al: The basement membrane zone of the nail. Br J Dermatol 131:499,1994.
- Cameli N, Picardo M, Pisani A:Charecterisation of nail matrix basement membrane zone:An immunohistochemical study of normal nails and of nails in Herlitz junctional epidermolysis bullosa. Br J Dermatol 134:182.1996.
- Zoi Apalla, George Chaidemenos, George Karakatsanis. Nail unit involvement during severe initial pemphigus vulgaris development. European Journal of Dermatology. Volume 19, Number 3, 290-1, May-June 2009, Correspondence.
- Habibi M, Mortazavi H, Shadianloo S, Balighi K, Ghodsi SZ, Daneshpazhooh M, Valikhani M, Ghassabian A, Pooli AH, Chams-Davatchi C. Nail changes in pemphigus vulgaris. Int J Dermatol. 2008 Nov;47(11):1141–4.
- Serratos BD, Rashid RM. Nail disease in pemphigus vulgaris. Dermatol Online J. 2009 Jul 15;15(7):2.
- Tosti A, André M, Murrell DF. Nail involvement in autoimmune bullous disorders. Dermatol Clin. 2011 Jul;29(3):511-3, xi. Epub 2011 May 6.
- Lee HE, Wong WR, Lee MC, Hong HS. Acute paronychia heralding the exacerbation of pemphigus vulgaris. Int J Clin Pract. 2004 Dec;58(12):1174–6.
- Schlesinger N, Katz M, Ingber A. Nail involvement in pemphigus vulgaris. Br J Dermatol. 2002 May;146(5):836–9.
- Parameswarw VR, Chinnappaiah Naik RP. Onychomadesis associated with pemphigus vulagaris. Arch Dermatol 117:759.1981.
- Azulay RD: Brazilian pemphigus foliaceus. Int J Dermatol 21:122, 1982.
- Baran and Dawber's Diseases of the Nails and their Management. Wiley's publications.
- Kirtschig G, Effendy I, Happle R. Leukonychia longitudinalis as the primary symptom of Hailey-Hailey disease. Hautarzt. 1992 Jul;43(7):451–2.
- Burge SM, Powell SM, Ryan TJ: Cicatricial pemphigoid with nail dystrophy.
- Cahali JB, Kakuda EY, Santi CG, Maruta CW. Nail manifestations in pemphigus vulgaris. Rev Hosp Clin Fac Med Sao Paulo. 2002 Sep-Oct;57(5):229–34.
- Sonnex TS, Dawber RP, Zachary CB, Millard PR, Griffiths AD. The nails in adult type 1 pityriasis rubra pilaris. A comparison with Sézary syndrome and psoriasis. J Am Acad Dermatol. 1986 Nov;15(5 Pt 1):956–60.
- Atiya Mahboob, Faryal Yaqub, Zahid Shahzad, Manaal Afzaal, Moazzum Hanif, Deeba Sattar Khan, Riffat Nasim, Aleena Khan. Classical presentation of darier's disease: A rare disorder of keratinization. J Ayub Med Coll Abbottabad 2010;22(3).
- Zaias N, Ackerman AB. The nail in Darier-White disease. Arch Dermatol 1973; 107: 193–9.
- Neerja Puri. A clinical and histopathological study of Darier's disease. Journal of Pakistan Association of Dermatologists 2011; 21 (4): 230-234.
- Baran R: An effective surgical treatment for nail thickening in Darier's disease. J Eur Acad Dermatol Venereol 19:689, 2005.
- Coskun BK, Saral Y, Ozturk P, Conskun N. Reiter syndrome accompanied by Terry nail. JEADV 20051987–9. PubMed
- Andrei Calin. Ann. rheum. Dis. (1979), 38, Supplement p. 68 Keratodermia blennorrhagica and mucocutaneous manifestations of Reiter's syndrome.
- Fariborz Zandieh and Mojgan Loghmani. Reiter's Syndrome in a Patient with Polyarthritis and Nail Involvement. Iran J Allergy Asthma Immunol September 2008; 7(3): 185–186.
- Lovy MR, Bluhm GB, Morales A. The occurrence of nail pitting in Reiter's syndrome. J Am Acad Dermatol. 1980 Jan;2(1):66–8.
- Norman Gaylls. Infliximab in the Treatment of an HIV Positive Patient with Reiter's Syndrome. Journal of Rheumatology 2003.30:2.
- Bryer Ash M, Kennedy C, Ridgway H: A case of leukonychia striata with severe erythema multiforme. Clin Exp Dermatol 6:565,1981.
- Landwehr AL, Starink TM: Inflammatory linear verrucous epidermal nevus. Dermatologica. 166:107.1983.
- Cheesebrough MJ, Kilby PE: The Inflammatory linear verrucous epidermal nevus-A case report. Clin Exp Dermatol 3:293.1978.
- Timpatanopong P, Hathirat P, Israngkura P: Nail involvement in Histiocytosis X. Argh Dermatol 120:1052.1984.
- Mann RJ, Allen BR: nail dystrophy due to sarcoidosis, Br J Dermatol 105: 599,1981.
- Kalf RE, Grossman ME: Pterygium formation due to sarcoidosis. Arch Dermatol 121:276.1985.
- Cohen PD, Lester RS. Sarcoidosis presenting as nail dystrophy. J Cutan Med Surg. 1999 Oct;3(6):302–5.
- Patel KB, Sharma OP: Nails in Sarcoidosis: Response to treatment. Arch Dermatol 119:277.1983.
- Starzycki Z. Primary syphilis of the fingers. Br J Vener Dis. 1983;59:169–71.
- K.K. Raja Babu. Nail and its Disorders. Iadvl Textbook of Dermatology R.G. Valia, Ameet R. Valia. 3rd Edition. 2008 Bhalani Publishing House, Mumbai. 949-94.
- Barth JH, Telfer NR, Dawber RPR. Nail abnormalities and autoimmunity. J Am Acad Dermatol. 1988;18:1062–5.
- Argebast KD, Lamberty LF, Koh JK et al. Congenital candidiasis limited to the nail plates. Pediatr Dermatol 1990; 7: 310–2.
- Sezer E, Koseoglu RD, Filiz N. Eccrine angiomatous hamartoma of the fingers with nail destruction. Br J Dermatol 2006; 154: 1002–4.
Onychomycosis (OM) refers to the fungal infection of nail and is the most common nail disease encountered in dermatology practice. OM may be caused by the dermatophytes, non-dermatophytic moulds (NDM) and yeast. Dermatophytes account for the majority of cases of OM and this infection of the nail is specifically termed as tinea unguium (TU). Despite various advances in the field of pathogenesis, diagnosis and drug therapy, management of OM remains a challenge. In addition to the significant cosmetic concern, OM of fingernails may result in pain/discomfort, impaired/lost tactile functions and limitation of activity while toenail involvement may interfere with walking, exercise and proper shoe fit. Like any other visible dermatologic imperfections, OM has both psychosocially and physically detrimental effects.
Predisposing Factors
There are major interregional differences in the prevalence of TU largely due to variations in the climate, demographic profile of the population, occupation, living environment and frequency of travel. Predisposing factors for TU include hot and humid climate, smoking, peripheral 120vascular disease, psoriasis, hereditary palmoplantar keratoderma, immunosuppression, repeated trauma to the nail and occlusive foot wear. In addition, avid sports participation, increasing use of health clubs and commercial swimming pools aids in the transmission of infection. Genetic predisposition to distal and lateral subungual onychomycosis (DLSO) by Trichophyton rubrum is known.1 Males are affected more frequently as compared to females possibly due to more frequent nail damage resulting from sports and leisure activities amongst male adolescents.2 Estrogen probably has a protective effect as premenopausal women are less frequently affected.3 The low incidence of TU in infants is attributed to a rapid nail growth rate with subsequent elimination of the fungus, a small contact surface with less chance of trauma and fungal colonization, a low incidence of tinea pedis and an infrequent exposure to fungi in public places. Bonifaz et al reviewed the predisposing factors for dermatophyte OM in children under two years of age and observed a positive association with Down syndrome, fungal infection on other body parts, premature birth and perinatal hypoxia and HIV infection in other family members.4 A world-wide increase in prevalence of OM in children has been noted. OM involving toe-nails is about seven times more common than that of fingernails and TU of toenails is reportedly 25 times more frequent possibly due to a three times slower growth rate.2 Though involvement of multiple toe-nails is a usual occurrence, first and the second toe are most often affected as they are more susceptible to trauma and pressure from foot-wear. Approximately 30% of patients with ringworm infection elsewhere on the body tend to acquire TU (Figure 11.1).
Etiology
Dermatophytes have been implicated in 90% cases of toe-nails and at least 50% cases of fingernail OM. Amongst dermatophytes, Trichophyton rubrum (53%) has been reported to be the most common etiological agent followed by Trichophyton mentagrophytes var interdigitale (13%), Epidermophyton floccosum (1.2%) and Microsporum species.5 In a study of 76 patients with culture positive dermatophytic toenail OM (unpublished observation), we found T. mentagrophytes to be the commonest isolate seen in 47 (61.8%) cases followed by T. rubrum (32.9%) and T. verrucosum (5.3%).

Pathogenesis
The keratolytic, proteolytic and lipolytic activities of dermatophytes aids in invasion into the skin, nail and hair. Most dermatophyte species affect the ventral and middle layers of the nail plate where the keratin is comparatively soft and in close proximity to the underlying living cells. Relatively more flexible intercellular junctions and parallel grooves and ridges over the ventral surface provide channels for hyphae to penetrate the nail plate.6
Classification, Clinical Patterns and Mode of Invasion
Fungal infection of the nail unit may be classified as superficial, distal or proximal depending on the site of fungal invasion. Recently, OM has been reclassified as primary and secondary (Table 11.1). Primary onychomycosis refers to cases where the clinical presentation is the result of invasion by the fungus. Fungal infection of nails previously afflicted with some other noninfective nail pathology is known as secondary onychomycosis. Clinical features in such cases are predominated by the underling nail pathology rather than fungal infection.
1. Distal Lateral Subungual Onychomycosis (DLSO): DLSO, also known as nail bed dermatophytosis, is the commonest clinical type of OM. It affects both finger- and toe-nails, and is characterized by the interrelated features of subungual hyperkeratosis, onycholysis and paronychia. The infection starts from the horny layer of hyponychium and later involves the nail bed and the nail plate (Figure 11.2). Thickening of the horny layer or subungual hyperkeratosis ensues disrupting the normal nail plate-nail bed attachment. The disease spreads proximally against the stream of nail growth and subsequently through the under surface of nail plate which becomes opaque.
|
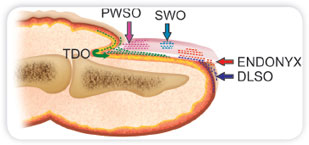

Clinically, there are discrete foci of onycholysis in the distal/lateral part and subungual hyperkeratosis accompanied by nail discoloration (Figure 11.3). The subungual hyperkeratosis provides a suitable environment for the fungus to proliferate. Sometimes, onycholysis may be the primary and predominant feature with little or no hyperkeratosis. With time, the nail bed becomes cornified and normal nail contour is lost. Nail dyspigmentation may also be seen as melanonychia or diffuse yellowish or whitish appearance that may replace the pinkish hue of a normal nail. With progress of infection, severe inflammatory reaction combined with tunnels produced by the fungus give the appearance of opaque streaks in the nail plate. These lacunae often contain masses of fungi as well as keratin debris where fungal spores can survive for weeks or months. Spikes refer to the hyperkeratotic yellow colored thickened band of nail that progress proximally towards the matrix. Thick mass of fungal hyphae and necrotic keratin between nail plate and nail bed is known as dermatophytoma. Antifungal drugs are often ineffective in treating these dormant fungal elements in dermatophytoma as they are known to form a biofilm restricting the penetration of these drugs leading to persistence of infection that often requires surgical excision.
The commonest dermatophyte species causing DLSO is Trichophyton rubrum followed by T. Mentagrophytes var. interdigitale, T. Tonsurans and Epidermophyton floccosum. One hand two feet’ tinea syndrome is a distinct clinical pattern in DLSO caused by T. rubrum in which the fungus spreads from the plantar and palmar surface of feet and hands (Figure 11.4). OM in this condition is often preceded by a traumatic event and the dominant hand that has reduced sweating and is involved in scratching the feet or picking the nails is often affected.3123

Chronic dermatophytosis syndrome, caused by T. mentagrophytes var. interdigitale presents with DLSO and tinea pedis. It starts as minute planter vesicles of size 1mm that harbour a large amount of hyphae and gradually dry up leaving a keratinous collarette. Thick skin of the soles is the predominant site of involvement. Later on other sites especially the nail beds become infected, leading to DLSO.2 A small subgroup of patients may present with moccasin type of severe tinea pedis.
2. Superficial White Onychomycosis (SWO): Superficial white onychomycosis (SWO) is a rare, distinctive pattern in which the upper surface of the nail plate is the primary site of invasion (Figure 11.2). SWO mainly involves toenails and T. mentagrophytes var. interdigitale is responsible for more than 90% of cases. The fungus possesses enzymes that allow it to digest and invade the nail plate directly. Clinically, there is presence of small well delineated opaque white islands on the dorsal nail plate which coalesce resulting in a rough, soft crumbly chalky white appearance to the entire nail surface (Figure 11.4); hence the term leukonychia trichophytica.7 Crumbled appearance helps in differentiating from leukonychia. SWO usually affects a single toe nail and may show a diffuse involvement of the nail both in width and depth. Older lesions may acquire a yellowish hue. The nail becomes friable and diffusely opaque with pigmentation varying from homogenous white to patchy yellow brown. T. mentagrophytes var. interdigitale infections present with rather pruritic, vesicular eruption affecting the plantar arch and sides of the foot and heel accompanied by superficial white onychomycosis.
Superficial black onychomycosis is also rare and caused by dematiaceous or black fungi.
SWO may be classified as classical SWO, dual invasion of the nail plate, superficial and ventral; and the pseudo-SWO with deep fungal invasion of the nail plate.8 The bipolar type is often seen in HIV positive patients and in young children with thin nails and involves both finger-and toe nails In pseudo-SWO, the crumbly appearance cannot be cleared by scraping.
3. Endonyx onychomycoses is invasion of the nail plate where the infection starts from the pulp as in DLSO, but instead of infecting the nail bed, the fungus penetrates the distal nail keratin of nail plate (Figure 11.2), where it forms milky white patches without subungual hyperkeratosis 124or onycholysis.

The nail plate develops pitting with lamellar splits and friability in the distal margin (Figure 11.5). It has been described with T. soudanense and T. violaceum infection that cause endothrix scalp infections. Endonyx is predominantly the infection of fingernails.
4. Proximal Subungual Onychomycoses (PSO): PSWO affects the fingernails and toenails equally and is primarily caused by T. rubrum, though T. Mentagrophytes, T. Schoenleinii, T. Tonsurans, and T. megninii have also been implicated. It is encountered with increased frequency in patients with AIDS. The infection starts from the stratum corneum on the ventral aspect of the proximal nail fold (Figure 11.2), migrates to the underlying matrix and then spreads distally under the nail plate. Infection occurs within the substance of the nail plate, but the surface remains intact. White discoloration under the proximal nail plate in the area of the lunula is the outcome. Clinically, there is subungual hyperkeratosis; transverse leukonychia with proximal onycholysis initially through a transparent and smooth nail plate; in due course of time subungual hyperkeratosis, onycholysis and destruction of the proximal nail plate takes place. Periungual inflammation may be quite marked and painful and associated with purulent discharge. In children, finger sucking may be the cause of paronychia. AIDS patients may present with a rapidly progressive form of PSO that occurs when CD 4 count falls to less than 450 cells/cu mm. The infection spreads rapidly under the proximal margin of all the finger and toe nails and is believed to result from the tinea pedis that precedes the onset of immunosuppression.
5. Total dystrophic onychomycosis (TDO): TDO represents the most advanced form of OM. There is total destruction of the entire nail including the nail plate, nail bed and matrix. The nail crumbles and disappears leaving a thickened abnormal dystrophic nail bed retaining keratotic nail debris (Figures 11.6 and 11.7). Secondary TDO may result from any of the four forms described above. Primary TDO is observed only in patients suffering from chronic mucocutaneous candidiasis or in immunodeficient states. Thickening of the soft tissues result in a swollen distal phalanx that is more bulbous than clubbed and the nail plate is thickened, opaque and yellow brown in colour. AIDS patients may develop an acute form of TDO, where the infection spreads from under the proximal nail fold or dorsal nail plate.125


6. Mixed pattern onychomycosis: Different clinical patterns of the nail plate infection may be encountered in the same patient in different nails as well as in the single nail. Co-occurrence of PSO and SO (Figure 11.8) or DLSO and SO is commonly seen.
Secondary onychomycosis: Fungal invasion of a previously diseased nail as seen in psoriasis, lichen planus or following trauma is well known. Such cases often present as diagnostic dilemmas with changes due to fungus superimposed over features of pre-existing nail pathology such as nail hyperkeratosis or pitting. Laboratory confirmation of the fungus becomes mandatory in such cases.
Differential Diagnosis
Clinical features seen in TU are not unique to fungal pathology and may also be seen in many other dermatoses affecting the nails. Concurrent presence of characteristic skin lesions of other dermatoses such as psoriasis, pityriasis rubra pilaris and lichen planus elsewhere on the body 126often helps to confirm the noninfective pathology.

However, sometimes nails may be the only site of involvement by the disease pathology and in such cases differentiation from TU may present a challenge. Subungual hyperkeratosis is the most important clinical feature causing diagnostic confusion between TU and other noninfective disease processes. Table 11.2 outlines in brief the various causes of subungual hyperkeratosis and their important differentiating features. Apart from subungual hyperkeratosis, other features such as onycholysis, leukonychia, nail plate fragility and discoloration seen in TU may also be encountered in other dermatologic diseases (Table 11.3).
Diagnosis of Tinea Unguium
The accuracy of clinical diagnosis in onychomycosis is low; history of tinea pedis in last one year, scaling on soles, white crumbly patches on nail, and nail discoloration are clinical predictors of a diagnosis of onychomycosis.9 The clinical presentation of onychomycosis may provide clues to the infecting organism; however, clinical appearance caused by different fungal species may be indistinguishable and laboratory diagnosis in such cases is desirable.
Specimen Collection (Table 11.4)
Proper specimen collection is central to achieving a correct diagnosis of onychomycosis. Avoidance of false negative results and elimination of contaminants are important challenges. Finger- and toe-nails should be sampled separately and associated tinea pedis or manuum should also be scraped (Table 11.4). The specimen should be obtained when the patient has been off both topical and systemic antifungal drugs for 2–4 weeks. The entire nail unit should be thoroughly cleaned with alcohol to remove contaminants. Nail clippers should be used to 127include the full thickness of nail.
|
|
|
Fine shavings or minute clippings are preferred to large pieces. The affected nail bed should be exposed by removing the onycholytic nail plate with a nail clipper and scraping the hyperkeratotic nail bed with a solid or disposable scalpel or curette. Outermost debris should be discarded and sampling of distal nail plate should be avoided as it frequently contains contaminants that may obscure the growth of pathogenic fungi. Possibility of finding viable hyphae is highest from the advancing edge closest to the cuticle. Sample may be transported in a sterile container, on a black paper sealed with tape or a pill packet or as a specifically designed mailer such as a DERMAPAK. Broth, saline or moist media should not be used as bacterial and fungal contaminants may out grow the pathogenic fungus under such conditions. Specimens should be ideally processed within a week though fungal elements can remain viable for months after specimen collection.
Diagnostic Techniques
Direct microscopy is the quickest and easiest technique to confirm the diagnosis of TU. The specimen for microscopy can be mounted in a solution of 10–30% KOH or NaOH mixed with 5% glycerol, warmed to emulsify lipids and hasten clearing.10 An alternative formulation consists of 60 mL of 20% KOH mixed with 40 mL of pure dimethylsulphoxide (DMSO), that provides a more rapid method of diagnosis of mycosis without heating and specimens lasts longer for re-examination. Potassium hydroxide digests the keratin without affecting fungal hyphae 129which becomes clearly visible and rate of clearance is directly proportional to the percentage of KOH. The slide should be examined first under 10x and then under 40x lens magnification for fungal hyphae or arthrospore or yeast forms. Fungal elements should be differentiated from artefacts including lipid vesicles, air bubbles, muscle fibre and mosaic fungus which are simulated by lipid deposition at the periphery of the host cell. Direct microscopy establishes presence or absence of fungi, but cannot identify the specific pathogen or differentiate viable from nonviable fungi.
Use of counter-stains such as chlorazol black, Chicago Sky blue or parkers blue black ink enhances the sensitivity and specificity of the procedure. Chlorozal is chitin-specific and accentuates the hyphae by staining the carbohydrate rich wall without staining potential contaminants such as cotton or elastic fibres. It is particularly useful for nail specimens where the hyphae are often sparse. Chicago Sky blue may also enhance the sensitivity and specificity of examination.11 Equi-volume mixture of Parkers Ink and KOH helps in highlighting non-dermatophyte fungi. Calcoflour white (CW), a fluorescent whitening agent that stains chitin in the fungal cell wall can also be used but requires a fluorescent microscope. Fluorescent whiteners specifically bind to plant structural proteins like chitin and lignin but not keratin. CW was found to have a sensitivity of 92% and specificity of 95% in one study.12 Phase contrast microscopy may further help to differentiate between types of hyphae or arthroconidia.13
Culture
Culture is essential for confirming the diagnosis and for ascertaining the exact etiologic fungus. Half of the specimen should be set up for culture even when microscopy is negative.
Different types of media used for culturing nail specimens include:
- Primary medium containing cycloheximide that inhibits the growth of non dermatophytic moulds and bacteria, e.g. Dermatophyte test media (DTM), Sabouraud peptone-glucose agar (Emmon's modification), Mycosel (BBL) and Mycobiotic (DIFCO).
- Secondary media like Sabouraud glucose agar (SGA), Littman's Oxgall medium and Potato dextrose agar (PDA) that are free of cycloheximide and allow isolation of nondermatophytic moulds. Antibiotics like chloramphenicol and gentamicin may be added to SGA or PDA to eliminate bacterial contamination from nonsterile sites. Specimens should be incubated at 25–30°C.
- Colonies of most dermatophytes are usually completely differentiated in 2 weeks. All plates should be kept for a minimum of 2 weeks and absence of growth even after 3-6 weeks should be taken as a negative result. Morphological and biochemical characteristics may help to differentiate various fungi. Microscopic morphology is studied by utilising teased or Scotch tape preparations in lactophenol cotton blue (LPCB). Various species of Trichophyton can be differentiated by biochemical tests such as Trichophyton agars, urea testing and hair perforation tests. Isolation of fungus also allows antifungal susceptibility testing and determination of MIC of different antifungal agents by broth microdilution method.
Growth on both types of media is indicative of a dermatophyte while growth only on cycloheximide free media is suggestive of nondermatophytic mould. If a dermatophyte is isolated, it is considered to be the likely pathogen.
A long downtime and poor yield are some of the limitations of fungal culture. False negative results may be seen when:130
- Inadequate nail sample is obtained or,
- When sample is taken from the distal part of the nail where fungal elements are not viable or,
- When the patient is receiving topical or systemic antifungal therapy.
The nail specimen must be crushed thoroughly to ensure fungal growth on the culture medium. Nail drilling has been recommended to improve the yield of fungal culture. Shemer et al found higher culture sensitivity if the sample was obtained using a driller as compared to curettage at all sites. They also found that culture sensitivity improves as the location of the sample is more proximal.14 Drilling can be done subungually (horizontal) where the driller serves as an electric curette through the nail. In the latter method, the driller is introduced through the nail plate directly above the affected area. Subungual drilling does not cause any deformity of the nail, but material from proximal and distal parts is mixed. Vertical drilling through the nail plate provides purely proximal nail material but causes transient deformation of the nail. False negative results are observed in about 10% of nail specimens under direct microscopic examination of KOH preparations and 20–35% of cultures.
Histopathology
Histopathological examination of nail specimens may be necessary when KOH preparations and culture are repeatedly negative in patients with high clinical suspicion of TU. Histopathology of nail specimens using periodic acid Schiff (PAS) stain is currently the gold standard for diagnosis of onychomycosis.15 Nail biopsy is also helpful in differentiating non-mycotic onychodystrophy caused by psoriasis and LP and ascertaining whether a fungus is invasive or just colonizing subungual debris. The fungi can be seen in the subungual keratin and under-surface of the nail plate (Figure 11.9). Presence of hyphae in the nail plate is considered to be diagnostic for onychomycosis and confirms the pathologic role of fungus. No fixative or transport media are required for HPE and samples can be processed easily observing a limited number of serial sections within 3-5 days. Histological sections may be improvised using a chitin–softening solution containing mercuric chloride, chromic acid, acetic acid and 95% alcohol. Alternatively, keeping biopsy specimen in 3% phenol for five days, 5% trichloroacetic acid, and 10% Tween-40 may also be used.13 Sections may be stained with hematoxylin and eosin as well as with periodic acid Schiff stain (PAS).


Figure 11.10: Dermatophytoma(Courtesy: Dr Chander Grover, Assistant Professor, University College of Medical Sciences, Delhi)
PAS stains glycogen and mucoproteins in the fungal cell wall. In one recent study, PAS was found to be more sensitive than KOH preparation and culture alone (92% vs 80% or 59% respectively) and PAS staining plus culture had the best sensitivity overall.16 Periodic acid-Schiff staining is the single method with the highest sensitivity in terms of detection of fungal elements (hyphae) in nail specimens. Grocott (Methenamine silver) stain and calcofluor white (CFW) stain are even more selective than PAS and vital stains like neutral red can help in distinguishing between viable and non-fungal elements. GMS provides greater contrast between the fungus and the surroundings. The latter, however, can only be performed on fresh smears from subungual hyperkeratosis and from scrapings of SWO.
Pretreatment with sodium hydroxide prior to processing improves the quality of sections for both hematoxylin-eosin-stained and periodic acid Schiff-stained slides with reduced tissue folding and fragmentation, ease of cutting, and tissue adherence to glass slides. This reduces the need for repeat sections and prevents delays in turnaround time.15
Alternatively, nail plate clipping/fragment can be sent in a 10% buffered formalin container for histopathological analysis such as PAS. Nail clippings may be embedded in paraffin without any prior fixation. Histopathological processing and PAS staining of nail dipping specimen can give results as good as those obtained from biopsy and is faster, economical and painless. In cases with prior antifungal treatment, histological analysis of PAS-stained nails clippings should be considered as an appropriate diagnostic tool. Histopathology of subungual hyperkeratosis alone may be enough to reach a diagnosis of onychomycosis obviating the need for histopathology of nail plate.17
However, unlike culture, HPE cannot differentiate between viable or nonviable organisms nor does it help to identify the particular pathogen as both dermatophytes and moulds produce hyphae and large, thick-walled arthrospores.
Other less frequently used tests to diagnose onychomycoses include:
- Immunohistochemistry
- Dual flow cytometry: These techniques are useful when identifying mixed infections and allowing for quantification of the fungal load in the nail plate. Immunohistochemistry and flow-cytometry have also been used in anecdotal studies.13
- DNA based methods such as PCR-RFLP assays, double round PCR, real time PCR and PCR 132direct sequencing have been used recently for detecting fungi.13 Triplex PCR and topo-isomerase II PCR have also been used recently with success. Triplex PCR has a very high sensitivity and specificity and can differentiate between dermatophyte, candida and molds.13 In a study, combination of PCR and CFW was found to more sensitive than CFW and culture.18 However, the DNA based methods cannot ascertain the viability and feasibility of fungus.
- Likewise, the role of scanning electron microscopy and confocal microscopy in onychomycosis at present is primarily for research. Confocal laser scanning microscopy is comparable to PAS and superior to KOH; however, their use is currently limited by their cost and complicated technique.
- Optic coherence tomography is a reliable, convenient, noninvasive technique used to visualise fungal elements in vivo based on measurement of reflected infrared light intensity as a function of position. Several areas in the nail can be screened at once making it possible to detect persisting hyphae during systemic or topical treatment. High cost and limited availability currently prevent widespread use of this technique.
- Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry and phase contrast hard X-ray microscopy are other techniques under evaluation.
- Nail digital dermoscopy: Jagged proximal edge with spikes of the onycholytic area and longitudinal striae are believed to be predictive of onychomycosis.
Treatment
Onychomycosis is a cosmetically disfiguring and debilitating disease adversely affecting the self-esteem of the patients and leading to depression. Apart from the pain and difficulty in walking, it carries the risk of cellulitis in elderly and diabetic foot in predisposed patients. No spontaneous clearing is known to occur and untreated patients can act as a reservoir for close family contacts and can contaminate communal bathing places. As a result, successful treatment of this condition is essential. However, treatment should not be instituted on clinical grounds alone.
There are various challenges to the successful treatment of TU. Extensive variability in the methods in drug trials makes interpretation of results difficult. The primary reason for this is the lack of consistency in defining and measuring cure. Secondly, efficacy assessment are often based on final evaluation at 48 to 52 weeks, whereas it takes around 4–6 months and 12 to 18 months for a deceased finger or toenail to be replaced respectively. In the treatment of onychomycoses, the desired endpoints are mycological cure and clinical recovery. Mycological cure is defined as negative microscopy and culture. Clinical cure is defined as a nail without any clinical signs of onychomycosis whereas complete cure is defined as having both mycological and clinical cure. Clinical recovery however depends a lot on the pre-existing condition of the nail including any other dermatoses like psoriasis or lichen planus or trauma. In severe cases of onychomycoses, up to 10% of the nail surface is likely to remain abnormal in appearance even when mycological cure has been attained. Therefore, clearance of the nail plate is a more appropriate term defined either by : clinical cure with 100% clearance of signs or clinical success with a residual affected nail area less than 10% with restoration of normal nail growth (at least 4 or 5 mm in 6 months) and no signs of onycholysis, hyperkeratosis, paronychia, discoloration or fragility. An ideal antifungal drug would be one that concentrates in the nail-bed and plate at levels toxic to the fungus but not the patient, with good long term cure rates, limited drug-drug interactions and minimal or no side effects. It should be broad spectrum, have favorable nail kinetics and yet be economical.19 133
|
Various factors influence the choice of antifungal for use in OM (Table 11.5). These include site of involvement, clinical type of onychomycosis, number of nails involved, patients’ age, pre-morbid conditions and current drug intake, expected compliance and cost of treatment regime. SWO has the best therapeutic response and TDO usually has a poor outcome even after adequate treatment.20 Lateral edge disease of nail plate is more difficult to treat.
Treatment can be either:
- Medical:
- Topical
- Systemic or
- Combination of topical and systemic
- Laser
- Light therapy
- Surgical
Topical Therapy
Topical therapy is especially desirable where systemic therapy is contraindicated due to risk of adverse effects or drug interactions. The nail plate that is composed of around 20 layers of 134tightly bound keratinized cells and mean nail plate thickness increases progressively along the entire length of nail plate. Topical therapy carries the problem of inadequate penetration and prolonged transport lag time with low drug levels in the nail bed, long duration of treatment, low cure rates and high rate of recurrence. Topical preparations of anti-fungal drugs as powders, creams, solutions and ointments are not adapted for use in the nails due to insufficient adhesion to the base and insufficient penetration into the nail. Penetration of topical drugs is, however, faster than oral drugs when used with optimum vehicle such as a lacquer. Lacquers are specialized transungual drug delivery systems (TUDDS) that produce a non water soluble film following application and evaporation of solvent which remains in contact with the nail for extended period of time. In TUDDS, the active ingredient remains in contact with the nail for long periods. Secondly, with evaporation of the solvent, the concentration of the active ingredient in the remaining film reservoir increases manifold, thus providing the high concentration gradient essential for maximal penetration. Furthermore, as the lacquer acts as occlusive agents, transungual water loss is further reduced, enhancing the mass transport of the drug into and through the nail plate. TUDDS may be used as:
- Water-insoluble polymers that create a film on the nail surface requiring daily or weekly application and removal with organic solvents or nail filing.
- Water-soluble, hydroalcoholic solutions of hydroxypropyl chitosan, forming an invisible non-irritating film which can be easily removed.20
The two main drugs that have been used via the topical route are ciclopirox and amorolfine. Ciclopirox is a hydroxypyridone derivative with fungicidal action against dermatophytes. It acts as a chelating agent and inhibits several iron- and aluminium-dependent mitochondrial enzymes and mitochondrial electron transport processes leading to reduced synthesis of proteins and nucleic acids. It penetrates into mycotic nail keratin more rapidly than healthy nail and the 8% concentration of ciclopirox in nail lacquer increases to 34.8% on application. Ciclopirox is applied to the nail as a coat daily over and above the previous applications. The layer of the lacquer is removed once weekly. Treatment needs to be continued for 48 weeks for an effective response. Mycological cure rates ranging from 46–85% were reported in a meta-analysis.21 It is generally well-tolerated with few adverse effects such as periungual erythema, transient irritation, and burning and itching of nail bed or adjacent skin.
Amorolfine is a morpholine derivative with fungicidal and fungistatic effect against dermatophytes. It affects membrane fluidity by inhibiting 2 important enzymes namely: 14 α reductase and delta 7–8 isomerase involved in ergosterol biosynthesis. Concentration of amorolfine increases from 5% to 27% with solvent evaporation. The nail lacquer formulation helps in preventing reinfection from propagules present in shoes and also helps to increase nail hydration by semi-occlusion, thus limiting the formation and persistence of drug resistance fungal spores. Amorolfine nail lacquer (ANL) is applied once or twice per week for 6–12 months. The drug can be detected in the nail for up to 2 weeks after discontinuation. Clinical cure rates in the range of 38% to 54% have been reported with amorolfine.22,23 Beneficial results have also been obtained in patients with diabetes where oral therapies may sometimes be contraindicated due to concomitant drug intake. Adverse events are rare and include local irritation, onycholysis, contact dermatitis and bluish or yellowish nail discolouration. No systemic side-effects have been reported with the use of these lacquers.
Chemical penetration enhancers (CPE) such as dimethyl sulfoxide (DMSO) and urea, bioadhesive polymers such as Carbopol 971P and Klucel MF or surface modifiers like tartaric acid and phosphoric acid gel may also be used to enhance penetration of topical drugs into the nail.18135
Other topical agents: A terbinafine nail solution was shown to be more effective than ciclopirox nail lacquer when used on a guinea pig model. Terbinafine nail solution was also shown to be safe and efficacious when delivered through iontophoresis.19
A ciclopirox hydrolacquer based on water soluble biopolymer technology was shown to be more effective than conventional available lacquer in a recent study.19
Baran et al reported efficacy of a solution of 1% fluconazole and 20% urea in a mixture of ethanol and water applied daily in treatment of oychomycoses affecting the distal nail.24
AN2690 is a novel oxaborole broad spectrum antifungal designed with properties required to allow for easier penetration through the nail plate, has been shown to have superior in vitro penetration compared to ciclopiroxolamine.25 It inhibits a vital fungal enzyme, leucyl transfer RNA synthetase (LeuRS) required for protein synthesis.25
Various newer strategies to enhance the penetration of topically applied drugs to the nails are also under study. These include disrupting the nail plate using physical techniques or chemical agents.
Physical techniques that can be employed are manual and electrical nail abrasion, acid etching, ablation by lasers, microporation, application of low-frequency ultrasound and electric currents. Nail abrasion thins the nail plate, decreases the fungal mass, exposes the infected nail bed and enhances the action of topical antifungal. Etching of nail plate is done using 20% tartaric acid and 10% phosphoric acid. It increases surface area and adhesion of active compound resulting in formation of profuse micro porosities. Microporation of nail plate creates micro channels in the nail plate increasing penetration in deep layers.26 In phonophoresis, ultrasound waves are transferred though a coupling medium onto nail surface.
Chemicals like thiols, sulphites, hydrogen peroxide, urea, water, enzymes have also shown ungual enhancer activity.19 Nail avulsion can be achieved using surgery, chemical (40% urea) and CO2 laser. At a cellular level, opening of pores in the cell membrane (secondary to lipid bilayer alteration) enhance drug diffusion. Alternatively, drug permeation into the intact nail plate may be encouraged, for example, by iontophoresis or by formulating the drug within a vehicle which enables high drug partition out of the vehicle and into the nail plate. Iontophoresis enhances drug diffusion through the hydrated keratin of nail. Lastly, nano emulsions are oil in water emulsions with encapsulated antifungal drugs that penetrate deeper and diffuse laterally and achieve high levels in nail plate and nail bed.
Systemic Therapy
Systemic therapy forms the cornerstone of treatment of TU. A study evaluating management of presumed onychomycoses in private practice found that terbinafine was the most commonly prescribed oral treatment and frequently instituted in the absence of any matrix involvement and without confirmation of the diagnosis.27 In fact patient satisfaction with onychomycosis therapy has also been reported to be more with oral as compared to topical therapy.28 Systemic therapy however, carries the drawback of high cost, low levels in nails due to decreased peripheral circulation and drug interactions in elderly population. Penetration of oral drugs into the nail plate may be sub-optimal in cases where the nail plate has separated from the bed.
Oral antifungals used to treat TU include: griseofulvin, azoles including ketoconazole, itraconazole and fluconazole, and allylamine terbinafine.136
Griseofulvin: One of the oldest oral antifungal drugs, griseofulvin is derived from certain Penicillium species such as P. Griseofulvum. It acts by blocking the formation of mitotic spindle and is effective only against dermatophytes. It takes a long time to saturate the nail and persists in the nail for just around 2 weeks after stopping therapy. This necessitates prolonged administration (4–6 months for fingernails and 10–18 months for toenails) and results in poor compliance. Mycological cure rates in fingernail infections are around 70% while in toenail onychomycoses, reported efficacy is only 30–40%. The adult dose is 500 mg to 1 gm given for 6–9 months in fingernail infection and 12–18 months in toenail infection. Up to 2 g may be used in recalcitrant cases. Absorption is increased with ultra-micronized or micronized particle form and with fatty food. Efficacy can be increased using cimetidine, a microsomal enzyme inhibitor. It is contraindicated in pregnancy, lupus erythematosus, hepatocellular failure and acute intermittent porphyria. It may interfere with oral contraceptives and cause fetal abnormalities (Table 11.6). Due to availability of more effective drugs for the management of TU, the role of griseofulvin is limited to treatment of tinea capitis, especially due to Microsporum species.
Azole antifungals inhibit the synthesis of ergosterol thus reducing membrane bound enzyme activity and interrupting chitin synthesis and making cell membrane more permeable.
Ketoconazole, an imidazole derivative, acts by blocking the cytochrome P-450 enzyme used in the conversion of lanosterol to ergosterol in the formation of fungal cell membrane. Blockage of human cytochrome P-450 dependent adrenal androgen bio-synthesis may result in gynecomastia, especially at higher doses above 600 mg daily. Drug-induced hepatitis has been reported rarely. Daily recommended dose is 200–400 mg/day administered with meals for 6-12 months. Ketoconazole is not recommended for routine use in onychomycosis in view of its significant adverse effects, especially liver injury and availability of more efficacious and safer options.
|
Fluconazole is a water soluble drug, that possibly aides in rapid penetration into the nail plate with detectable levels at 48 hours. It persists in cured nails in high concentrations 3–6 months after the end of treatment. Oral bioavailability is high and not dependent on gastric PH, presence of food, antacids or H2 receptor antagonists. Rapid penetration into nails and tendency to be retained and concentrated in keratinous structures make once weekly administration sufficient. It is not generally recommended as first-line therapy because of limited data concerning its use in monotherapy for dermatophyte onychomycosis. A recent review evaluating seven studies using fluconazole treatment for onychomycosis found mycological cure rates ranging from 36% to 100% for placebo controlled studies. However, the cure rates were lower (31%) when compared with terbinafine (75%) and itraconazole (61%).29 Doses of 150 mg, 300 mg, 450 mg were all shown to be effective with no significant difference.30 Complete cure rates of only 15% to 36% have been achieved even when using higher doses of fluconazole.31 A daily and alternate day 100 mg/day dosing regimen had also been reported to give a success rate of 80%.2 Hepatic side effects are lesser as compared to other congeners (Table 11.6). Fluconazole inhibits both CYP3A4 and CYP2C9 and close monitoring is required when prescribing drugs metabolized by these enzymes with narrow therapeutic index. Simultaneous use of fluconazole and terfenadine or cisapride is contraindicated. Drug interactions are fewer with fluconazole especially when administered once weekly.
Itraconazole is a triazole antifungal with mechanism of action similar to ketoconazole, though it binds more specifically to fungal cytochrome P-450 and only weakly to the mammalian enzyme. It is a highly lipophilic drug, oral bioavailability is maximum when taken with a full meal and is enhanced by acidic conditions. Absorption is further enhanced in a cyclodextrin formulation used for treatment of severe oropharyngeal candidiasis. Itraconazole shows very strong binding to keratin and nails take up and concentrate itraconazole. Concentration is even higher at the site of infection such as subungual hyperkeratosis as compared to nail clippings. Itraconazole is incorporated into the nail through both nail matrix and nail bed and is detectable in the nail as early as 7 days after starting therapy and persists for up to 6–9 months following discontinuation of therapy. Rapid appearance, concentration and persistence of itraconazole in the nail plate make the intermittent dosing regimen as efficacious as the continuous regime. Besides, intermittent therapy is more economical and results in higher maximum plasma concentrations but lower total systemic exposure compared with the continuous regime. Itraconazole binding to mammalian cytochrome P450 3A4 system in the liver is responsible for most aspects of potential itraconazole toxicity and drug-drug interactions (Table 11.7). Asymptomatic abnormalities of liver function occur in less than 3% patients.19 Hepatitis occurs with continuous therapy and usually after 4 weeks of therapy. One case of severe hepatic dysfunction requiring liver transplantation has also been reported.32 Monitoring for hepatic functions is recommended in patients with pre-existing derangement, those receiving continuous therapy for > 1 month and with concomitant use of other hepatotoxic drugs and in those who have experienced liver toxicity with other drugs. It is contraindicated in patients with congestive cardiac failure due to increased risk of negative inotropic effects and therefore carries a black box warning regarding heart failure. Due to its ability to prolong the QT interval and increase the risk of arrhythmia, drugs like cisapride, pimozide and quinidine are contraindicated for co-administration. Itraconazole is given as a 200 mg dose once daily for 3 months or preferably as pulse regime with 200 mg twice daily for 1 week each month. Two such pulses are given for finger-nail onychomycoses and 3 for toe-nail disease. Intermittent therapy was shown to have equal mycological and higher clinical cure rates in a multicentric double blind randomized trial comparing the continuous and daily regimen.33138
|
Terbinafine: Terbinafine, an allyamine, inhibits the fungal squalene epoxidase, leading to accumulation of squalene and deficiency of ergosterol. Intracellular squalene accumulation is possibly responsible for the fungicidal effects of terbinafine whereas fungistatic action is the result of ergosterol deficiency. Terbinafine is well-absorbed orally with more than 70% bioavailability. It is widely distributed in various body tissues including the nail matrix. It is keratinophilic and detectable in the nail within 24 hours after initiating therapy and up to 90 days after stopping treatment. In vitro terbinafine is fungicidal against dermatophytes. Due to few reports of occurrence of SLE, SCLE, bullous pemphigoid and autoimmune hepatitis in patients receiving terbinafine, it is prudent to exert caution when using in patients with known autoimmunity.19 It is FDA approved as a continuous treatment with dose of 250 mg daily for 6 weeks for fingernail onychomycoses and 12 weeks for toenail onychomycoses. The LION study demonstrated superiority of terbinafine in terms of long-term mycological and clinical cure and lower risk of recurrence than itraconazole.34 In a cumulative meta-analysis of randomized controlled trials, mycological cure rates of 76 ± 3%, 63 ± 7%, and 59 ± 5% were reported with terbinafine, itraconazole pulse and itraconazole continuous regimes, respectively. The corresponding values for clinical response were as follows: terbinafine 66 ± 5%, pulse intraconazole 70 ± 11%, and continuous itraconazole 70 ± 5%.35 Long-term efficacy of terbinafine has also been found to be superior to itraconazole, fluconazole, and ketoconazole.36,37
Considering that terbinafine persists in the nail for long periods after discontinuing therapy, various intermittent regimes have been tried with variable success. Gupta et al used an intermittent terbinafine regime consisting of 2 courses of terbinafine 250 mg daily given for 4 weeks with an interval of 4 weeks without terbinafine. They found this intermittent regime to be as effective as continuous terbinafine and more efficacious than pulse itraconazole for treatment of toe nail onychomycoses.38 We compared the efficacy and tolerability at 12 weeks and 24 weeks, of continuous (250 mg once daily) and pulse dose terbinafine (500 mg daily for first week every 4 weeks) continued for 12 weeks in the treatment of dermatophyte toe-nail onychomycosis (unpublished observation) in a randomized double blind trial and did not found statistically significant difference in the clinical, mycological and complete cure rates. A regimen of three pulses of terbinafine therapy given 250 mg twice daily for 1 week every month for 3 months given alone or in combination with topical application of terbinafine cream has also been reported to be effective in treating TU.39,40 Sikder et al found 4 pulses of 250 mg terbinafine for one week more effective than itraconazole administered intermittently for 4 weeks.41
The hepatic side effects of oral antifungals remain a concern (Table 11.6). However, Chang et al studied the safety of all oral antifungal in the treatment of OM and found a low incidence of liver related side effects associated with use of all oral antifungals in immunocompetent patients.42
Newer systemic antifungal drugs: Gupta et al evaluated the role of ravuconazole in the treatment of DLSO. Mycological cure was seen in 59% of subjects in the 200 mg/day group, which was significantly higher than the rates found in the other groups. Drug-related adverse events were infrequent in all treatment arms with headache being commonest.43 Posaconazole pulse therapy (oral suspension of 400 mg twice daily, taken with a meal on the first 5 days of each month, repeated for 3 months) has been reported to produce partial response.44 Pramiconazole is a new addition to the family of triazole agents. It is absorbed rapidly and has a long half-life making once daily dosing feasible. In pre-clinical studies, it has shown similar/superior activity to ketoconazole and itraconazole. 140
Lasers
Laser systems are the latest edition to the therapeutic armamentarium for TU. Currently, two laser systems—Pinpointe and Genesis Plus are FDA approved for use in OM. PinPointe FootLaser (Patholase) is a new high powered pulsed Nd: Yag laser at 1064 nm. High rates of mycological cure and clinical clearance with very little pain have been reported with this Laser. The laser causes photoinactivation of the fungal pathogens at a depth below the nail tissue surface without causing collateral damage and leaving the surrounding tissue intact. Difficulties in selectively delivering laser energy to deeper levels of nail plate without collateral damage, however, interfere with complete elimination of the fungus. Prior reduction of thickness of severely dystrophic nails enables the optimal effect of the laser procedure.20 Femtosecond (fsec) infrared titanium sapphire laser have also shown successful results.19
Landsman et al recently reported efficacy of Noveon dual-wavelength (using 870- and 930-nm light) near-infrared diode laser in the treatment of moderate to severe onychomycoses. It causes photo inactivation of the fungal hyphae and spores without causing photoablation toxic plume associated with pulsed Nd:YAG lasers. There is minimal thermal effect and no damage to underlying nail structure. The probes are disposable and developed specifically for nails and up to 4 nails can be treated simultaneously. The study showed clinical cure in 85% and negative culture in 30% cases. Review of 270-day mycological data confirmed further decrease in both clinical and mycological parameters.45,46
Light Therapy
Application of germicidal UVC radiation has shown to successfully inactivate dermatophytes in TU patients.19 Photodynamic therapy (PDT) has also been used successfully to treat T. rubrum infection. PDT can be considered as an alternative therapeutic option in patients where systemic antifungal treatment is contraindicated. It carries the advantage of being minimally invasive and locally active, with no damage to healthy tissues or systemic side-effects. There are no reports of fungal resistance, cumulative toxicity or mutagenic effects which allows repeated treatments. 5-aminolevulinic acid (ALA) is taken up directly by the organism, which then induces accumulation of protoporphyrin IX (PPIX). Subsequent light irradiation of PPIX leads to its inactivation due to photodamage to the cellular structure. Techniques proposed to ensure adequate penetration of ALA into the nail include use of penetration enhancers or iron chelators or filing of dorsal surface of the nail. Discomfort reported by the patients during illumination, transient local phototoxic reactions and need for pretreatment with urea and removal of hyperkeratosis to achieve adequate ALA levels are the few limitations associated with PDT in OM.47
Combination Therapy
Treatment failure and relapse are the biggest challenges in the treatment of TU. Mycological cure rates are about 30% better than clinical cure rates in the majority of studies, with the latter often below 50%. Even for terbinafine and itraconazole which were initially believed to be very effective, clinical success rates are just 35–50% and 25–40% for terbinafine monotherapy and itraconazole monotherapy, respectively. The relapse rate even in the best clinical trials is at least 25%. This has necessitated the use of combination therapy in an attempt to improve the cure rate and reduce relapse. Rapid accumulation and binding to nail matrix and prolonged 141retention due to binding to nail matrix are the advantages of oral antifungals. However, drug accumulation after systemic therapy is delayed and may even be suboptimal in the lateral borders of nail. These problems can be circumvented with topical therapies such as amorolfine that reach the nail within hours after application and penetrate the nail plate including the lateral margins. The latter, however, may not penetrate the deeper layers of nail sufficiently where oral drugs are more likely to reach and concentrate. Combination of different treatment modalities may be synergistic with drugs acting at different levels. The combination of oral and topical drugs may allow reduction in oral dosing and shorten the total duration of therapy and drug toxicity resulting in increased patient tolerance and compliance while improving efficacy and reducing relapse. Likewise, combination of surgical therapies like physical debridement can reduce the fungal load and aid drug penetration. Combination of amorolfine with itraconazole was shown to be more efficacious than itraconazole alone (87% vs 46%).48 In a randomized study, Baran et al reported combination of amorolfine plus terbinafine to be twice as effective as terbinafine monotherapy (27% vs 17%).49 The combination regimes can be administered sequentially or in parallel. In parallel treatment, both oral and topical drugs are given simultaneously and is used in patients likely to fail therapy. Sequential therapy involves administration of oral drug alone for a period of time followed by topical drug and is recommended for patients showing a poor response to treatment such as positive microscopy after 3–6 months of treatment.19
Supplementary Therapy
Supplementary therapy involves microscopic examination and culture at 24 weeks or 6 months following start of therapy and extended administration of oral antifungal (4 weeks of daily terbinafine or another pulse of itraconazole) in patients with positive culture. This is based on the belief that there is a window of opportunity for booster therapy until 6–9 months from start of therapy during which residual drug concentration can still be detected within the nail and a short burst of extra therapy during this time may be just sufficient o produce cure especially in patients who were likely to fail therapy.
Sequential Therapy
Sequential therapy combines the use of two oral antifungal working at two different pathways in ergosterol metabolism. In this regime, the duration of active drug therapy and cumulative drug exposure to each of the two drugs is reduced. In this therapy, patients were given 2 pulses of itraconazole followed by one or two pulses of terbinafine. The results were compared with patients receiving 3–4 pulses of terbinafine alone. Complete cure was seen in 52% vs 32% patients’ respectively.19 Itraconazole is administered before terbinafine because the former is barely detectable in plasma 10-14 days after completing a pulse thus limiting the cumulative hepatotoxicity and drug interactions of terbinafine and itraconazole.
BATT and BOAT
The boosted oral antifungal treatment (BOAT) therapy are designed to target dormant chlamydospores and arthroconidia within the nail plate in order to produce sensitive hyphae which are less refractory to treatment with antifungals. This is performed by securing a piece of Sabarauds dextrose agar on to the affected nail plate for 48 hours following the weekly pulse 142of itraconazole. A pilot study suggested that this protocol improves the mycological cure rate compared to conventional treatments (> 90%).19 A similar approach is boosted antifungal topical treatment (BATT), designed to improve the therapeutic efficacy of amorolfine nail lacquer.19 These therapies, however, carry the risk of over stimulation and systemic spread of fungi that are not susceptible to the antifungal agent and are therefore not yet widely accepted.
Surgical Intervention
As the thickened nail plate with subungual hyperkeratosis is most often responsible for inadequate penetration of drugs, removal of the same may enhance the success rate as well as shorten the duration of therapy. The partial removal of the nail can be the most effective option in cases of lateral nail plate involvement or in patients with onycholytic pockets or canals on the under surface of the nail filled with a longitudinal spike (dermatophytoma). Surgical methods can be used to remove part (debridement) or all (avulsion) of the nail plate. Such methods usually should be combined with oral and/or topical treatments and not used alone. They may be combined with topical therapy if oral antifungals are contraindicated. Nails can be removed using a carbon dioxide laser. Surgical distal removal is a painful procedure and carries the risk of infection and abnormal nail regrowth (distal nail embedding), which is frequent. Nail plate removal should be accompanied by debridement of subungual debris from the nail bed or grooves. After nail avulsion, the distal nail bed can sometimes lift because upward forces are no longer counteracted by the downward forces usually exerted by the nail plate. In addition, there may be shrinkage of nail bed and distal ingrown edge. Malay et al found combination of debridement and nail lacquer application (76.74% rate mycological cure) to be more effective than debridement alone. None of the patients in the debridement-only group experienced mycological cure.50 However, Grover et al did not find good results when surgical nail avulsion for single nail onychomycoses was combined with topical application of antifungal creams.51
Chemical nail avulsion involving application of keratolytic chemical, such as 40% urea to the affected nail, resulting in chemical onycholysis can also be employed. The affected portion of the nail plate can be subsequently trimmed. Chemical avulsion reduces the fungal load to a lesser extent than surgical avulsion as it may not eliminate fungi located beneath the margin of the remaining normal nail portion. Chemical removal should be reserved for patients with very thick nails and for patients unable to tolerate mechanical removal. It is generally not indicated in the elderly because of application difficulties, in patients with multiple infected toenails (burdensome) or when the infection has spread beneath the proximal nail fold. Apart from avulsion, mechanical nail abrasion using sandpaper fraises or a high speed hand piece at the beginning of treatment with antifungal nail lacquer decreases the critical fungal mass and aides the penetration of the topical agent into the deepest nail layers. The procedure when used alone or in combination with topical antifungal application has produced 40–68% cure rates.20
Relapse
Onychomycosis relapse is defined as the reappearance of the same infection, whatever time has elapsed. It can be due either to reinfection or recurrence. Recurrence may be defined as the return of the disease within 1 year of therapy completion. Reinfection implies contracting the infection again after having achieved cure, usually after a period of one year. Reinfection usually indicates the predisposition of a particular individual towards acquiring an infection which can be due to multiple factors like lifestyle, age, genetic factors, occupation, climate, nature 143and extent of initial infection, close or repeated exposure to an infected contact or presence of associated comorbid conditions like DM, immunosuppression, and associated tinea pedis.
Therapeutic failure can occur due to lack of diagnostic accuracy, inappropriate choice of antifungal or mode of delivery, presence of dormant conidia as in dermatophytoma, sequestrated mycelium pockets or resistant fungal species or lack of consistent penetration. Certain prognostic factors can help determine the choice of therapeutic agent, length of treatment and duration of follow-up and may help in identifying cases requiring extended/individualized treatment and reduce the chances of failure and subsequently relapse (Table 11.8). Combined itraconazole and pentoxifylline or itraconazole and topical amorolfine were found to be more useful than systemic monotherapy alone.52
Drug Resistance
Terbinafine is the most effective and potent drug against dermatophytes. Resistance to terbinafine though rare, has been reported.53 Resistance to azole antifungals is more widely known.54 Organisms resistant to one group are usually sensitive to the antifungal from other group, possibly suggesting a target specific mechanism of resistance. Antifungal susceptibility testing may be undertaken in patients showing poor or unsatisfactory response to the treatment.
Special Populations
Pregnancy and Lactation
Itraconazole and fluconazole are category C drugs while terbinafine is category B. Use of systemic drugs should be avoided in pregnancy and topical therapies are the mainstay of therapy in this population.55
|
All oral antifungals are excreted in breast milk and therefore contraindicated in lactating mothers.
Children
Children with onychomycoses should be screened carefully for concomitant tinea capitis and pedis. Parents and siblings should also be screened for any cutaneous mycoses. Griseofulvin is the only licensed antifungal for use in children with onychomycosis with a recommended dose for age groups of one month and above of 10 mg/kg daily (micronized and ultra micronized preparation). None of the newer antifungals including terbinafine and itraconazole are approved for use in children and laboratory testing including hemogram, liver function tests and serum electrolytes should be carried out every 4–8 weeks to look for possible side effects. However, both terbinafine and itraconazole have been safely used in treatment of onychomycoses with favourable outcome and the former is approved for treatment of tinea capitis in children above 4 years of age. Ginter Haanselmeyer et al have used terbinafine and itraconazole in their series of 36 patients aged 4–17 years and reported no significant side effects specific to children (Table 11.9).56 Fluconazole in a dose of 3–6 mg/kg given daily or in pulse regimen is considered safe in children.
Elderly
Poor peripheral circulation, diabetes, repeated nail trauma, longer exposure to pathogenic fungi, suboptimal immune function and inactivity or inability to cut toe nails or maintain good/standard foot care are some of the factors leading to increased incidence and poor response to treatment in elderly. However, a multitude of other disorders like trauma, psoriasis, and lichen planus may lead to onychodystrophy in elderly. Therefore, the clinical impression of TU should be confirmed by mycological examination, whenever possible. The management of TU may include no therapy, palliative treatment with mechanical or chemical debridement, topical antifungal therapy, oral antifungal agents or a combination of treatment modalities. Gupta et al have reported both continuous terbinafine and pulse itraconazole to be safe in elderly patients.57 Terbinafine is considered the drug of choice for TU, with greater mycological cure rates, less serious and fewer drug interactions, and a lower cost than continuous itraconazole therapy. In general, topical nail lacquers, amorolfine and ciclopirox are not practical for elderly patients because of the recommended frequency of application, periodic routine debridement of affected nails and long duration of therapy. However, nail lacquers may be a good option as monotherapy for patients with superficial white onychomycosis or in combination with systemic antifungal therapy for patients with recurrence. They may also be considered for patients receiving multiple concomitant medications due to risk of possible interactions.
|
Diabetics
Diabetics are reported to be 2.5–2.8 times more likely to have OM than the control population and the risk is further increased in male patients. The combination of ischaemia, sensory neuropathy and direct adverse effects on host defence mechanisms render these patients especially vulnerable to foot infections. Other factors associated with higher rates of infection include increasing age, peripheral vascular disease (PVD), poor glycemic control, obesity and hypertriglyceridaemia. Ulcerated onychomycotic toe nails may become thick, cause pressure effects and subsequently lead to severe complications like diabetic foot.
The treatment is particularly challenging due to multitude of possible drug interactions of most oral antifungals with concomitant medications used for diabetes. Topical preparations are preferable but carry the drawback of prolonged treatment and cumbersome application due to comorbid obesity and advanced age. Foot care interventions including nail drilling in combination with topical therapies have been shown to be effective in the treatment of OM in diabetics. Data from clinical trials suggest that drug interactions resulting in hypoglycaemia may not be an important issue when itraconazole and terbinafine are used in diabetic patients receiving concomitant hypoglycemic medications.58 Terbinafine forms the first line of treatment due to its relatively low risk of drug-drug interactions and proven efficacy in this population. Though itraconazole has also been shown to be safe and effective, its black box cardiac warning and drug interactions prevents its use as a first line drug.
References
- Zaias N, Tosti A, Rebell G et al. Autosomal dominant pattern of distal subungual onychomycosis caused by Trichophyton rubrum. J Am Acad Dermatol 1996;34:302–304.
- Baran R, Hay R, Haneke E, Tosti A editors. Onychomycosis: The current approach to diagnosis and therapy. London: Informa Healthcare; 2006.
- Sobera JO, Elewski BE. Onychomycosis. In: Scher RK, Daniel CR, editors. Nails: diagnosis, therapy, surgery. 3rd Edition. Philadelphia: Elsevier Saunders; 2005.p 123-131.
- Bonifaz A, Saúl A, Mena C, Valencia A, Parades V, Fierro L, et al. Dermatophyte onychomycosis in children under 2 years of age: experience of 16 cases. J Eur Acad Dermatol Venereol 2007;211:115–7.
- Hay RJ, Baran R. Onychomycosis: a proposed revision of the clinical classification. J Am Acad Dermatol. 2011;65:1219–27.
- Rashid A, Scott E, Richardson MD. Early events in the invasion of the human nail plate by Trichophyton mentagrophytes. Br J Dermatol. 1995;133:932–40.
- Hay RJ, Baran R, Haneke E. Fungal (Onychomycosis) and other infections involving the nail apparatus. In: Hay RJ, Baran R, Haneke E editors. Baran and Dawber's Diseases of the nails and their management. 3rd ed. London: Blackwellscience; 2001. p129-171.
- Baran R, Hay R, Perrin C. Superficial white onychomycosis revisited. J Eur Acad Dermatol Venereol 2004; 185: 569–71.
- Fletcher CL, Hay RJ, Smeeton NC. Onychomycosis: the development of a clinical diagnostic aid for toenail disease. Part I. Establishing discriminating historical and clinical features. Br J Dermatol. 2004 Apr;150:701-5.
- Kaur R, Kashyap B, Bhalla P. Onychomycosis—epidemiology, diagnosis and management. Indian J Med Microbiol 2008;26:108–16.
- Haldane DJ, Robart E. A comparison of calcofluor white, potassium hydroxide, and culture for the laboratory diagnosis of superficial fungal infection. Diagn Microbiol Infect Dis 1990;13:337–39.
- Grover C, Khurana A. Onychomycosis: newer insights in pathogenesis and diagnosis. Indian J Dermatol Venereol Leprol. 2012;78:263–70.
- Shemer A, Trau H, Davidovici B, Grunwald MH, Amichai B. Collection of fungi samples from nails: comparative study of curettage and drilling techniques. J Eur Acad Dermatol Venereol 2008;22:182–85.
- Nazarian RM, Due B, Deshpande A, Duncan LM, Misdraji J. An improved method of surgical pathology testing for onychomycosis. J Am Acad Dermatol. 2012;66:655–60.
- Weinberg JM, Koestenblatt EK, Tutrone WD, Tishler HR, Najarian L. Comparision of diagnostic methods in the evaluation of onychomycosis. J Am Acad Dermatol 2003;49:193–7.
- Chang A, Wharton J, Tam S, Kovich OI, Kamino H. A modified approach to the histologic diagnosis of onychomycosis J Am Acad Dermatol. 2007;57:849–53.
- Gupta AK, Zaman M, Singh J. Diagnosis of Trichophyton rubrum from onychomycotic nail samples using polymerase chain reaction and calcofluor white microscopy. J Am Podiatr Med Assoc 2008;98:224–8.
- Singal A, Khanna D. Onychomycosis diagnosis and treatment. Indian J Dermatol Venereol Leprol 2011;77:659–72.
- Grover C, Khurana A. An update on treatment of onychomycosis. Mycoses. 2012;55:541–551.
- Gupta AK, Schouten JR, Lynch LE. Ciclopirox nail lacquer 8% for the treatment of onychomycosis: A Canadian perspective. Skin Therapy Lett 2005;10:1–3.
- Lauharanta J. Comparative efficacy and safety of amorolfine nail lacquer 2% versus 5% once weekly. Clin Exp Dermatol. 1992;17 Suppl 1:41–3.
- Reinel D, Clarke C. Comparative efficacy and safety of amorolfine nail lacquer 5% in onychomycosis, once-weekly versus twice-weekly. Clin Exp Dermatol. 1992;17 Suppl 1:44–9.
- Baran R, Coquard F. Combination of fluconazole and urea in a nail lacquer for treating onychomycosis. J Dermatolog Treat 2005;16:52–5.
- Hui X, Baker SJ, Wester RC, Barbadillo S, Cashmore AK, Sanders V, et al. In vitro penetration of a novel oxaborole antifungal (AN2690) into the human nail plate. J Pharm Sci 2007;96:2622–31.
- Murdan S. Enhancing the nail permeability of topically applied drugs. Expert Opin Drug Deliv 2008;5:1267–82.
- Duhard E, Coudière P, Voisard JJ, Allaert FA. Management of presumed onychomycosis in private practice. Ann Dermatol Venereol. 2006;1331:11–5.
- Stier DM, Gause D, Joseph WS, Schein JR, Broering JM, Warolin KL, Doyle JJ. Patient satisfaction with oral versus nonoral therapeutic approaches in onychomycosis. J Am Podiatr Med Assoc. 2001;91:521–7.
- Brown SJ. Efficacy of fluconazole for the treatment of onychomycosis. Ann Pharmacother 2009;43:1684–91.
- Scher RK, Breneman D, Rich P, Savin RC, Feingold DS, Konnikov N, et al. Once-weekly fluconazole (150, 300, or 450mg) in the treatment of distal subungual onychomycosis of the toenail. J Am Acad Dermatol 1998;38:S77–86.
- Ling MR, Swinyer LJ, Jarratt MJ, Falo L, Monroe EW, Tharp M, et al. Once weekly fluconazole (450mg) for 4, 6, or 9 months of treatment for distal subungual onychomycosis of the toenail. J Am Acad Dermatol 12 1998; 38:S95–102.
- Srebrnik A, Levtov S, Ben-Ami R, Brenner S. Liver failure and transplantation after itraconazole treatment for toenail onychomycosis. J Eur Acad Dermatol Venereol 2005;19:205–7.
- Havu V, Brandt H, Heikkilä H, Hollmen A, Oksman R, Rantanen T, et al. A double-blind, randomized study comparing itraconazole pulse therapy with continuous dosing for the treatment of toe-nail onychomycosis. Br J Dermatol 1997;136:230–4.
- Sigurgeirsson B, Billstein S, Rantanen T, Ruzicka T, di Fonzo E, Vermeer BJ, et al. L.I.O.N. Study: Efficacy and tolerability of continuous terbinafine (Lamisil) compared to intermittent itraconazole in the treatment of toenail onychomycosis. Lamisil vs. Itraconazole in Onychomycosis. Br J Dermatol 1999;141Suppl 56:5-14.147
- Gupta AK, Ryder JE, Johnson AM. Cumulative meta-analysis of systemic antifungal agents for the treatment of onychomycosis. Br J Dermatol 2004;150:537–44.
- Piraccini BM, Sisti A, Tosti A. Long-term follow-up of toenail onychomycosis caused by dermatophytes after successful treatment with systemic antifungal agents. J Am Acad Dermatol 2010;62:411–4.
- Cribier BJ, Paul C. Long-term efficacy of antifungals in toenail onychomycosis: A critical review. Br J Dermatol 2001;145: 446–52.
- Gupta AK, Lynch LE, Kogan N, Cooper EA. The use of an intermittent terbinafine regimen for the treatment of dermatophyte toenail onychomycosis. J Eur Acad Dermatol Venereol 2009;23:256–62.
- Takahata Y, Hiruma M, Shiraki Y, Tokuhisa Y, Sugita T, Muto M. Treatment of dermatophyte onychomycosis with three pulses of terbinafine (500 mg day for a week). Mycoses 2009;52:72–6.
- Nakano N, Hiruma M, Shiraki Y, Chen X, Porgpermdee S, Ikeda S. Combination of pulse therapy with terbinafine tablets and topical terbinafine cream for the treatment of dermatophyte onychomycosis: A pilot study. J Dermatol 2006;33:753–8.
- Sikder AU, Mamun SA, Chowdhury AH, Khan RM, Hoque MM. Study of oral itraconazole and terbinafine pulse therapy in onychomycosis. Mymensingh Med J 2006;15:71–80.
- Chang CH, Young-Xu Y, Kurth T, Orav JE, Chan AK. The safety of oral antifungal treatments for superficial dermatophytosis and onychomycosis: a meta-analysis. Am J Med. 2007;120:791–8.
- Gupta AK, Leonardi C, Stoltz RR, Pierce PF, Conetta B. Ravuconazole onychomycosis group. A phase I/II randomized, double-blind, placebo-controlled, dose ranging study evaluating the efficacy, safety and pharmacokinetics of ravuconazole in the treatment of onychomycosis. JEADV 2005;19: 437–443.
- Elewski B, Pollak R, Ashton S, Rich P, Schlessinger J, Tavakkol A. A randomized, placebo- and active-controlled, parallel-group, multicentre, investigator-blinded study of four treatment regimens of posaconazole in adults with toenail onychomycosis. BrJ Dermatol 2012; 166:389–398.
- Landsman AS, Robbins AH, Angelini PF, Wu CC, Cook J, Oster M, et al. Treatment of mild, moderate, and severe onychomycosis using 870- and 930-nm light exposure. J Am Podiatr Med Assoc 2010; 100: 166–7.
- Treatment of Mild, Moderate, and Severe Onychomycosis Using 870- and 930-nm Light Exposure: Some Follow-up Observations at 270 Days. J Am Podiatr Med Assoc 2012; 102: 169–171.
- Watanabe D, Kawamura C, Masuda Y, Akita Y, Tamada Y, Matsumoto Y. Successful treatment of toenail onychomycosis with photodynamic therapy. Arch Dermatol 2008;144:19–21.
- Lecha M. Amorolfine and itraconazole combination for severe toenail nychomycosis: Results of an open randomized trial in Spain. Br J Dermatol 2001;145 Suppl 60:21-6.
- Baran R, Feuilhade M, Combernale P, Datry A, Goettmann S, Pietrini P, et al. A randomized trial of amorolfine 5% solution nail lacquer combined with oral terbinafine compared with terbinafine alone in the treatment of dermatophytic toenail onychomycoses affecting the matrix region. Br J Dermatol 2000;142:1177–83.
- Malay DS, Yi S, Borowsky P, Downey MS, Mlodzienski AJ. Efficacy of debridement alone versus debridement combined with topical antifungal nail lacquer for the treatment of pedal onychomycosis: A randomized, controlled trial. J Foot Ankle Surg 2009;48:294–308.
- Grover C, Bansal S, Nanda S, Reddy BS, Kumar V. Combination of surgical avulsion and topical therapy for single nail onychomycosis: A randomized controlled trial. Br J Dermatol 2007;157:364–8.
- Ratajczak-Stefańska V. Assessment of mycological and clinical factors on the course and results of treatment of mycotic infections in patients with recurrent onychomycosis. Ann Acad Med Stetin 2003; 49:161–71.
- Meńdez-Tovar LJ, Manzano-Gayosso P, Velásquez-Hernández V, Millan-Chiu B, Hernández-Hernández F, Mondragón-González R, et al. Resistance to azolic compounds in clinical Trichophyton spp. strains. Rev Iberoam Micol 2007; 24: 320–231.
- Baran R, Hay RJ, Garduno JI. Review of antifungal therapy, part II: treatment rationale, including specific patient populations. J Dermatolog Treat. 2008;19:168–75.
- Ginter-Hanselmayer G, Weger W, Smolle J. Onychomycosis: A new emerging infectious disease in childhood population and adolescents. Report on treatment experience with terbinafine and itraconazole in 36 patients. J Eur Acad Dermatol Venereol 2008;22:470–5.
- Gupta AK, Konnikov N, Lynde CW. Single-blind, randomized, prospective study on terbinafine and itraconazole for treatment of dermatophyte toenail onychomycosis in the elderly. J Am Acad Dermatol 2001; 44:479–84.
- Mayser P, Freund V, Budihardja D. Toenail onychomycosis in diabetic patients: Issues and management. Am J Clin Dermatol 2009; 10:211–20.
Introduction
Onychomycosis is not a life-threatening infection, but it poses several clinically significant consequences such as disfigurement, secondary infection, serving as a reservoir of cutaneous and systemic infection, and challenges in therapy. Role of dermatophytes in onychomycosis and their management is comprehensively discussed in Chapter 11. Fungi other than dermatophytes are also isolated from abnormal nails, which include nondermatophytic moulds (NDM) and yeasts. Although there are some controversies, it is generally accepted that they are capable of causing nail diseases. In this chapter we throw light on the mycology and clinical aspects, and also analyze some of the facts related to the management of nondermatophytic mould (NDM) and yeast infections of the nails.
It is difficult to associate NDMs with infection since they are often transient contaminants or colonizers; however, it is now generally believed that some of the environmental moulds are capable of causing not just nail but also hand and foot infections. They may be accountable for significant number of onychomycosis and may outnumber that caused by dermatophytes in certain geographic areas.1 It is difficult to diagnose them with accuracy. It may be more difficult to treat them because their antifungal sensitivity is clearly not understood. Some of these moulds 150are also capable of producing invasive fungal diseases in neutropenic and immune-suppressed patients, and hence their eradication may be essential.2
Yeasts like Candida albicans are associated with onychomycosis generally in the presence of finger nail paronychia. It is also capable of directly invading the nails when there is immune-deficiency as it is seen in with chronic muco-cutaneous candidiasis (Figure 12.1).3
Epidemiology
There seems to be a great geographic variation in the incidence of nondermatophytic onychomycosis infections. NDM are commonly found in nature as saprophytes and plant pathogens. They are not keratolytic, and are capable of causing infection only when there is previous keratin destruction by dermatophytes, trauma, or any other nail disease. Reported incidence of onychomycosis due to NDM is about 1.45 to 17.6% .4 This highly variable incidence depends on the geographical region and the diagnostic criteria used. Some authors have reported incidence as high as 51.6% for nondermatophyte moulds, which is higher than that of dermatophytes (36.3%).1 Over 95% of cases affect toe nails. This may be due to recurrent trauma, local environmental conditions, peripheral vascular disease and slow nail growth.5
Among the causes of onychomycosis due to NDM, Aspergillus species were more frequently isolated than other agents (Figures 12.2A and B).6,7,8 Scopulariopsis brevicaulis has also been reported as a frequent cause of onychomycosis.5 Reported prevalence of onychomycosis caused by Scytalidium spp. was of 0.87%.9 Table 12.1 gives a list of nondermatophytic moulds reported to be a cause of onychomycosis.5, 10, 11, 12
Reported incidence of onychomycosis by yeast is also variable. It could be the second commonest cause of onychomycosis after dermatophytes. However, in one study it was the most frequent cause of onychomycosis accounting for nearly 60%.13
Clinical Features
NDM Onychomycosis
NDM are saprophytic moulds that are present in the soil. There are no specific clinical patterns for onychomycosis caused by NDM, and all patterns as seen with dermatophytic infections are seen with NDM too.5



|
It is difficult to distinguish dermatophytic infections from NDM infections, however, some of the clinical features such as prior history of trauma, absence of Tinea pedis and lack of response to systemic antifungals may suggest possibility of onychomycosis due to NDM. Clinical forms include distal lateral subungual onychomycosis (DLSO), superficial white onychomycosis (SWO), proximal subungual onychomycosis (PSO), and total dystrophic onychomycosis (TDO).
In DLSO nail plate is primarily not affected. Infection begins at the hyponychium, especially at the lateral edges, and then spreads proximally along the nail bed resulting into subungual hyperkeratosis and onycholysis. SWO is rarer than DLSO and in this variety there is direct dorsal surface nail plate invasion with white discoloration and flakiness and onycholysis is rare. PSO is very rare and presence of HIV disease, peripheral vascular disease and diabetes may predispose to this variety of onychomycosis. Nail invasion occurs at the cuticle. Nail near the cuticle becomes yellow-white discolored and destroyed. Any of these varieties eventually may cause TDO. Nondermatophytes that may be associated with DLSO are Scopulariopsis brevicaulis, Aspergillus species, Acremonium species and Fusarium oxysporum, whereas WSO onychomycosis may be caused by Acremonium species, Aspergillus species and Fusarium.10, 14 Nondermatophyte molds such as Scopulariopsis brevicaulis may uncommonly result in cutaneous infections whereas Scytalidium dimidiatum and Scytalidium hyalinum has been reported to cause tinea pedis.15 Other features that are associated with NDM onychomycosis are paronychia, leukonychia, melanonychia and onycholysis.16
Scopulariopsis brevicaulis is more likely to cause DLSO type of infection but PSO type is also reported.4 Almost all cases are associated with toe nail infections and more frequently the great toe nail. Lesion begins as a yellowish discoloration with progressive thickening of lateral nail plate, eventually classical DLSO develops. Presence of peripheral circulatory disorders seems to be an important clinical association with this infection. There are reports of pulmonary cavities, endophthalmitis, pneumonia and endocarditis in association with this mould.2
Aspergillus species are another important cause of NDM onychomycosis. Aspergillus versicolor, Aspergillus flavus, Aspergillus fumigates, Aspergillus alliaceus, Aspergillus terreus, Aspergillus candidus, Aspergillus niger and Aspergillus ochraceusare are the various species that may cause onychomycosis.16 Similar to other mould infections, great toe nail is commonly involved. DSLO and SWO are the two varieties of infections that are seen. Associated features like paronychia, spotted-striate or total leukonychia and dark discoloration (A. niger) are other features that are commonly associated. Rapid progression of the disease is another important feature suggestive of infection by Aspergillus.
Onychomycoses due to Fusarium spp. almost always involve the great toenails. Previously altered nails due to traumatic or other abnormalities, or nails already infected by dermatophytes are more likely to be affected. Immune-compromised hosts are also likely candidates for Fusarium onychomycosis. Fusarium solani has been reported to cause SWO and Fusarium oxysporum to cause distal subungual hyperkeratosis.17
Scytalidium dimidiatum and Scytalidium hyalinum are etiologic agents of plantar, palmar, interdigital and ungual dermatomycoses. Lesions clinically resemble dermatophytoses. Studies have described the role of S. dimidiatum in invasive and subcutaneous infections in immunodepressed patients. Almost all lesions are seen involving the toe nails. Characteristically they produce DLSO type of lesions. Significant number of cases involves the plantar or interdigital skin lesions.9
Yeast Onychomycosis
Unlike nondermatophytic moulds, yeast like Candida albicans has an intimate association with humans and is part of the normal flora of the skin, mucosa and gut. Infection of the nail apparatus 153with yeasts like Candida species may be a consequence of chronic paronychia, secondary candidiasis, distal nail infection, or as a manifestation of chronic mucocutaneous candidiasis.18
Commonest form of candida onychomycosis manifests secondary to paronychia. Chronic paronychia of the fingernails is seen usually in patients with wet occupations. Swelling of the posterior nail folds occur secondary to chronic immersion in water and contact with irritants or allergens. Damage to the cuticle is an important factor in pathogenesis, due to which yeasts and bacteria enter the subcuticular space.18 This combination of inflammation and infection leads to chronic paronychia with subsequent damage to nail matrix followed by proximal nail dystrophy. Secondary candidal onychomycosis occurs in other diseases of the nail apparatus, most notably psoriasis.
Distal nail infection with yeasts is uncommon and it resembles DLSO caused by dermatophytosis or NDM. Almost all patients have peripheral vascular disease. A lesser degree of subungual hyperkeratosis and exclusive fingernail involvement are two distinguishing features of candidial onychomycosis.
Patients with chronic mucocutaneous candidiasis are at risk of developing Candida onychomycosis. It is a rare cause and is seen in immunocompromised patients. There is direct invasion of the nail plate and formation of candidal granuloma. Involvement of whole thickness of the nail results in swelling of the proximal and lateral nail folds until the digit develops a pseudo-clubbing or “chicken drumstick” appearance.10 The mucous membranes are almost always involved in such cases.
Laboratory Diagnosis
Collecting the Nail Specimen and Transport
- The first step of the sample collection process is thorough cleansing of the affected toenails/ fingernails area with alcohol to remove contaminants such as bacteria. When the nail is heavily soiled, first wash with soap and water.19
- Because the sites of invasion and localization of the infection differ in different types of onychomycosis, different approaches, depending on the presumptive diagnosis, are necessary to obtain optimal specimens.10,20 The following collection techniques are recommended.20Type of onychomycosisSpecimen collectedDistal subungual onychomycosisSpecimen from the nail bed where concentration of viable fungi is greatest after clipping the nailProximal subungual onychomycosisA sharp 1 mm or 2 mm serrated curette is used to remove material from the infected proximal nail bed as close to the lunula as possible after cutting the nailWhite superficial onychomycosisA No. 15 scalpel blade or sharp curette can be used to scrape the white area and remove the infected debrisCandida onychomycosisMaterial is obtained from the proximal and lateral nail edgesEndonyx/total dystrophic onychomycosisNail clipping
- The sample is collected on a sterile black filter paper or cardboard folder and neatly folded. The name of the patient, physician name, date and site of collection may be recorded on the pack.
Specimen Analysis
Both direct microscopy and in vitro laboratory culture of sampled material are necessary to definitively identify the etiologic agent. The specimen should be divided into two portions for direct microscopy and culture. Even if the microscopic examination is negative the specimen should be cultured to isolate the microorganism.
Direct Microscopy
Direct microscopy is only a screening test for the presence or absence of the fungi. It may not differentiate between living and dead or identify the mould pathogens. The amount of fungi may be small and the specimen also may be little which may contribute to false negative results at the rate of (5–15%).10 Contrast can be obtained by counterstaining with chitin specific Chlorazol black E which differentiates fungi from cotton or elastic fibers which prevent false positive results. Parker blue-black ink or Lactophenol cotton blue can also be used to provide contrast but they are not chitin specific.
Nail plate clippings may be sent for histopathologic evaluation to differentiate nail dystrophy by onychomycosis, psoriasis, or lichen planus. Periodic Acid Schiff (PAS) stain is used for the analysis. The test has very high sensitivity, and may also help to observe the depth of tissue invasion, type of mould (whether dermatophyte or nondermatophyte) to some extent.21 Grocott methanamine silver stain and Calcoflour white stain yield better results.
Culture
In case of onychomycosis, culture helps to identify the causative microorganism. As the nails are nonsterile, fungal and bacterial contaminants may overgrow the real pathogen. Usually the specimens are cultured on two different media. One will be selective for dermatophyte and the other which allows the growth of dermatophyte and nondermatophyte. Cycloheximide inhibits the growth of nondermatophyte fungi. Specimen is always cultured on media containing cycloheximide and also without them. Commonly used media are Sabouraud dextrose agar with or without antibiotics like gentamicin or chloramphenicol and Littman's oxgall medium. If the growth occurs on both types of media then it is dermatophyte but if growth occurs only on cycloheximide free medium then it is likely to be nondermatophytic moulds (NDM). The NDM grow much faster, within one week. The yeast like Candida grows within 48 hours of incubation. Grams stain of the culture grown, germ tube test, chlamydospore formation test, culturing on Chromagar may help to speciate the Candida grown. The dilemma for laboratory personnel in reporting a nondermatophyte as a causative agent of onychomycosis is because these fungi are also laboratory contaminants. Dermatophytes, if isolated, should be considered as pathogens. If NDM is isolated, it should be considered as laboratory contaminants unless KOH or microscopy demonstrates atypical frond-like hyphae or if the same organism is repeatedly isolated.10 Gupta, AK et al suggested an inoculum counting (Walshe and English criteria) in clinical diagnosis of onychomycosis caused by nondermatophytic filamentous fungi.22
O ther Tests
In case of research laboratories DNA based tests like PCR RFLP are used for epidemiological and confirmation purposes. Immunohistochemistry and dual flow cytometry have been used to identify mixed infections and for quantification of the fungal load.155
Treatment
Onychomycosis is a cosmetic problem, and it may have a negative physical and psychological impact on afflicted persons. It may also serve as a reservoir for systemic infections and communicate the fungal infections to family members. There are no uniform guidelines on when to treat onychomycosis and decision should be taken on case to case basis. Irrespective of cause of onychomycosis, therapeutic outcome is generally not satisfactory.
Both topical and systemic therapies are available for the therapy of onychomycosis. Many published reports do not highlight the cause of onychomycosis prior to therapy. Systemic therapy scores over topical therapy because the penetration of topical antifungals is unpredictable with nail diseases. Topical therapy can only be used in SWO and possibly in early DLSO, or when systemic therapy is contraindicated on medical or other grounds.18
For onychomycosis caused by Candida or nondermatophyte moulds, there is no single superior systemic therapy. Combination of drugs with oral itraconazole or terbinafine may be useful in all nondermatophyte mould infections.23 The in vitro activity of terbinafine is superior to itraconazole against various species of Aspergillus.16 Itraconazole and terbinafine have demonstrated efficacy and safety against some cases of S. brevicaulis toe onychomycosis.24 Griseofulvin is ineffective against toe onychomycosis caused by S. brevicaulis. Ketoconazole is not recommended by many for toe onychomycosis given its potential for adverse effects. Fluconazole is less effective than terbinafine and itraconazole in the treatment of onychomycosis, but it is a choice when patients do not tolerate other oral antifungal agents.25 Minimal dosing of fluconazole should be 150 mg per week for at least 6 months. Candida responds to treatment with itraconazole and fluconazole. Addition of amorolfine to oral itraconazole pulse therapy is beneficial in the treatment of Candida fingernail onychomycosis.26
Topical treatment with terbinafine (with nail avulsion) or ciclopirox can be successful in the treatment of onychomycosis caused by S. brevicaulis, Fusarium sp., and Acremonium sp.23 Ciclopirox may have a broad antimicrobial profile including dermatophytes, yeasts and nondermatophytes, and activity of ciclopirox and terbinafine suggests many instances of synergy or additivism.27 Amorolfine is a structurally unique, topical antifungal agent, which possesses both fungistatic and fungicidal activity against dermatophyte, dimorphic, some dematiaceous and filamentous fungi, and some yeast. Application of amorolfine 5% nail lacquer once or twice weekly for up to 6 months produced mycological and clinical cure in approximately 40 to 55% of patients with mild onychomycosis.28.
Therapy in case of onychomycosis involves two end points namely mycological cure and clinical cure. Successful eradication of fungus (mycological cure) with therapy is not necessarily associated with clinical improvement or normalization of structure of nail (clinical cure). This is especially true with respect to yeast and NDM infections because nails are very often traumatized or dystrophic prior to the treatment and such defects may be permanent. This aspect has to be clearly informed to the patients before a decision on treatment be taken.
References
- Ungpakorn R, Lohaprathan S, Reangchainam S. Prevalence of foot diseases in outpatients attending the Institute of Dermatology, Bangkok, Thailand. Clin Exp Dermatol. 2004;29(1):87–90.
- Kirkpatrick CH. Chronic mucocutaneous candidiasis. Pediatr Infect Dis J. 2001;20(2):197–206.
- Hwang SM, Suh MK, Ha GY. Onychomycosis due to nondermatophytic molds. Ann Dermatol. 2012;24(2):175–80.
- Bonifaz A, Cruz-Aguilar P, Ponce RM. Onychomycosis by molds. Report of 78 cases. Eur J Dermatol. 2007 Jan-Feb;17(1):70–2.
- Bassiri-Jahromi S, Khaksar AA. Nondermatophytic moulds as a causative agent of onychomycosis in tehran. Indian J Dermatol. 2010;55(2):140–3.
- Hilmioglu-Polat S, Metin DY, Inci R, Dereli T, Kilinç I, Tümbay E. Non-dermatophytic molds as agents of onychomycosis in Izmir, Turkey - a prospective study. Mycopathologia. 2005;160(2):125–8.
- Ramani R, Srinivas CR, Ramani A, Kumari TG, Shivananda PG. Molds in onychomycosis. J Int Dermatol. 1993;32(12):877–8.
- Xavier AP, Oliveira JC, Ribeiro VL, Souza MA. Epidemiological aspects of patients with ungual and cutaneous lesions caused by Scytalidium spp. An Bras Dermatol. 2010;85(6):805–10.
- Elewski BE. Onychomycosis: pathogenesis, diagnosis, and management. Clin Microbiol Rev. 1998;11(3):415–29.
- Escobar ML, Carmona-Fonseca J. Onychomycosis by common non-dermatophyte moulds. Rev Iberoam Micol. 2003;20(1):6–10.
- Van Esbroeck M, Wuytack C, Van Looveren K, Swinne D. Isolation of Onychocola canadensis from four cases of onychomycosis in Belgium. Acta Clin Belg. 2003;58(3):190–2.
- Hashemi SJ, Gerami M, Zibafar E, Daei M, Moazeni M, Nasrollahi A. Onychomycosis in Tehran: mycological study of 504 patients. Mycoses. 2010;53(3):251–5.
- Gupta AK, Elewski BE. Nondermatophyte causes of onychomycosis and superficial mycoses. Curr Top Med Mycol. 1996;7(1):87–97.
- Romano C, Valenti L, Difonzo EM. Two cases of tinea pedis caused by Scytalidium hyalinum. J Eur Acad Dermatol Venereol. 1999;12(1):38–42.
- Gianni C, Romano C. Clinical and Histological Aspects of Toenail Onychomycosis caused by Aspergillus spp.: 34 Cases Treated with Weekly Intermittent Terbinafine. Dermatology. 2004;209(2):104–10.
- Godoy P, Nunes E, Silva V, Tomimori-Yamashita J, Zaror L, Fischman O. Onychomycosis caused by Fusarium solani and Fusarium oxysporum in São Paulo, Brazil. Mycopathologia. 2004;157(3):287–90.
- Roberts DT, Taylor WD, Boyle J. Guidelines for treatment of onychomycosis. Br J Dermatol. 2003;148(3):402–10.
- Ghannoum Mahmoud A, Isham Nancy C. Chapter 16: Dermatophytes and dermatophytoses Anaissie Elias J, McGinnis Micheal R, Pfaller Micheal A (Eds). Clinical Mycology, 2nd edition, Churchill Livingstone, Elsevier; 2009 p 375-384.
- Shenoy MM, Teerthanath S, Karnaker VK, Girisha BS, Krishna Prasad MS, Pinto J. Comparison of potassium hydroxide mount and mycological culture with histopathologic examination using periodic acid-Schiff staining of the nail clippings in the diagnosis ofonychomycosis. Indian J Dermatol Venereol Leprol. 2008;74(3):226–9.
- Gupta AK, Cooper EA, MacDonald P, Summerbell RC. Utility of inoculum counting (Walshe and English criteria) in clinical diagnosis of onychomycosis caused by nondermatophytic filamentous fungi. J Clin Microbiol. 2001;39(6):2115–21.
- Singal A, Khanna D. Onychomycosis: Diagnosis and management. Indian J Dermatol Venereol Leprol. 2011;77(6):659–72.
- Gupta AK, Gregurek-Novak T. Efficacy of itraconazole, terbinafine, fluconazole, griseofulvin and ketoconazole in the treatment of Scopulariopsis brevicaulis causing onychomycosis of the toes. Dermatology. 2001;202(3):235–8.
- Brown SJ. Efficacy of fluconazole for the treatment of onychomycosis. Ann Pharmacother. 2009;43(10):1684–91.
- Rigopoulos D, Katoulis AC, Ioannides D, Georgala S, Kalogeromitros D, Bolbasis I, Karistinou A, Christofidou E, Polydorou D, Balkou P, Fragouli E, Katsambas AD. A randomized trial of amorolfine 5% solution nail lacquer in association with itraconazole pulse therapy compared with itraconazole alone in the treatment of Candida fingernail onychomycosis. Br J Dermatol. 2003;149(1):151–6.
- Gupta AK, Kohli Y. In vitro susceptibility testing of ciclopirox, terbinafine, ketoconazole and itraconazole against dermatophytes and nondermatophytes, and in vitro evaluation of combination antifungal activity. Br J Dermatol. 2003;149(2):296–305.
- Haria M, Bryson HM. Amorolfine. A review of its pharmacological properties and therapeutic potential in the treatment of onychomycosis and other superficial fungal infections. Drugs. 1995;49(1):103–20.
Definition
Paronychia is a common disorder and is defined as an inflammation of tissue surrounding the nail plate.
Epidemiology
It is the most frequent of hand infections: 35% of hand infections are said to be due to paronychia. The female to male ratio is 3:1. Adults suffer more than children, save thumb-suckers. Finger nails are more frequently involved than toe nails.
Classification
Depending on the Clinical Duration
- Chronic: More than six weeks.
- Acute paronychia: Less than six weeks.
Depending on the Etiology
Infectious
Primary or secondary
- Acute bacterial:
- Gram positive:
- Staph. aureus
- Streptococci
- Gram negative: Pseudomonas, E. coli and other related gut flora
- Anaerobes
- Mixed
- Fungal: Candida, dermatophytes, moulds
- Viral: Herpes, warts (Figure 13.1)
- Parasitic
- Mycobacterial
Non-infectious Causes
- Chemicals: Commonly industrial workers
- Allergic: Agents causing allergic contact dermatitis of hands (Figure 13.2)
- Mechanical: Artificial nails, tight footwear
- Hallux deformity: Extremely rare
- Neoplastic: Extremely rare
Etiopathogenesis
The nail is longitudinally supported by two lateral folds or peronychium. Proximally, it is covered by the eponychium. Distal to the peronychium, the region immediately below the free edge of the nail is the hyponychium. The hyponychium serves as a tough physical barrier that resists bacterial infection.


|

Any breach in the continuity of any of the barriers of lateral, proximal nail folds would potentially be a risk factor to cause paronychia.
Predisposing Factors
- Commonly seen in lateral fold are—Cracks, fissure or trauma, improper manicure/pedicure, ingrown toe nail (Figure 13.4)
- Pre-existing dermatitis (Figure 13.5 to 13.8)
- Frequent nail biters or thumb-suckers (Figure 13.9 and 13.10)
- Anemia
- Occupational circumstances (vide supra)
- Immunosuppression: Diabetes/HIV/Drugs-corticosteroids, immunosuppressive drugs (Figures 13.11 and 13.12).











Clinical Features
Acute Paronychia
Common in lateral nail folds, often follow trivial cracks, fissures or trauma.
Erythema, edema and tenderness are the hallmark of acute paronychia (Figure 13.13). If neglected, it could rapidly lead to paronychial suppuration (Figure 13.14), presenting as fluctant swelling, abscess and may even result in digital cellulitis.
The digital pressure test: Pressure is applied to the palmar surface of the distal finger. The area of the abscess will blanch with palmar pressure.
Chronic Paronychia
Most commonly affects index and thumb nails of adult females. Housewives, nurses and bartenders, who frequently soak their nails in water, are predisposed. The amount of inflammation is slight to moderate, following repetitive injury. The cuticles are typically hyperkeratotic and there is a boggy swelling all around the nail, which is minimally painful. Involvement of germinal matrix may result in secondary nail changes including pitting, dystrophy, deformity and discoloration (Figures 13.15 and 13.16).
Candida albicans is the most frequently implicated organism; less common being the pseudomonas and staphylococcal species. The source of candida organisms may be from intertrigo or vaginitis, often carried via nails due to inadequate personal hygiene. Moisture, warmth and friction often contribute to perpetuation of the inflammation.
However, actual microbiological documentation of finding candida species from the paronychias may not be readily be established in many of the cases. It is speculated that hypersensitivity to candida might be a reason behind persistent inflammation. Thus, the cause of chronic paronychia, can be best considered as multifactorial.
Differential Diagnosis
- Felon: Thumb and index fingers are more predisposed. Digital pulp space is affected and the infection is deep-seated than simple paronychia. Severe tenderness and swelling is marked.Suppuration is compartmentalized and self-drainage may not occur easily. Therefore, procedural drainage is often required and involving deep surgical dissection of the pulp space.
- Herpetic Whitlow: It is often misdiagnosed in the initial phase, especially if seen after a few days of onset. Recurrent vesicular eruptions, which may rapidly cause erosions should serve as a clue.
- Contact Dermatitis: History of contact preceding the onset of each episode clinches the diagnosis.
- Drug Rash: Fixed drug eruption may involve fingers, presenting as paronychia. Typical clinical appearance is of an erythematous rim with bluish pink center; may cause bullous eruption.


Complications
Suppuration leading to abscess, cellulitis, felon, suppurative tenosynovitis and rarely, osteomyelitis of the underlying phalangeal bone.
Investigations
- Complete blood counts: Anemia
- Blood sugar
- Serological tests for HIV
- Gram stain/KOH: Cutaneous candidiasis
- Patch test: Contact dermatitis
- Tzanck smear: Herpes whitlow; differentiates from pompholyx
- Onychomycosis: Fungal scraping or nail clipping
Treatment of Acute Paronychia
- Thorough cleansing with soap and running (tap) water may suffice in minor wounds
- Warm soaks can be used 3 or 4 times a day for acute paronychia to promote drainage and relieve some of the pain
- Antibiotics: Cephalexin/ampicillin+cloxacillin/Co-amoxi-clav
- NSAIDs
- Topical antibiotics: Mupirocin/Fucidic acid
- If it does not subside, surgical drainage may be required
- Surgical drainage: Actual surgical incision is generally not required. The fluctuant swelling needs only separation from cuticle by blunt scalpel (directed away from the nail plate) in most cases. Complete surgical nail removal for suppurative paronychia is generally discouraged.
Treatment of Chronic Paronychia
Avoidance of predisposing factors such as chemicals with potential allergens and irritants, avoidance of repetitive trauma to nail, and elimination of chronic immersion of hands into water. Protection by wearing gloves helps to achieve dry milieu within the eponychial space, thus facilitating reduction in inflammation.
A combination of topical steroids and antifungal often helps. Systemic antifungals such as fluconazole, itroconazole, though are a popular medication for eradication of candida, may not be necessary. Antibiotics may be required for control of secondary bacterial infection.
Surgical therapy may be required if medical therapy does not produce the desired results.
Eponychial marsupialization technique with nail plate removal has produced excellent response as per one study.
Unresponsive Chronic Paronychias
Those patients of chronic paronychia, who are not responsive to adequate medical therapy should be evaluated for underlying systemic diseases such as neoplastic disease.
Tumors such as squamous cell carcinoma and malignant melanoma, cysts, syphilitic chancres, warts or foreign body granulomas can occasionally mimic a chronic paronychia.
Treatment Pearls for Chronic Paronychia
- Usage of 4% thymol solution serves well for drying but may be irritant.
- Potent topical steroids along with topical antibiotics for short duration is often relieving.
- Self-retaining long finger polyvinyl sleeves are commercially available.
- Touch up with 20–50% carbolic acid may improve healing.
Summary
References
- Rockwell P. Acute and chronic paronychia. Am fam phy 2001; 63: 6. 113-6.
- Rich P. Nail disorders. Diagnosis and treatment of infectious, inflammatory, and neoplastic nail conditions. Med Clin North Am 1998;82:1171-83,vii.
- Brook I. Aerobic and anaerobic microbiology of paronychia. Ann Emerg Med 1990;19:994–6.
- Brook I. Aerobic and anaerobic microbiology of paronychia. Ann Emerg Med 1990;19: 994–6.
- Jebson PJ. Infections of the fingertip. Paronychias and felons. Hand Clin 1998; 14:547-55,viii.
- Brook I. Paronychia: a mixed infection. Microbiology and management. J Hand Surg [Br] 1993;18:358–9.
- Canales FL, Newmeyer WL 3d, Kilgore ES. The treatment of felons and paronychias. Hand Clin 1989;5:515–23.
- Lee TC. The office treatment of simple paronychias and ganglions. Med Times 1981;109:49-51,54-5.
- Jules KT, Bonar PL. Nail infections. Clin Podiatr Med Surg 1989;6:403–16.
- Lane LB, Bednar C. Eponychial marsupialization and nail removal for surgical treatment of chronic paronychia. J Hand Surg Am. 1991 Mar;16(2):314–7.
A tumor is described as a circumscribed swelling, which may or may not be a true cellular proliferation. Hence, many degenerative, reactive or ‘pseudo’ lesions may be classified as tumors, apart from the true neoplasms. The true nature of a tumor generally requires histopathological confirmation and subsequent management.
The nail unit is a very vascular structure, which is a very common site for many ‘tumors’. Irrespective of the underlying pathology, the clinical presentations tend to overlap with only subtle differences in their clinical features. Nail unit tumors (NUT) are frequently misdiagnosed or diagnosed at a later stage because the nail plate can cover any underlying lesion/tumor simulating an inflammatory or infectious disease. NUT can be classified as benign, malignant, or metastatic. Almost, any portion of the nail apparatus can be affected except the nail plate, although it is often distorted/destroyed secondary to many tumors.1 Usually, there is involvement of a single digit. The clinical appearance alone may not yield a diagnosis in most of the cases, and appropriate histopathological and radiological investigations are required. Among these, magnetic resonance imaging (MRI) has emerged as the most useful modality in assessment of nail unit tumors, although simpler modalities like X-ray, ultrasound (USG) or computerised tomography (CT) may be of help in select cases. This chapter aims at reviewing the commonly encountered NUT.170
The nail unit tumors may be classified as benign, benign but aggressive (resulting in nail destruction) or malignant.
Benign Tumors
Verrucae
Warts are the most commonly seen tumors of the nail unit. They affect fingernails more than toenails. Children and teenagers are the most commonly affected age group; with maximum cases occurring in the age spectrum of 12 to 16 years.2 Nail biters are quite commonly affected. Certain occupations also predispose to higher chances of development of periungual warts, including butchers and those involved in a lot of wet work. It has been seen that up to 23% of handlers of meat, fish, and poultry develop periungual warts (Butchers’ warts).3 Human papillomavirus (HPV) types most often implicated in periungual warts are types 1, 2 and 4.4 Butcher's warts are most commonly produced by HPV types 2 and 7. Clinically apparent lesions generally develop a few weeks to more than a year after inoculation.
Clinically, warts present as rough hyperkeratotic papules. The lesion commonly starts from the lateral or proximal nail fold or the hyponychium and goes on to involve the nail bed thereon (Figure 14.1). Although warts do not directly affect the nail matrix, they may produce slight matricial damage due to compression, resulting in nail plate ridging and grooving.2 Warts may also present as foci of onycholysis resulting from a subungual wart (Figure 14.2), which may be diffuse or a linear onycholytic band with splinter hemorrhages. Pain may be a symptom in subungual warts.2 Complications resulting from nail unit verrucae include occasional bony erosions, spread to other areas and rarely development of Bowen's disease and squamous cell carcinoma (in long standing cases).2 Differential diagnosis includes onychophosis affecting a lateral fold of the toenails, subungual filamentous tumor, subungual vegetations of amyloidosis, subungual corn (heloma), verrucous epidermal nevus, inflammatory linear verrucous epidermal nevus, and multicentric reticulohistiocytosis.5

Figure 14.1: A young boy with multiple warts over the hand, arising in the periungual location and invading under the nail bed

The diagnosis can be confirmed with histopathology which shows a sharply demarcated epithelial hyperplasia with acanthosis, papillomatosis, and hyperkeratosis with areas of parakeratosis. The granular layer shows vacuolated cells containing typical basophilic inclusions. The dermal papillae are thin and elongated and contain blood vessels that project into the wart. Radiological investigations are generally not required.
Treatment of nail unit warts is often frustrating with low cure rates and high recurrences seen with most forms of therapy. However, many periungual warts may undergo spontaneous resolution, especially in children. It has been reported that 25% lesions may disappear spontaneously within 6 months and 65% within 2 years.6 Spontaneous resolution is less frequent for HPV-2-induced mosaic warts, for large and long-standing warts, and for warts in immunocompromised patients.7
Topical treatment options combined with keratolytics should be considered as the first line of intervention, especially in cases with limited involvement. Salicylic acid in concentrations of 10-60% may be used, often in combination with lactic acid. Similar results have been produced by glutaraldehyde and formaldehyde, which act by producing skin desiccation with viral destruction.8 Strong topical sensitizers like squaric acid dibutylester (SADBE) or diphenylcyclopropenone (DFC) have been used for treatment of multiple warts. 2% SADBE or DFC in acetone base is used for sensitization. After 21 days, weekly applications are carried out with dilutions ranging from 0.001 to 1% according to the patient's response. The aim is to produce a mild contact dermatitis.9 Imiquomod is another potential agent which may be used for periungual warts. Intralesional injections of bleomycin are an effective modality of treatment. Under local anesthesia, the bleomycin solution (1 U/mL of sterile saline) is dropped on the wart surface. Using a disposable needle, the wart is then punctured approximately 40 times per 5 mm2 area.10 The wart slowly undergoes necrosis with formation of an eschar that can be scraped away 3–4 weeks after treatment.10
Surgical treatment may be required in selective cases. Cryotherapy for 10–15 seconds, after paring off the hyperkeratotic part, may be performed. Complications may occur due to the concurrent matrix damage and manifest as leukonychia, Beau's lines, and onychomadesis.11 Surgical excision is associated with a high-risk of recurrence. Electrosurgery may produce 172considerable scarring. CO2 laser (1–2 sessions) has been reported to produce complete cure in 71% of patients with periungual warts, treated exclusively with this modality.12 However, temporary or permanent nail dystrophy may develop and the procedure should be restricted to very recalcitrant warts. Er-YAG laser has a similar mechanism of action and has produced good results. Pulsed dye laser (PDL) acts through a selective microvascular destruction of the dilated capillaries of the warts, as the oxyhemoglobin in the vessels preferentially absorbs yellow light.13 Resolution of the wart occurs both due to thermal damage and the removal of blood supply. Stimulation of a cell-mediated immune response may be another contributing factor. The treated lesion turns dry and black due to the associated necrosis and healing is expected to occur over 2–4 weeks. However, periungual warts are less responsive to treatment as compared to palmar or common warts. Although this technique is associated with a very low incidence of scarring, cure after two to four treatments can be expected in only one-third of the cases.13
Onychomatricoma
This neoplasm is a relatively newly described entity, first described about 2 decades ago. It is considered to be a benign NUT. Onychomatricoma is generally considered a form of fibroma of the proximal nail fold, closely associated with the matrix. It presents with a combination of three main clinical signs which may be striking enough to make a diagnosis or at least to arouse suspicion. These include a yellow longitudinal band of variable width, leaving a single or double portion of normal pink nail on either side; tendency toward transverse overcurvature of the affected nail portion, which becomes more pronounced as the yellow color is more extended; and on avulsion, the proximal aspect of the nail reveals multiple honeycomb channels corresponding to the villous tumoral outgrowths emanating from the matrix.5 Although the tumor is asymptomatic, there may be very extensive villous projections occasionally; producing bleeding upon cutting the nails.14 Less classically, the affected nail may present in the form of melanonychia or a presentation similar to onychomycosis.15
Radiological imaging is of use in preoperative diagnosis of the tumor. MRI images are typical, highlighting the tumoral core in the matrix area and the invagination of the lesion into the funnel- shaped nail plate, in sagittal sections. Axial slices accurately show the holes in the substance of the nail plate, filled with the digitations.5 Histologically, the tumor is characterized by multiple fibroepithelial projections that extend into the thickened nail plate. The tumor epithelium is identical to that of the normal nail matrix and keratinizes without a granular layer.16
Treatment involves excision of the tumour in toto. The proximal nail fold may have to be pulled back to expose the entire extent of the mass before complete excision can be carried out. The lesion is apparently benign; however, it is subject to recurrence. Long-term follow-up is recommended. The risk of conversion to malignancy is not known.
Glomus Tumor
Glomus tumor is a benign vascular tumor, arising from neuromyoarterial glomus bodies. Approximately 75% of glomus tumors occur in the hand, especially in the fingertips and in particular in the subungual area, and 1% to 2% of all hand tumors are glomus tumors.17 These tumors generally present with severe pulsating pain, which may be spontaneous or provoked by the slightest trauma and temperature change (especially warm to cold). Pain may be worst at night and may refer to the shoulder when severe. The classical triad of temperature, cold sensitivity and severe pain is present in 63–100% of patients.18173
Clinically, the objective signs depend on the site of involvement of the nail unit. Nail matrix tumors cause splitting and distortion of the nail plate whereas the nail bed lesions may appear as bluish or red foci, 1–5 mm in diameter, beneath the nail (Figure 14.3). This erythematous focus does not blanch with pressure and is associated with excruciating pain on pressure.5 About half of these tumors cause a depression on the dorsal aspect of the distal phalangeal bone, visible on radiographic study.19 However, intraosseous location is unusual.
Confirming the diagnosis of a glomus tumor is challenging and it rests on a high degree of clinical suspicion. Useful clinical tests which help in confirming the suspicion, include Hildreth's sign (a blood pressure cuff inflated proximally abolishes the pain)20 and Love's sign (helps in localization of tumor; done by applying pressure to the suspected area with the head of a pin, which will elicit intense pain).21 A plain skiagram may reveal bony erosion in only 1/3rd of the cases. Doppler USG has been reported to be useful in confirming the diagnosis. Recently, MRI has emerged as a useful modality in imaging of glomus tumors. MRI can reveal the exact location, extent and size of the tumour. However, lesions less than 3 mm in size may be missed. A preoperative imaging is highly advisable to assess for synchronous lesions. magnetic resonance imaging can also be used to evaluate for residual tumors.15
Histology provides definitive confirmation of the diagnosis as it reveals vascular channels lined with endothelium and cuboidal glomus cells. These cells have dark nuclei and pale cytoplasm. Myelinated and nonmyelinated nerves are found, which may account for the associated symptoms.15 Immunohistochemistry shows positivity for Vimentin, a 42-kD muscle Actin (with HHF 35), a smooth muscle Actin (CGA 7), and Myosin, but absence of Desmin, Factor VIII-related antigen, and several neural markers.20
Treatment involves complete excision of the tumor. Pain may take time to disappear following the excision. Recurrence can develop in 10–20% cases and may be the result of incomplete excision, an overlooked tumor at the initial operation, or newly developed tumors.5

Figure 14.3: A subungual glomus tumor, presenting as an intensely painful nail. The underlying, ill-defined focus of reddish discoloration can be clearly seen. Distally, the nails are dyed with henna
Pyogenic Granuloma (PG)
It is also known as granuloma telangiectaticum, granuloma pediculatum or lobular capillary hemangioma. Pyogenic granuloma is a benign vascular tumor, presenting as a rapidly evolving, solitary, sessile or polypoid vascular nodule, most commonly seen the hands (especially fingers), the feet, lips, face, upper trunk and the mucosal surfaces of the mouth and perianal area.23 In 174the nail unit, pyogenic granuloma generally arises in the nail folds (Figure 14.4). Sometimes it may be subungual when arising from the nail matrix. In this location, it is generally associated with onycholysis. The lesion has a prominent collarette at the base and is often tender. Bleeding occurs with minor trauma and causes much patient morbidity. Pain is generally absent except when the lesion becomes infected.
The exact etiopathogenesis is unknown. It is believed to be a reactive hyperproliferative vascular response to a variety of stimuli, such as infective organisms, penetrating injury, hormonal factors and drugs.24 Several drugs have been reported to produce PG's involving the nail apparatus. These include indinavir, retinoids, ciclosporine, lamivudine, capecitabine and cetuximab.25–29 Extensive tissue granulation caused by an ingrown toenail may mimic a periungual PG.
Diagnosis is generally clinically apparent; however, differentiation from other benign and malignant tumors (especially cavernous angioma, pseudopyogenic granuloma, hemangiosarcoma, amelanotic melanoma, Spitz nevus or metastatic tumors) may become difficult at times. Histological examination shows proliferation of blood capillaries with a radiating pattern set in a loose edematous collagenous matrix.24 The epidermis shows inward growth at the base of the lesion, producing an epidermal collarette and causing in some cases slight pedunculation of the lesion. A dermal mixed inflammatory infiltrate is a common finding. Older pyogenic granulomas tend to organize and partly fibrose with fibrous septa intersecting the lesion and producing a lobular pattern.24 Recently, dermoscopy has been studied as a diagnostic tool for the diagnosis of this disorder. A reddish homogeneous area surrounded by a white collarette was seen most frequently.24 Importantly, there is absence of known dermoscopic signs of other tumors.
Therapy should be as simple as possible to avoid disfiguring scars or nail deformity. Treatment failure and local recurrence of the lesion is a problem with all treatment methods. The lesion may be removed by excision at its base followed by electrodesiccation or application of Monsel's or aluminum chloride solution.5 The use of argon, CO2, and 585 nm flashlamp-pumped pulsed dye lasers has also been described.31

Figure 14.4: A nail unit pyogenic granuloma, arising from underneath the proximal nail fold and sitting on the nail plate surface. The tumor bleeds profusely
Exostosis
Subungual exostoses are the most common benign bony proliferations associated with the nail unit.16 They present as bony outgrowths, most commonly on the dorsomedial aspect of the tip 175of great toe (Figure 14.5). The lesions generally develop after trauma, are painful on pressure and often produce onycholysis and nail deformity. The triad of pain (the leading symptom), nail deformation, and radiographic features is usually diagnostic.5 Multiple exostoses are generally inherited in an autosomal dominant pattern and are attributable to mutations of the EXT1 and EXT2 genes on chromosomes 8q and 11p, respectively.32
On radiography, exostoses are seen as an ill-defined trabeculated osseous growths with an expanded distal portion covered with radiolucent fibrocartilage.5 A subungual osteochondroma, which presents with similar signs and symptoms, may be differentiated by the presence of hyaline cartilage instead of fibrocartilage. However, an absolute distinction between the two lesions may not be possible.
Treatment consists of local curettage and excision of the excess bone.

Pseudomyxoid Cysts
It is a relatively commonly seen tumor which is termed as a ‘pseudocyst’ because the cellular cyst wall can seldom be demonstrated.15 Pseudomyxoid cysts are most commonly seen in middle-aged women. They are generally located in the proximal nail fold of the fingernails. They appear as small soft nodules which often drain a viscous jelly-like fluid, spontaneously or on mild trauma.15 The lesion may produce pressure on the nail matrix leading to nail plate depression and grooves. Another common location is subungual where these cysts may connect to the distal interphalangeal joint by a tract. Osteoarthritis of the distal interphalangeal joint is a frequent association.16 MRI permits identification of the cyst in doubtful cases.16
Treatment includes incision and drainage; intralesional sclerosant; intralesional steroid injection; cryosurgery; laser and infrared photocoagulation. There is a high relapse rate after single treatments with less invasive therapies.15
Fibrous Tumors
Fibromas are a common occurrence in and around the nail unit. Various types of lesions have been described. Koenen's periungual fibromas develop in about 50% of the cases of tuberous sclerosis.16 Individual tumors are small, round, flesh colored, and asymptomatic, with a smooth surface (Figure 14.6). The tip of the tumor may be slightly hyperkeratotic, resembling a fibrokeratoma. These lesions tend to grow out of the proximal or lateral nail fold, eventually 176overgrowing the nail bed and destroying the nail plate. Depending on their location, they may cause longitudinal depressions in the nail plate. They are sometimes also seen to grow into the nail plate.

Figure 14.6: A patient of tuberous sclerosis with Koenen's tumor. The patient also had adenoma sebaceum and ash leaf macules
Acquired ungual fibrokeratoma is a fibroepithelial growth of unknown origin, which presents more commonly in men. Trauma is believed to play an important role in their development. These tumors are generally seen as pinkish, asymptomatic nodules with a hyperkeratotic tip and a narrow base. They occur mostly in the periungual area or elsewhere on the fingers. Most ungual fibrokeratomas emerge from beneath the proximal nail fold, growing on the dorsum of the nail where they cause a sharp longitudinal depression (Figure 14.7). Some of these lesions originate from within the matrix and thus grow in the nail plate, eventually to emerge in the middle of the nail. Such intraungual fibrokeratomas are also called “dissecting ungual fibrokeratoma” because they divide the nail plate into two.33 Subungual fibrokeratomas arising from the nail bed are rare.
Imaging is required before planning any surgical intervention. MRI is the most useful modality of investigation for these tumors. Treatment is by complete excision of the tumor.

Figure 14.7: An acquired digital fibrokeratoma, presenting on the thumb nail. Perionychial mild inflammation can be appreciated
Implantation Epidermis Cyst
Implantation epidermis cyst generally present as gradual enlargement of the tip of the digit, mimicking the appearance of clubbing, or pincer nail.15 Pain may arise due to involvement of the underlying bone, producing erosion or distortion of cortical structure. Suggestive changes may be seen on X-ray and a cyst may be more clearly demarcated on MRI. There is sometimes a history of previous trauma or surgery. Surgical excision of the cyst is generally curative.15
Malignant/Premalignant Tumors
The malignant tumors of the nail unit are essentially the same as those affecting the skin and include basal cell carcinoma (BCC), squamous cell carcinoma (SCC) and malignant melanoma (MM). However, the clinical presentation and the behavior of these NUT's are often different from their cutaneous counterparts. A high level of suspicion is required for an early diagnosis of these lesions.
Bowen's Disease
Bowen's disease of the nail is uncommon and is seen most frequently in middle-aged men.15 It presents as a periungual or subungual verrucous lesion that may ulcerate. Inflammation and crusting are common, as is longitudinal melanonychia. Predisposing factors include HPV infection (especially HPV16) and chronic X-ray exposure.34
Squamous Cell Carcinoma (SCC)
This is the most common malignant tumor of the nail unit. In a large retrospective study by Nguez-Cherit et al, SCC appeared as the sixth most common nail tumor.1 The etiology of this tumor remains controversial, with possible contribution of HPV infection (especially HPV type 16) and UV radiation.35,36 HPV-34 and 35 have also been reported to be associated with clinically apparent lesions of SCC.37 A possible role of anogenital transmission of HPV is suggested, with similar HPV genomes being found at the two sites.
The tumor affects fingers more than toes. It presents as a slow growing periungual or subungual nodule that ulcerates and bleeds. Paronychia is commonly associated. Subungual lesions produce onycholysis and nail plate destruction (Figure 14.8). The initial presentation may be as a verrucous lesion appearing like a viral wart, adding to diagnostic confusion.35 Systemic metastases or death from SCC of nail is extremely rare.
The diagnosis can be confirmed by biopsy. An invasive SCC will show cords of polygonal cells, with eosinophilic cytoplasm and enlarged nuclei; variable mitotic activity and atypical mitoses. Dyskeratotic cells are usually present, along with parakeratosis of the horny layer. Radiological investigations are a must to evaluate the involvement of the underlying bone. Long-standing cases are associated with bony involvement in up to 60% of cases.23
Moh's micrographic surgery is the treatment of choice. Other techniques which may be used when appropriate include electrodesiccation and curettage; cryosurgery; simple excision; and radiation therapy. Bone/joint involvement requires amputation because of the risk of systemic metastases.23178

Figure 14.8: Squamous cell carcinoma of the nail unit in an 75-year-old male. The lesion had been growing rapidly over 6 months.
Keratoacanthoma (KA)
Keratoacanthoma is a rare tumor of nail unit. It usually involves thumb and index fingers in patients aged 40–60 years. The predisposing factors include previous trauma or HPV infection. Multiple and familial cases are reported. Keratoacanthomas may arise from nail bed or folds, and present with pain, swelling and erythema, mimicking paronychia and often producing onycholysis. Nail unit KAs differ from SCC as they appear at a younger age; grow rapidly and generally do not invade underlying bones.35 However, bony destruction may occur sometimes, owing to the pressure effects of the rapidly growing mass. Unlike cutaneous KAs, spontaneous regression is highly unlikely for nail unit KAs.35 Also, a clinical and histological differentiation between KA and SCC is not always possible, hence, KA is best considered as a low-grade variant of SCC.35
Complete excision is the treatment of choice. Most lesions are amenable to local excision and curettage. Moh's micrographic surgery helps reduce the risk of recurrence.15
Malignant Melanoma (MM)
Nail unit melanomas are rare but devastating in nature. These tumors may arise from nail bed or nail matrix. Thumb is affected most commonly followed by index finger.38 Patient often refers to a traumatic event prior to the development of the tumor; however, causal association with trauma is not known. The relative incidence of nail unit melanomas is higher in blacks compared to fair skinned population; with 20% of melanomas in black people arising in nail unit.39
Nail matrix melanoma usually presents as longitudinal melanonychia (being the first symptom of MM in 76% patients). Dark band with blurred margins, wider proximal portion, nail plate thinning and fissuring and presence of periungual pigmentation (Hutchinson's sign) may help in distinguishing longitudinal melanonychia of MM from benign bands commonly seen in darker races.23 However, clinical signs cannot be completely relied on and may be misleading. Presence of Hutchinson's sign warrants a nail matrix biopsy. Pseudo-Hutchinson's sign may be seen in some as very dark bands, which become visible through the cuticle. It must be 179remembered, however, that up to 20% of nail unit melanomas may be amelanotic.23 Subungual lesions present with nodules leading to onycholysis, nail bed ulceration and bleeding. Specific dermatoscopic features have been evaluated for confirming the diagnosis of melanoma, however, these are not well established and should not substitute histopathological evaluation.23
Histopathology shows presence of atypical melanocytes extending to variable depths of the dermis. There may be an inflammatory response to invasive melanoma cells consisting of lymphocytes, and melanophages may be present.23
Nail unit MM has a poor prognosis as early diagnosis is difficult in this region. In a series of 46 patients, 61% had tumors invasive to Clark's level IV or V at the time of diagnosis and one quarter already had lymph node or distant metastasis.40 Five-year survival rate is poor, ranging from 20 to 60%.35
Treatment is often unsatisfactory. Amputation is generally required. Thinner lesions may be treated with local excision.35 Moh's microsurgery has been evaluated in a small series of patients and may be a favorable option for thin lesions.41
Basal Cell Carcinoma
Despite being the most common skin cancer, nail unit BCC is very rare. Rare cases reported had a metatypical histological pattern, that is, they have a component of SCC.42 Local excision; curettage and electrodesiccation has been successful in the reported cases.
Metastatic Tumors
Nail unit metastasis are most commonly reported in patients with primary tumors of the lung (41%), genitourinary tract (17%) and breast (9%).43 The other reported sites of primaries are the head and neck region, bone (sarcoma), skin (melanoma), gastrointestinal tract and liver.43 Within the nail unit, subungual location is the most common for metastasis. Periungual lesions usually develop as a result of direct extension from subungual masses. An NUT may be the first presentation of the malignancy in about 44% of cases.43 Metastasis generally present as painful, erythematous enlargement or swelling of the distal digit or as a red to violaceous nodule that distorts the nail plate, soft tissue of the distal digit or both. These patients have a poor overall prognosis, with only a few months survival following the diagnosis. Radiological evidence of bony involvement is either already present or subsequently develops in 92% of cases.43 Histopathology is helpful in confirming the diagnosis.
References
- Domínguez-Cherit J, Chanussot-Deprez C, Maria-Sarti H, Fonte-Avalos V, Vega-Memije E, Luis-Montoya P. Nail unit tumors: a study of 234 patients in the dermatology department of the “Dr Manuel Gea González” General Hospital in Mexico City. Dermatol Surg. 2008;34:1363–71.
- Tosti A, Piraccini BM. Warts of the nail unit: surgical and nonsurgical approaches. Dermatol Surg. 2001;27:235–9.
- Finkel ML, Finkel DJ. Warts among meat handlers. Arch Dermatol. 1984;120:1314–7.
- Baran R, Richert B. Common nail tumors. Dermatol Clin. 2006;24:297–311.
- Laurent R, Kienzler JL. Epidemiology of HPV infections. Clin Dermatol. 1985;3:64–7.
- Mascarò JM, Mascarò JM Jr. Warts and condilomas. In: Katsambas AD, Lotti TM. (Eds). European handbook of dermatological treatments. Berlin: Springer-Verlag, 1999:624.
- Hirose R, Hori M, Shukuva T, et al. Topical treatment of resistant warts with glutaraldehyde. J Dermatol. 1994;21:248–53.
- Silverberg NB, Lim JK, Paller AS, Mancini AJ. Squaric acid immunotherapy for warts in children. J Am Acad Dermatol. 2000;42:803–8.
- Munn SE, Higgings E, Marshall M, et al. A new method of intralesional bleomycin therapy in the treatment of recalcitrant warts. Br J Dermatol. 1996;135:969–71.
- Dawber R, Colver G, Jackson A. Viral warts, cryosurgical technique. In: Dawber R, Colver G, Jackson A (Eds). Cutaneous cryosurgery. Principles and clinical practice, 2nd Edition. London: Martin-Dunitz, 1997:43.
- Street ML, Roenigk RK. Recalcitrant periungual verrucae: the role of carbon dioxide laser vaporization. J Am Acad Dermatol. 1990;23:115–20.
- Ross BS, Levine VS, Nehal K, Tse Y, Ashinoff R. Pulsed dye laser treatment of warts: an update. Dermatol Surg. 1999;25:377–80.
- Raison-Peyron N, Alirezai M, Meunier L, et al. Onychomatricoma: an unusual cause of nail bleeding. Clin Exp Dermatol. 1998;23:138.
- de Berker DAR, Baran R. Disorders of nails. In: Burns T, Breathnach S, Cox N, Griffiths C (Eds). Rook's textbook of Dermatology, 8th edition, UK; Blackwell Publishing Ltd; 2010;65.30-65.40.
- Tosti A, Piraccini BM. Nail Disorders. In: Bolognia JL, Jorizzo JL, Rapini RP (Eds). Dermatology. 2nd edition. Spain; Elsevier, 2008.
- Rettig AC, Strickland JW. Glomus tumor of the digits. J Hand Surg. 1977;2:261–5.
- Heys SD, Brittenden J, Atkinson P, Eremin O. Glomus tumour: An analysis of 43 patients and review of the literature. Br J Surg. 1992;79:345–7.
- Van Geertruyden J, Lorea P, Goldschmidt D, et al. Glomus tumours of the hand. A retrospective study of 51 cases. J Hand Surg. 1996;21(2):257–60.
- Vasisht B, Watson HK, Joseph E, Lionelli GT. Digital glomus tumors: a 29-year experience with a lateral subperiosteal approach. Plast Reconstr Surg. 2004;114:1486–9.
- Love JB. Glomus tumors: Diagnosis and treatment. Mayo Clin Proc. 1944;19:113.
- Daugaard S, Jensen ME, Fisher S. Glomus tumours. An immunohistochemical study. APMIS. 1990;98:983–90.
- Tosti A, Richert B, Pazzaglia M. Tumours of the nail apparatus. In: Scher RK, Daniel III CR (Eds). Nails: Diagnosis, Therapy, Surgery, 3rd edition, China, Elsevier Saunders, 2005;195–204.
- Zaballos P, Carulla M, Ozdemir F, Zalaudek I, Baáuls J, Llambrich A, Puig S, Argenziano G, Malvehy J. Dermoscopy of pyogenic granuloma: a morphological study. Br J Dermatol. 2010;163:1229–37.
- Baran R. Retinoids and the nails. J Dermatol Treat. 1990;1:151–4.
- Bouscarat F, Bouchard C, Bachour D. Paronychia and pyogenic granuloma of the great toes in patients treated with indinavir. N Engl J Med. 1998;338:1776–7.
- Higgins EM, Hughes JR, Snowdon S, Pembroke AC. Cyclosporin induced periungual granulation tissue. Br J Dermatol. 1995;132:829–30.
- Busam KJ, Capodicci P, Motzer, Kiehn T, Phelan D, Halpern AC. Cutaneous side-effects in cancer patients treated with the antiepidermal growth factor receptor antibody C225. Br J Dermatol. 2001;144:1169–76.
- Nakano J. Paronychia induced by gefetinib, an epidermal growth factor receptor tyrosine kinase inhibitor. J Dermatol. 2003;30:261–2
- Gonzales S, Vibhagool C, Falo LD Jr, Momtaz KT, Grevelink J, González E. Treatment of pyogenic granulomas with the 585 nm pulsed dye laser. J Am Acad Dermatol. 1996;35:428–31.
- Hall CR, Cole WG, Haynes R, Hecht JT. Reevaluation of a genetic model for the development of exostosis in hereditary multiple exostosis. Am J Med Genet. 2002;112:1–5.
- Sau P, McMarlin SL, Sperling LC, et al. Bowen's disease of the nail bed and periungual area. A clinicopathological analysis of seven cases. Arch Dermatol. 1994;130:204–9.
- Spencer JM. Malignant tumopurs of the nail unit. Dermatol The. 2002;15:126–30.
- Eliezri YD, Silverstein SJ, Nnuevo GL. Occurrence of human papilloma virus 16 DNA in cutaneous squamous and basal cell neoplasms. J Am Acad Dermatol. 1990;23:836–42.
- Kawashima M, Jablonska S, Favre M. Charaterization of a new type of human papilloma virus found on a lesion of Bowen's disease of the skin. J Virol. 1986;57:688–92.
- Spencer JM. Nail apparatus melanoma. Lancet. 1999;353:84–5.
- Finley RK, Driscoll DL, Blumeson L, Karakousis CP. Subungual melanoma: an eighteen year review. Surgery. 1994;116:96–100.
- Heaton KM, El Naggar A, Ensign LG, Ross MI, Balch CM. Surgical management and prognostic factors in patients with subungual melanoma. Ann Surg. 1994;219:197–204.
- Zitelli JA, Brown C, Hanusa BH. Mohs micrographic surgery for the treatment of primary cutaneous melanoma. J Am Acad Dermatol. 1997;37(2 Pt 1):236–45.
- Hoffman S. Basal cell carcinoma of the nail bed. Arch Dermatol. 1973;108:828.
- Cohen PR. Metastatic tumors to the nail unit: subungual metastases. Dermatol Surg. 2001;27:280–93.
Synonyms: Ingrowing nail; Onychocryptosis; Unguis incarnates; Ungua labial hypertrophy
Introduction
Onychocryptosis (from Greek onyx nail and kryptos hidden) is an extremely common problem causing considerable pain and discomfort. The term “ingrown nail” is controversial since the nail plate is implemented as etiology for ingrowing but others believe that lateral nail wall tissue is the cause. It is common in adolescents and young adults but can occur at any age including children and elderly.1
Etiopathogenesis
There are different types of ingrowing nails. The causes for the ingrowing nails are varied at different age group as enumerated in Table 15.1. The commonest age group is adolescent and most common form is distal-lateral ingrowing.2 183
|
There are many theories on the etiology of onychocryptosis. The widely accepted theory is that onychocryptosis occurs due to penetration of the lateral nail fold by the edge of the nail plate causing foreign body reaction. This local inflammatory process leads to formation of granulation tissue, secondary bacterial colonization, and eventually infection.3 Also, this process results in permanent hypertrophy of the nail fold which creates new pressures on the periungual tissues, fostering recurrence of the problem.4 Vandenbos and Bower postulated that pressure necrosis of the soft tissue surrounding the nail contributes to the pathogenesis of ingrown toenails.5 Indeed, increased nail-fold skin width in patients with ingrown toenails, greater weight-bearing on the soft tissue of the nail fold and repetitive rotation of the toe have all been suggested to be important contributing factors.5–7 Pearson et al reported no differences in the shape of the toenails among patients with ingrown toenails and healthy controls and substantiated the Vandenbos theory that the nail is not the real culprit.8
Predisposing Factors9
The predisposing factors implicated in the development of an ingrown toenail are as follows:
- Poorly fitting shoes: Extrinsic compression of the great toe by tight footwear and narrow shoes leading to constant pressure directly on the medial nail wall and indirectly on the lateral wall as the great toe is pushed against the second toe.
- Improperly trimmed toenails: Tapering or rounding the corners while cutting the nail. Cutting the nail too short will allow more bulging of soft tissue leading to an inflammatory reaction and pressure necrosis.6
- Excessive sweating: Excessive sweating and maceration causes the skin of the nail folds to become soft that can be easily penetrated by the nail. It also predisposes to colonization by bacteria and fungi leading to infection.
- Nail infections: In tinea unguium or onychomycotic nails, the nail plate becomes brittle resulting in easy breaking off of nail spicules, making it easier for the nail to pierce the surrounding skin.
- Nail apparatus abnormalities: Improper shape of the nail plate, thick nail folds, medial rotation of the hallux (eversion) and reduced nail thickness can play a role in the development 184of the ingrown toenail.6 A nail that is more curved from side-to-side rather than being flat is more likely to become an ingrown nail.
- Others: Diabetic patients have been found to have a higher incidence of ingrown nails compared to nondiabetic patients.10 Ingrown toenail and paronychia have been reported secondary to drugs, such as indinavir and indinavir/ritonavir combination.11,12 Excess nail fold granulation tissue and ingrown toenail have also been reported with retinoids,13 docetaxel,14 cyclosporine15 and oral antifungal treatment.16 Subungual neoplasms may cause ingrown toenails due to compression of the nail plate against the nail fold.
Clinical Features
Ingrowing nail commonly affects the great toe, occasionally it can involve the other toes. Onychocryptosis is more frequent in men (62%) than in women (38%). Although all age groups are affected, most patients are adolescents in the first and second decades of life. The fibular canal is more often affected than the tibial canal, in a proportion of 2:1.17 Initially, patient complaints of pain and redness, followed by swelling and pus formation. Granulation tissue then forms, increasing the compression, which adds to the swelling and discharge. Heifitz divided onychocryptosis into three stages.18 Recently, Mozena refined this classification and described four stages (Table 15.2, Figures 15.1A to D).19
Differential Diagnosis
Differential diagnosis includes subungual exostosis, primary osteomyelitis of the phalanx and tumors of the nail bed, including subungual melanoma, trauma, paronychia, onycholysis, and onychophosis.
|

Figures 15.1A to D: Stages of ingrown toenails: (A) Stage I; (B) Stage IIa; (C) Stage IIb; (D) Stage III(Source: Khunger N, Kandhari R. Ingrown toenails. Indian J Dermatol Venereol Leprol 2012;78:279-89)
Complications
Paronychia or secondary infection of the nail fold is common and can be caused by Staphylococcus, Pseudomonas, Candida, and superficial dermatophytes. It is important to treat any secondary infections resulting from or following ingrown toenails. Scarring of the nail fold and skin and rarely, cellulitis and osteomyelitis can occur. In diabetics, it may lead to amputations or life-threatening infections.
Management of Ingrown Nail
Ingrown nails can be managed by both—non-surgical and surgical interventions. Surgery for ingrown nail is indicated if patient has pain and functional disability; recurrent onychocryptosis, surgical relapse, or iatrogenic nail disorders; and when conservative treatments have failed.17 Surgical interventions aim at removing the ingrown part of the nail plate partially along its length and partial destruction of the matrix to the corresponding area of the nail removed. This procedure is aimed at relieving symptoms and preventing regrowth of the nail in the same direction and prevents recurrences yet maintains cosmetically and functionally acceptable nail structure. Non-surgical and conservative managements are primarily aimed at prevention and treatment at early stages while surgical management by partial nail avulsion with matricectomy is the best treatment strategy for moderate to severe stages of ingrown nails. Ingrown nails manifesting in any of the finger or toenails is a theoretical possibility; it invariably occurs in the great toe and less commonly in the second toe. However, congenital malformation leading to ingrown toenails usually manifest in all the toenails or in any one of the toes.
General Measures for the Prevention and Management of Early Stages of Ingrown Nails
Preventive Measures
- Avoid tight fitting shoes and use either sandles or shoes with a roomy front
- Avoid over jealous and deep trimming, ideal to trim the outgrown portion only, maintaining a straight line. Avoid deep cutting of the edges
- Appropriate and timely management of any underlying cause such as hyperhidrosis, onychomycosis and congenital anomalies.
Non-surgical Management Strategies9
- Insert a small ball of sterile cotton wisp underneath the ingrowing edges of the nail by gently lifting the leading distal edge by nail elevator. Maintain proper hygiene and replace the cotton wisp frequently to avoid impaction and infection.
- Insertion of dental floss (Figure 15.2) from the distal end towards the proximal part underneath the ingrown nail; try to lift the edge of the nail plate with repetitive to and fro movements keeping upward traction. Patients are advised to practice the procedure daily by taking care of the hygiene.
- Insertion of a semicircular malleable (soft) plastic tube (Figures 15.3A to D) from the distal end of the ingrown toe nail by lifting the edge of the nail plate to be inserted slowly for a length of one centimeter or more (A small piece of vertically split intravenous-drip infusion set's plastic tube is author's choice).
- One end of Band-aid/plaster tape (Figure 15.4) is placed on one side of the lateral nail fold adjacent to the ingrown toenail and the rest is twisted around the toe from the ventral side at an angle directed proximally and pasted to the dorsal aspect of the proximal portion of the toe avoiding covering of the inflamed area such that the lateral nail fold is constantly pulled away.
- Nail wiring, angle correction technique, acrylic artificial nail and nail brace are other conservative techniques that have been described in the literature but are more complex for regular practice by patient.

Figure 15.2: Treatment of ingrown toenail using dental floss. Inset: Irregularly cut nail spicule seen

Figures 15.3A to D: Gutter splint technique; (A) Stage 2 ingrown toenail; (B) Proximal digital block at the base of great toe; (C) Insertion of longitudinally cut intravenous tube; (D) Edges of the tube trimmed

Surgical Method
Many surgical procedures are described for the management of ingrown toenails but most of them have high recurrence rate. The ideal surgical procedure should result in a high level of patient satisfaction both functionally and esthetically, a rapid return to normal activities, and a low rate of recurrence.1 7 Simple nail avulsion alone, without matricectomy leads to high recurrence rates of up to 70%.20,21 Various techniques and procedures are used in the surgical management of the ingrown nail depending on the stage of the disease and expertise of the treating dermatologist or surgeon (Figure 15.5).188

Instruments Required for Nail Surgeries (Figure 15.6)

Figure 15.6: Instruments used in surgical management of ingrown toenail L-R: 88% phenol, toothpick, skin punch, Frei's speculum, nail clipper, artery forceps- straight and curved, scissors – iris and medium straight, forceps
Preoperative preparation:
- Detailed history, examination and clinical diagnosis
- Detailed history of systemic disorders like collagen vascular disorders, bleeding disorders, diabetes mellitus, etc.
- History of drug intake and discontinuation of acetylsalicylic acid, NSAID's and other blood thinners 5 to 6 days before the surgery and readjustment of anti-coagulant dosage
- Discontinuation of smoking prior to surgery
- Preoperative cleaning of the surgical sites
- Appropriate premedication and antibiotic prophylaxis if necessary
- Detailed informed consent with information on possible work disruption and time taken for regrowth of nail plate
- History of vasovagal syncope and anaphylaxis to local anesthesia.
Contraindications
There are no absolute contraindications for nail surgeries. Relative contraindications to performing surgery in the nail unit are outlined as follows
- Peripheral vascular disease
- Collagen vascular disease
- Uncontrolled diabetes mellitus
- Disorders of hemostasis
- Acute infection or inflammation of the nail unit and the surrounding paronychial tissue
- Reported allergy to anesthetic agent.
Anaesthesia
Digital block is the standard anesthetic procedure, however metatarsal block is preferred by some. Proximal digital block is commonly practiced (Figures 15.7A to D). Proper understanding of anatomy of digital innervations and blood supply are vital for achieving optimal anesthesia. Usually 2% xylocaine solution without adrenaline is the local anesthetic agent of choice.

Figures 15.7A to D: Preparation of parts: (A and B) Proximal digital block. Needle is inserted at the base of the great toe; (C) Digital exsanguinations using finger glove; (D) Same is rolled back which act as tourniquet
Excision of the Spicule and Partial Matricectomy: Suppan 1 Technique
It is advocated for individuals with Stage I ingrown toenail affecting the nail plate without hypertrophy of the nail fold. Preferably done in adults or elderly patients and in diabetics, in whom tissue-regeneration capacity is reduced and recurrence rate is more.17 The technique consists of excision of the affected portion of the nail plate followed by partial mechanical matricectomy (with curette or scalpel).
Partial Chemical Matricectomy: Phenol-Alcohol Technique
It involves excision of the portion of affected toenail and partial matricectomy by phenol (Table 15.3, Figures 15.8A to E). This technique is indicated in onychocryptosis affecting the nail plate with hypertrophy of the nail fold of less than 3 mm (stage-I and IIa).17 This procedure has success rates upto 90%. It is less painful, has a lower morbidity and higher success rate than surgical excision of the matrix. Other advantage is that phenol causes nerve damage at the site of surgery, which provides a degree of analgesia but does not result in any long-term deficit. Phenol-alcohol technique is safe in diabetic patients who have no vascular risk and have good control of their diabetes but contraindicated in diabetes with some vascular risk or poor control of diabetes. Local complications include tissue necrosis, pain and persistent exudate postoperatively. Systemic toxicity is rare due to very low quantity of phenol applied but rarely possible due to longer duration of contact, which includes abdominal pain, dizziness, cyanosis, hemoglobinuria and cardiac arrhythmias.9 However, as per the authors experience, phenolization if performed carefully with optimal quantity just to damage the matrix by avoiding damage to the surrounding structures yields good results without any complications as described above. It is also advised not to keep the phenol in a open container during the procedure to avoid complications due to its inhalation. The other agents used for chemical matricectomy are sodium hydroxide22,23 and trichloroacetic acid.24 Other options for destruction of the nail matrix, as well as for destruction of granulation tissue, include electrocautery, radiofrequency surgery and carbon dioxide laser ablation. However 88% phenol solution is the best agent for matricectomy as per the available data and author's personal experience.

Figure 15.8A to E: Treatment of ingrown toe nail with partial nail avulsion followed by phenol matricectomy; (A) Ingrowing toenail Stage II; (B) Freeing the lateral margin; (C) Lateral nail plate avulsion; (D) Lateral chemical matricectomy with 88% phenol using toothpick); (E) Immediate post-operatively
|
Wedge Resection of the Toenail and Nail Fold
This procedure can be carried out via the esthetic reconstruction technique or the Winograd technique. Both involve excision of the affected portion of the nail plate, partial matricectomy and wedge extirpation of the hypertrophic nail fold and the nail bed.
Aesthetic reconstruction technique:25 Is done in onychocryptosis with hypertrophy of the nail fold exceeding 3 mm in thickness (Stage IIb). This technique involves complete removal of the nail plate and debridement of the granulation tissue, after which wedge-shaped ellipse of skin and subcutaneous tissue lateral to the affected nail fold is removed in order to reduce the convexity of the nail fold.192
Winograd technique: This procedure is preferred in Stage III onychocryptosis. In this technique wedge excision of the lateral matrix horn with better preservation of the lateral nail fold is done.26
Total Matricectomy
Total matricectomy is indicated for Stage IV onychocryptosis (ingrown nail) in adult patients, onychogryphosis, onychodystrophy and chronic hypertrophy of the distal and lateral folds. It involves nail plate avulsion followed by total matricectomy either by surgical excision or chemical cautery using phenol.
CO2 laser, Er:YAG laser, radiofrequency ablation and electrocautery are other techniques employed for matricectomy. However, it may be difficult to completely ablate or destroy the lateral horn of the matrix in total without exposing it by reflection of the proximal nail fold by the above procedures and hence the possibility of growth of nail spicules post-surgically.27 Application of 80–88% phenol solution in an optimal quantity is always a better option for complete matricectomy.28
Other Procedures
- Decompression technique: Unilateral soft tissue resection of the nail fold combined with partial nail plate avulsion technique without permanent matricectomy.29
- Soft-tissue nail fold excision technique: Skin and soft tissue enveloping the nail is removed and allowed to heal with secondary intention.30
- Nail avulsion and silicone gel sheeting: Useful in reducing the thickness of the hypertrophic nail fold and prevent the recurrence of the condition during the regrowth of the nail plate. It involves excision of one-quarter of the lesional side of the nail plate followed by application of silicone gel sheet on the granulation tissue and the exposed nail bed.31
References
- Murray WR, Bedi, B S. British Journal of Surgery. 1975; 62:409.
- Haneke E. Controversies in the treatment of ingrown nails. Dermatology research and practice.
- DeLauro NM, DeLauro TM. Onychocryptosis. Clinics in Podiatric Medicine and Surgery 2004;21:617–30.
- Vandenbos K, Bowers W. Ingrowing toenail: a result of weight bearing on soft tissue. U S Armed Forces Med J. 1959;10:1168–73.
- Langford DT, Burke C, Robertson K. Risk factors in onychocryptosis. Br J Surg. 1989;76:45.
- Antrum RM. Radical excision of the nailfold for ingrowing toenail. J Bone Joint Surg Br. 1984;66:63.
- Pearson HJ, Bury RN, Wapples J, et al. Ingrowing toenails: Is there a nail abnormality? A prospective study. J Bone Joint Surg Br. 1987;69:840.
- Khunger N, Kandhari R. Ingrown toenails. Indian J Dermatol Venereol Leprol. 2012;78:279–89.
- Riviera A. Risk factors for amputation in diabetic patients: A case controlled study. Arch Med Res. 1998;29:179–84.
- James CW, McNelis KC, Cohen DM, Szabo S, Bincsik AK. Recurrent ingrown toenails secondary to indinavir/ritonavir combination therapy. Ann Pharmacother. 2001;35:881–4.
- Bourezane Y, Thalamy B, Viel JF, Bardonnet K, Drobacheff C, Gil H, et al. Ingrown toenail and indinavir: A case control study demonstrates strong relationship. AIDS 1999;22:2181–2.
- Baran R. Retinoids and the nails. J Dermatol Treat. 1990;1:151–4.
- Nicolopoulos J, Howard A. Docetaxel- induced nail dystrophy. Australas J Dermatol. 2002;43:293–6.
- Higgins EM, Hughes JR, Snowden S, Pembroke AC. Cyclosporin-induced periungual granulation tissue. Br J Dermatol. 1995;132:829–30.
- Weaver T, Jespersen D. Multiple onychocryptosis following treatment of onychomycosis with oral terbinefine. Cutis 2000;66:211–2.
- Martínez-Nova A, Sánchez-Rodríguez R, Alonso-Peáa D. A new onychocryptosis classification and treatment plan. J Am Podiatr Med Assoc. 2007;97:389–93.
- Heifitz CJ. Ingrown toenail: a clinical study. Am J Surg. 1937; 38: 298–315.
- Mozena JD. The Mozena classification system and treatment algorithm for ingrown hallux nails. J Am Podiatr Med Assoc. 2002;92:131–5.
- Gupta S, Sahoo B, Kumar B. Treating ingrown toenails by nailsplinting with a flexible tube: An Indian experience. J Dermatol. 2001;28:485–9.
- Moriue T, Yoneda K, Moriue J, Matsuoka Y, Nakai K, Yokoi I, et al. A simple therapeutic strategy with super elastic wire for ingrown toenails. Dermatol Surg. 2008;34:1729–32.
- Ozdemir E, Bostanci S, Ekmekci P, Gurgey E. Chemical matricectomy with 10% sodium hydroxide for the treatment of ingrowing toenails. Dermatol Surg. 2004;30:26–31.
- Tatlican S, Eren C, Yamangokturk B, Eskioglu F, Bostanci S. Chemical matricectomy with 10% sodium hydroxide for the treatment of ingrown toenails in people with diabetes. Dermatol Surg 2010;36:219–22.
- Kim SH, Ko HC, Oh CK, Kwon KS, Kim MB. Trichloroacetic acid matricectomy in the treatment of ingrowing toenails. Dermatol Surg. 2009;35:973–9.
- Persichetti P, Simone P, Livecchi G, Di Lella F, Cagli B, Marangi GF. Wedge excision of the nail fold in the treatment of ingrown toenail. Ann Plast Surg. 2004;52:617–20.
- Winograd AM. Modification in the technique of operation for ingrown toe-nail.1929. J Am Podiatric Med Assoc. 2007;97:274–7.
- Vanhooteghem O, Henrijean A, André J, Richert B, De La Brassinne M, Ingrown nails: a complication of surgery for an in-growing toe-nail using the Zadik procedure. Ann Dermatol Venereol 2006;133:1009–10.
- Baran R, Haneke E. Matricectomy and nail ablation. Hand Clin. 2002;18:693–6.
- Aksakal AB, Oztas P, Atahan C, Gurer MA. Decompression for the management of onychocryptosis. J Dermatolog Treat. 2004;15:108–11.
- Chapeskie H, Kovac JR. Soft-tissue nail-fold excision: A definitive treatment for ingrown toenails. Can J Surg. 2010;53:28–6.
- Aksakal AB, O'zsoy E, Gurer MA. Silicone gel sheeting for the management and prevention of onychocryptosis. Dermatol Surg. 2003;29:261–4.
Nail discoloration, often has been an interesting entity to all dermatologists. Fascinating colors are often encountered, and become an element of curiosity to a clinician.
Intentional, artefactual discoloration tends to be a nail adornment in women and also in men. Henna dyes and nail polish can create a myriad of colored nails on a temporary basis, adding more to the clinical confusion. Clinical history hence is important in all cases of colored nails.
Spontaneous pigmentation of nail, either abrupt or insidious calls for comprehensive evaluation, as this may indicate a disease of the nail apparatus or may be a marker of an internal disease. Brown-to-black pigmentation of nails is called as ‘Melanonychia’.1
Etiologically the causes may be studied based on the level of involvement:
- Affect on the dorsal nail surface.
- Substance of the nail plate.
- Undersurface of the nail or the nail bed.
Exogenous or Nail Surface Changes
Exogenous pigment is easily demonstrated by scraping and easy removal. There always is a proximal arc to the pigment matching the shape of the proximal nail fold, and the gap between 195the pigment and fold widens with progress of time (Figure 16.1). Examples are ‘Quitters nails’ of smokers, election indelible marker ink stain (black) (Figure 16.2) and henna stain (yellow brown) (Figure 16.3) are often seen in India.
Exogenous pigment on undersurface of nail plate is difficult to demonstrate, and may need avulsion of the nail plate to be differentiated from nail bed pigmentation. The green pigment of Pseudomonas infection is an example (Figure 16.4).
Exogenous causes often include tobacco, dirt, tar, iodine, potassium permanganate and silver nitrate, and these may cause a brown-to-black pigmentation. This non-melanotic pigmentation is called as chromonychia. Most exogenous pigmentation can be scratched off easily.2




Nail Plate Pigmentation
Loss of normal lucency is often the clue, and this may happen from addition of pigment, or alteration of normal cellular and intercellular organisation of nail plate structure.
Pigment often in the form of melanin produced by matrix melanocytes may get added and is often seen as a brown longitudinal streak along the length of the nail called ‘Melanonychia striata’ (Figure 16.5). It results from a physiologic activation of melanocytes in the nail matrix. It is also known as ‘Racial longitudinal melanonychia’ and is common in Asians, and often abnormal in Whites necessitating a evaluation to rule out occult melanoma of the proximal nail apparatus.3
Nail biting, friction, inflammatory diseases like psoriasis and systemic lupus erythematosus (SLE), hydroxyurea treatment, PUVA therapy and pregnancy may result in melanotic nail pigmentation from stimulation of melanocytes.
Heavy metals and some drugs may get incorporated through the nail matrix and cause discoloration as is the gray color seen with silver.
Disruption of nail plate formation may occur in trauma, chemotherapy, disease and poisoning. This results in waves of parakeratotic cells or small splits between cell columns. The obvious result would be reduced lucency of the nail plate, and white marks called as leukonychia.


This discoloration resulting from collagen disorganization may arise from the matrix or other parts of the nail as in fungal infections where it may be seen distally or laterally, based on the fungal species. (Figure 16.6).
Nail Bed Changes
Vascular changes in the nail bed either localized or generalised may also result in color changes.
Differential blood supply to the tumor and vicinity is always helpful in diagnosing a Glomus cell tumor.
Hematoma often is diagnosed from the initial pain, and red discoloration (Figure 16.7). With progress of time the hematoma becomes organised and, may result in local onycholysis, displaying color change following hemoglobin deposition and gets pushed distally alongwith the growing nail plate. Chronic minor trauma as in an ill-fitting shoe can result in a longitudinal dark band.
Splinter hemorrhages often appear in the fine serrated topography between the nail plate and bed, and appear as miniature linear red streaks in the distal part of the nail plate (Figure 16.8). Color changes and gradual drift are akin to that in a hematoma.


Trauma apart, psoriasis, dermatitis and dermatophytosis may be other causes. Large number of proximal hemorrhage in the absence of trauma indicates a systemic cause like bacterial endocarditis or antiphospholipid syndrome. Unilateral splinters may appear after arterial catheterization.
Subungual hyperkeratosis, and drug deposits like with antimalarials and phenothiazines also cause a change of color.4
Some Interesting Entities
True Leukonychia
White nails indicate a matrix dysfunction. Total leukonychia is a rare inherited form characterized by porcelain, milky white nails. Subtotal leukonychia shows white color in proximal two thirds and a distal pink discoloration. Tranverse leukonychia (Mee's lines) reflects a systemic cause, either poisoning or chemotherapy affecting the matrix. The 1-2 mm arcuate band is alike the lunula, and is analogous to the Beau's lines.5 Punctate leukonychia, shows 1-3 mm white spots and can be caused by trauma as in manicure or may also be seen in alopecia areata. The pattern and number of puncta may be variable during nail growth. In Longitudinal leukonychia a parakeratotic focus is the cause, and the same is seen in Darier's disease or growth of a small tumor.
Apparent Leukonychia
Changes in nail bed are the reason here, and the same may be caused by anemia, edema or vascular impairment. A normal nail plate perched on a pale nail-bed is seen.
Terry's Nail
Mildly increased vascularity results in proximal white and a distal normal color and is attributed to cirrhosis, congestive cardiac failure and adult-onset diabetes mellitus. This is differentiated from Half-and-half nail where there is a proximal white zone and a distal brownish sharp discoloration, which is seen in 9-50% of chronic renal failure patients and after chemotherapy. Neapolitan nails may be a mix of the above nails and may be a feature of old age. Bands of white, brown and red are seen here.
Muehrcke's Nail
Two white lines with a band of pink parallel to the lunula is seen in hypoalbuminemia, and a correction of the same makes the entity a reversible one.
Drug-induced Discoloration
Tetracyclines result in yellowish discoloration and distal photo-onycholysis, and the same is reversible on drug discontinuation. Mepacrine causes bluish color which flourescences as white or yellow-green under the Wood's lamp.
Chloroquine causes blue-black color of the nail bed, while other antimalarials produce longitudinal bands of pigmentation in the nail bed or in the nail.199
Fixed drug eruption of the nail may cause a dark blue color. Argyria causes a slate blue color, while inorganic arsenic causes longitudinal pigment bands or transverse white stripes (Mees stripes) across the nail.
Melanin related hyperpigmentation of nail and nail bed may occur in children after doxorubicin therapy. In HIV patients, zidovudine and ART-naive patients too can show a longitudinal melanonychia. (Figure 16.9).6
In drug related melanonychia the pigmentation usually fades over months to years after withdrawal of the offending drug.
Yellow Nail Syndrome
The color is secondary to thickening, and a tinge of green may also occur in the presence of infection. Loss of cuticle, obscuring of lunula and increased curvature both longitudinally and horizontally are seen. The condition often seen in adults, is accompanied with acquired lymphedema and a nasal sinus or respiratory disease. All nails get affected and obvious is the slow nail growth. Evaluation for occult malignancies, hypothyroidism and AIDS needs to be done. Nail changes are often permanent.7
Red Lunulae
Erythema of all or part of the lunula may be seen. The change may be transient. Dotted red lunulae are reported in alopecia areata and psoriasis.
Fungal Melanonychia
Though termed a rare entity, this is often seen in our setup. The number of cases seems to be on the rise, so also are the varieties of causative fungi. The current list includes 21 dematiaceous, and 8 species of non-dematiaceous fungi. Superficial phaeohyphomycosis is the general term used to describe these ungual dematiaceous species, which always pose a therapeutic challenge. Shades of brown to black used by melanin deposits pose a diagnostic challenge as they may mimic a subungual melanoma (Figure 16.10).


The fungi are often found in soil, wood, polluted water and decomposing plants, and are endemic to tropical and subtropical regions. This infection is often encountered as an occupational disease.
Alternaria alternata is the frequently encountered fungus. Scytalidium infections are often encountered in Europe, while Exophiala species are relatively new entities. Among the causative non-dematiceous fungi are Trichophyton rubrum and Candida species. It may be noted that the fungal melanin is produced by the Pentaketide pathway1, than the classical tyrosine pathway. The melanin incorporated in the mycelial wall protects them from temperature variations, various rays and enzymatic hydrolysis. Their role in virulence is unclear, but resistance to drugs is known.
The discolored nail often is dystrophic, and raised. Periungual inflammation is common. Clinical pattern often is a clue to the origin of infection. Longitudinal melanonychia with a distal broadening is seen in T. rubrum, while Scytalidium dimidiatum, Aspergillus niger, and Alternaria alternata cause a diffuse brown pigmentation. Paronychia is often seen in Candidiasis, while it is infrequent in dermatophytosis. The paronychial inflammation often activates the host melanocytes resulting in nail pigmentation of candidiasis.3
While proximal onychomycosis is common with dermatophytes, distal and lateral infection often is a result of Alternaria alternata and Scytalidium species. Infection beginning at the distal corner and progressing proximally in the undersurface often on the great toe is common with the latter species. Painful paronychia is often the presenting symptom. Simultaneous harboring of toe webs and soles is also frequent.
Superficial black/white onychomycosis is caused by non-dematiceous molds like Aspergillus niger. Periungual inflammation and black pigmentation of proximal nailfold are frequent. The pigmented areas are soft, and can be gently scraped. Any of the above clinical patterns can lead to complete destruction of nail plate known as ‘Total nail dystrophy’.8
Melanocyte Hyperplasia
This refers to an increased number of nail matrix melanocytes, and includes lentigo, nevus and subungual melanoma. Lentigo is observed in 9% of longitudinal melanonychia. Nail matrix nevi are a common cause in children with longitudinal melanonychia. Nevi comprise 12% of longitudinal melanonychia in adults.
Melanoma
Pigmentation of nail should always raise a suspicion of melanoma, and is always best ruled out. 66% of ungual melanomas present with nail pigmentation, and a high mortality always makes it imperative to exclude this diagnosis. 15–20% of melanomas in African Americans happen in the nail apparatus. Hutchinson sign or periungual spread of pigmentation to the proximal or lateral nail folds is an important sign of subungual melanoma. The same should be differentiated from Pseudo-Hutchinson sign, where a benign pigmented streak is visible through a thin proximal nail fold.
Sudden onset of nail pigmentation, sudden darkening or broadening of an existing pigment band, nail dystrophy, history of melanoma or a Hutchinson sign should all prompt a workup to rule out melanoma of the nail apparatus. Suspicion or diagnostic uncertainty should necessitate a nail biopsy.1201
References
- Finch J, Arenas R, Baran R. Fungal melanonychia. J Amer Acad Dermatol. 2012; 66,5:830-41.
- Haneke E, Baran R. Longitudinal melanonychia. Dermatol Surg. 2001;27:580–4.
- Lateur N, Andre J. Melanonychia : diagnosis and treatment. Dermatol Ther. 2002;15:131–41.
- Daniel CR. Nail pigmentation abnormalities. Dermato Clin. 1985;3:431–43.
- Marino MT. Mees’ lines. Arch Dermatol. 1990;126:827–8.
- Panwalker A. Nail pigmentation in AIDS. Ann Intern Med. 1987;107:943–4.
- Samman PD, White WF. The ‘Yellow nail’ syndrome. Br J Dermatol. 1964;76:153–7.
- Romano C, Paccagnini E, Difonzo EM. Onychomycosis caused by Alternaria sps in Tuscany, Italy from 1985-1999. Mycoses. 2001;44:73–6.
Introduction
Psychodermatology or psychocutaneous medicine focuses on the boundary between psychiatry and dermatology. Correlation between psychiatric and dermatologic disorders exist due to more than a fact, that the brain which is the center of psychological functions, and the skin has the same ectodermal origin.1 The incidence of psychiatric disorders among dermatological patients is estimated to be about 30–60%.
Psychiatry is more focussed on the internal nonvisible diseases and dermatology is focussed on the external visible diseases. Connecting disciplines is a complex interplay between neuroendocrine and immune system that has been described as the NICS or neuro immune cutaneous system. Patient with psychocutaneous disorders frequently resist psychiatric reference, and the liaison among the primary care physician, psychiatrist and dermatologist can prove very useful in the management of these diseases. Hence liaison therapy enables multidisciplinary approach with the co-operation of psychiatric and dermatologic teams and simultaneous diagnostic procedures and treatment of patients with psychodermatologic disorders.2
Psychodermatology is divided into three categories according to the relation between skin disorders and mental disorders:
- Psychosomatic (psychophysiologic disorders)
- Primary psychiatric disorders
- Secondary psychiatric disorders
Psychosomatic Disorders
The word psychosomatic refers to skin disorders that are not directly caused by psychological factors, but they can be exacerbated or worsened by emotional stress, e.g. eczema203
Primary Psychiatric Disorders
These are psychiatric conditions which induce development of various skin changes, e.g. neurotic excoriation, trichotillomania.
Secondary Psychiatric Disorders
These disorders appear as the result of:
- Certain disfiguring skin disease which induces psychologic suffering such as loss of self-confidence, anxiety and social phobia (Koo, 1995).
Nail Changes in Psychiatric Illness
Oncychophagia and Onychotillomania
- Chronic biting of the nails is known as onychophagia whereas chronic picking and manicuring of nails is known as onychotillomania.
- Onychophagia is a reflexive behavior to emotional imbalance, normally occurring in children between the ages of 4 and 18 (Figure 17.1).
- Onychophagia is transference of thumb-sucking habit, typically abandoned during third year of life when onychophagia starts. After adolescence onychophagia is replaced by the habit of lip “pinching’, chewing of pencils and other objects, nose scratching, hair twirling. It is estimated that 28–33% of children aged 7–10 years and 45% of teenagers are nail biters. The prevalence of nail biting among the people in the age range of 60–69 years is believed to be 4.5% and 10.5%.
- Nail biting is related to high anxiety and low esteem. It may be caused by overstimulation (due to stress and excitement) or under stimulation (due to boredom or inactivity).
Clinical Features
Nails look wrinkled and cracked. There is severe nail dystrophy, damaged cuticle, distal onycholysis, short irregular nail plate, increased nail growth, paronychia, spread of periungual wart, melanonychia, self-inflicted gingival injuries and dental problems. Osteomyelitis and temporomandibular dysfunction (mal-occlusion of the anterior teeth and apical root resorption of the teeth) are rare complications.
Prognosis
- Onychophagia typically follows a chronic and remittent course
- Onychotillomania results in onychoatrophy, anonychia, nail plate pigmentation, self-induced transverse groove, ingrown toe nail.
Management
- Treatment should be individualized
- To be able to quit the habit, the patient must be motivated, he/she must be aware of the need to abandon the habit. As a rule no treatment is needed for mild cases.
- For more serious situations treatment should involve removal of emotional factors inducing the habit, stimulation of good habits, and developing a conscious awareness
- The patient can be asked to paint his/her nail with lacquer for cosmetic purpose.
- Children can wear footed pyjamas as a remainder not to bite the nails
- Patients with a severe form of nail biting may benefit from psychiatric referral and intervention
- It has been suggested that pharmacotherapy is effective in approximately 60-70% of patients of onychophagia
- SSRI (selective serotonin reuptake inhibitor) are effective treatment if there is an underlying obsessive compulsive disorder
- Clomipramine also appears to be an effective, safe and well tolerated agent for the treatment of onychophagia.


Onychotemnomania
- Cutting nails too short leads to traumatization of nail body and nail fold
- It can be associated with body dysmorphic disorder, hypochondriasis, delusional disorder or depression. It may be one form of self-mutilating behavior seen in genetic disorders like Lesch-Nyhan syndrome and Smith-Magenis syndrome.
- Patients suffering from this disorder end up hurting themselves by chewing their fingers, lips or banging their heads.
Brittle Nail
Fifty percent behavioral syndromes such as anorexia nervosa and bulimia nervosa are associated with nail changes like brittle nail and hair.
Worn Down Nail Syndrome
- The surface of the nail plate becomes glossy and shiny and the edge of the nail is worn away due to chronic scratching or rubbing
- A French variant of worn down nail is the bidet nail reported by Baron and Moulin.
Bidet Nails
- These types of nail changes are commonly seen in females, who have an obsession for genital hygiene, and the nail changes are the result of excessive rubbing of nail against the porcelain of bidet while cleaning the genital area
- This is also seen in children with habit of scratching the school desk with nails and finger tips
- The resultant nail changes are triangular thinning and erythema of distal nail plate. Dilated capillaries and pinpoint hemorrhages can be seen on dermoscopy.
White Banding of Nail
White banding of nail plate is commonly seen in psychosis. The exact cause for white band is not known.
Habit-tic Deformity
Habit-tic deformity is a common condition caused by conscious or unconscious rubbing or picking of the proximal nail fold. Horizontal grooves are formed proximally due to nail matrix damage and subsequently move distally with finger nail growth. The dominant thumb nail is most affected by frequent rubbing with the ipsilateral index finger nail, although all nails can be involved.
This deformity is more common during periods of stress and is believed to result from a compulsive or impulsive control disorder. These nails demonstrate an apparent lack of cuticle and slight widening of cuticular sulcus on the thumb nail. Habit-tic deformity is often called as onychotimnomania.206
Median Nail Dystrophy of Heller
Synonyms: Dystophia unguius mediana canaliformis, onychodystrophia mediana canaliformis.
It manifests as a longitudinal plate or canal with a characteristic fir tree pattern of the transverse ridges. Some authors consider this as a subset of habit-tic deformity3 (Figure 17.2).

Figure 17.2: Habit-tic deformity (Courtesy: Dr Umashankar N, Department of Dermatology, Rajarajeshwari Medical College, Bengaluru)
Hemionychophagi
This is also called as forgotten nails. This type of nail disorder is commonly seen in patients who are hemiplegic. On the unaffected side, nails are bitten but the effected side is not bitten. Hence the name forgotten nails.
Nail Fold Vascular Plexus
Visibility of the nail fold vascular plexus appears to be a genetically transmitted marker for susceptibility to schizophrenia. Plexus visualization scores are significantly correlated with negative behavior, cognitive and motivational deficit family history, duration and severity.
Conclusion
The diagnosis and treatment of psychodermatologic disorders which involves nails should be carried out through the liaison which enables multidisciplinary approach including family physician, dermatologist, a psychiatrist, and a psychologist.
Majority of these diseases can be treated with cognitive—behavioral psychotherapy, psycho-therapeutics, stress and anxiety management techniques and psychotrophic drugs.
References
- Psychiatric danubiana; 2005;17(1-2):76–83.
- KH Basavaraj, Navya MA, Rashmi R. Relevance of psychiatry in dermatology: Present concepts. 2010,52(3):270-5.
Nail unit is composed of nail plate, nail bed, matrix, hyponychium, proximal and lateral nail folds. Nails and scalp are biological matrices where drugs and toxins tend to accumulate. Although many nail disorders have been associated with drug intake, most reports are anecdotal. Nail changes may manifest anywhere between 2 weeks to 18 months after commencement of drug therapy. Their occurrence is usually unpredictable. Usually, the changes are transient and disappear once drugs are discontinued. Rechallenge may or may not be positive.
Several factors may complicate the diagnosis of drug induced nail changes.1 They are:
- Because of the kinetics of nail formation and slow growth rate, the nail changes may appear several weeks after drug intake. This may make it difficult to correlate the abnormalities with the drug.
- Nail symptoms often improve or resolve without drug withdrawal.
- Rechallenge is often negative.
- The abnormalities do not necessarily involve all nails.
- Often, the pathogenesis of nail damage is not completely understood.
A drug should always be suspected when the signs affect all nails at the same distance from the proximal nail fold. A drug intake of 2 to 3 weeks before the appearance of the nail symptom should be considered, as a fingernail takes about 40 days to emerge from the proximal nail fold. A toenail takes about 80 days to emerge from the proximal nail fold.208
Drug induced nail changes can be simplified as follows:
- Nail matrix damage
- Beau's lines and onychomadesis
- Nail fragility
- Nail growth rate alteration
- True transverse leukonychia
- Nail bed damage
- Onycholysis and photo onycholysis
- Apparent leukonychia
- Proximal nail fold damage
- Acute paronychia
- Pyogenic granulomas
- Nail blood flow alterations
- Ischemic changes
- Subungual hemorrhages
- Splinter hemorrhages
- Nail atrophy
- Nail pigmentation
- Melanonychia
- Nonmelanin pigmentation
Nail Matrix Damage
Beau's lines and onychomadesis: Toxicity to the nail matrix keratinization results in transient or complete arrest of nail plate formation leading to Beau's lines and onychomadesis. Both are changes of the same spectrum where Beau's lines are transverse depressions and onychomadesis is whole thickness sulcus splitting the nails into two halves.
Drug induced Beau's lines and onychomadesis are usually dose related and reproducible with repetitive cycles of drug intake. There is no preventive measure and they require no treatment because they migrate distally as the nail grows.
Drugs: Cancer chemotherapeutic agents, taxanes, retinoids, carbamazepine (Figure 18.1), cefaloridine and cloxacillin,2 dapsone, fluorine, itraconazole,3 lithium, metoprolol, phenolphthalein, psoralens, sulfonamides, and tetracyclines.
Nail fragility: Mild damage to the nail matrix causes nail fragility. Two types of nail fragility are seen.
- Lamellar onychoschizia where the superficial layers of the nail plate shows lamellar exfoliation.
- Onychorrhexis where there is isolated split at the free edge which may extend proximally.
Drugs: Cancer chemotherapeutic agents, retinoids, antiretroviral agents.
Nail growth rate alteration: Drugs can increase or decrease the rate of nail growth. Decreased rate is because of decreased mitotic activity caused by the drug. The mechanism of increased growth rate is not known.
Drugs which increase nail growth rate: Fluconazole, itraconazole,4 levodopa,5 and oral contraceptives.209

Drugs which decrease nail growth rate: Cyclosporin A, heparin, lithium, methotrexate, and zidovudine.
True transverse leukonychia: Retention of nuclei occurs in the keratinocytes because of transient impairment of distal nail matrix keratinization. One or several parallel white bands of 1 to 2 mm width are seen affecting all nails at the same level and moving distally with the nail growth. Mees's lines are also an example of true transverse leukonychia.
Drugs: Chemotherapeutic agents,6, 7 especially doxorubicin, cyclophosphamide, and vincristine; are cyclosporin, fluorine, penicillamine, pilocarpine, retinoids, corticosteroids, and sulfonamides. Typically, Mee's lines occur after acute arsenic and thallium poisoning.
Nail Bed Damage
Onycholysis and photo onycholysis: Toxicity to the nail bed epithelium leads to loss of adhesion between nail plate and nail bed. The nail plate appears white. In photo onycholysis detachment occurs because of photo mediated toxic or allergic effect of the drug. Thumb nails are typically spared.
Drug induced photosensitivity is a complication usually seen with tetracycline derivatives, psoralens and flouroquinolones. Photo onycholysis is a sequelae to such photosensitive reaction. It is a part of Segal's triad of photosensitivity followed by discoloration of nails and onycholysis. Patients taking tetracyclines usually have severe onychodynia which precedes onycholysis by 1 to 3 weeks. Terminal vessels, capillaries and glomus bodies may play an important role in causation of pain.
Four different types of onycholysis have been described. They are:
- Type 1: Several fingers are involved. The separating part of the nail plate is half moon-shaped and concave distally with pigmentation of variable intensity and well demarcated proximal border.
- Type 3: Central part of the nail bed on several fingers are affected. Usually a yellowish stain which turns reddish after 5 to 10 days.
- Type 4: Bullae under the nails. Seen in photo onycholysis due to tetracyclines.
Onycholysis and photo onycholysis often regress spontaneously, even without interrupting drug intake. In some cases they may persist after the drug withdrawal. Rechallenge is usually negative.
Apparent leukonychia: Nail bed damage appears as white pigmentation of the nail plate. It fades with digital pressure. They appear as transverse parallel white bands that do not move as the nail grows. They are asymptomatic and resolve after drug withdrawal. Muehrcke's lines is an example of apparent leukonychia.
Drugs: Cancer chemotherapeutic drugs.
Proximal Nail Fold Damage
Acute paronychia: It is erythema, inflammation and pain occurring in proximal nail folds of several nails immediately after intake of the offending drug. This is because of the toxic effect of the drug on nail epithelia sometimes resulting in nail loss. Paronychia resolves with stopping of drug and is frequently followed by onychomadesis. Rechallenge is often positive.
Pyogenic granulomas: Granulation tissue with formation of painful bleeding nodules may arise from the proximal and lateral nail folds of several nails due to activation of angiogenic factors by the offending drugs. The occurrence of the same side effects with different drugs (e.g. retinoids10 and indinavir) is probably due to the fact that the HIV-1 protease catalytic site and cellular retinoic acid-binding proteins have structural analogues.
Nail Blood Flow Alterations
Ischemic changes: Certain drugs like bleomycin and β-blockers cause Raynaud's phenomenon where the distal digital perfusion is impaired leading to ischemic changes and necrosis of the nail unit. Drug withdrawal is not associated with regression of symptoms.
Subungual hemorrhages: Drug induced damage to the nail bed blood vessels can lead to splinter hemorrhages or subungual hematoma. Splinter hemorrhages occur as multiple tiny longitudinal brown streaks involving the distal nail bed. It usually involves the finger nails. Subungual hematoma appears as red to black discoloration at the juncture of nail plate and nail bed due to trapping of blood. Over time it moves distally and disappears as the nail grows.
Drugs: Antithrombotics and anticoagulants, including aspirin and warfarin,11 cancer chemotherapeutic agents,12 especially the taxanes; tetracyclines, nucleotide analogue ganciclovir.
Nail Pigmentation
Melanonychia: Nail matrix melanocytes are activated by several drugs to produce melanin leading to longitudinal or transverse bands of melanonychia varying from brown to black color pigmentation. When the band is isolated, it is important to distinguish a band of longitudinal 211melanonychia due to drugs from a band of longitudinal melanonychia due to a nail matrix melanocytic neoplasm. In doubtful cases, a nail matrix biopsy is mandatory.
Drug-induced melanonychia most commonly appears 3 to 8 weeks after drug intake. Pigmentation is usually reversible within 6 to 8 weeks, but may persist for months after drug interruption. Rechallenge is usually negative. The pathogenesis of nail melanocyte activation is unclear and is independent of melanocyte-stimulating hormone, corticotropin activity and ultraviolet light.
Drugs: Zidovudine (Figure 18.2), cancer chemotherapeutic agents (Figure 18.3),13 hydroxyurea and psoralens.14 Radiation therapy for malignant disease far from the digit can also cause longitudinal melanonychia (Figure 18.4).
Nonmelanin pigmentation: Certain systemic drugs which are excreted via the nail route are seen deposited within the nail plate giving rise to characteristic nail discoloration. There can also be dermal or periungual deposition. The pigmentation does not move as the nail grows and does not disappear completely on stopping the offending drug.
Drugs: Tetracyclines,15 gold salts often produce a yellow discoloration of the nail plate. Clofazimine (Figure 18.5) produces a dark-brown pigmentation.16




Several topical drugs, such as tar and anthralin, may deposit within the superficial layers of the nail plate, producing an exogenous brown-black pigmentation. Exogenous pigmentation migrates distally with nail growth and has a proximal border parallel to the cuticle.
Nail changes due to teratogens (Table 18.1): Nail hypoplasia or complete absence of nails which may be associated with distal digit malformation is seen.
Nail changes caused by drugs acting on CNS: See Table 18.2.
Nail changes induced by retinoids (Table 18.3): Pyogenic granuloma like lesions is reported following etretinate therapy17. Increased skin fragility with nail plate brittleness, results in fine spicules that break through the lateral nail grooves and result in the formation of pyogenic granulomas.
Drugs causing photo onycholysis (Table 18.4): Demethylchlortetracycline is the most common cause of photo onycholysis followed by doxycycline. Yellow discoloration of nails and 213photo onycholysis has been described in all the finger and toe nails in a patient treated with oxytetracycline for rosacea.18
|
| |||||||||||||||||||||||||||||||||||
Minocycline can also cause slate gray to deep blue pigmentation of the proximal nail bed or diffuse hyperpigmentation of the nail. Elemental analysis of nail clippings have shown the presence of iron chelate of minocycline in pigmented areas of the nail.
Nail changes due to antibiotics (Table 18.5): Clofazimine crystals are sometimes formed in the nail plate and nail bed in patients taking long-term therapy for leprosy.214
|
|
Nail changes due to antiretroviral drugs (Table 18.6): Pigmentation following zidovudine usually occurs 8 weeks to 1 year after starting the therapy. It is reversible once the drug is discontinued or dosage is reduced. Histological studies have shown that zidovudine induced nail pigmentation is due to melanin deposition.
Nail changes due to cardiovascular drugs: See (Table 18.7).
Nail changes due to intoxicants (Table 18.8): More than 3 μg/g of arsenic in nail samples is suggestive of arsenic intoxication. Transverse white bands called Mees’ lines, which move distally along with nail growth, suggestive of true leukonychia are seen. They may be single or multiple parallel lines. These lines appear 4–6 weeks after acute arsenic poisoning. Multiple lines are due to band-like precipitation of arsenic in nail matrices called as Liesegang phenomenon.
Nail changes caused by anticoagulants (Table 18.9): Warfarin causes purplish discoloration of the distal toes including the toe nails 3 to 8 weeks after starting warfarin therapy.215
| |||||||||||||||||||||||||||||||||||||||||
They usually fade on pressure and leg elevation.19 Purple toes occur as a result of cholesterol microembolization because of interruption of healing of atherosclerotic plaques by oral anticoagulants.
Nail changes caused by antimalarials (Table 18.10): A complex formed by antimalarial drug with melanin and hemosiderin is the cause of pigmentation. Nail pigmentation is irreversible even after stopping of the antimalarial drugs. 216
| |||||||||||||||
| |||||||||||||||||||||||||||
| |||||||||||||||||||||||||||
|
|
|
Nail changes due to hormones: See (Table 18.11).
Nail changes induced by antineoplastic agents (Table 18.12): Chemotherapeutic agents are the most important cause of drug induced nail changes. The continuously dividing nail matrix cells are easily disturbed by the antimitotic activity of the antineoplastic agents. It is very difficult to attribute the nail changes to a single drug because the drugs are used in combination in most anticancer protocols.
Management of Drug Induced Nail Changes
The Multinational Association of Supportive Care in Cancer (MASCC) has proposed a scale where nail abnormalities are divided into those of nail plate, nail folds and digit tips (Table 18.13).
- Patients with nail fragility should wear cotton gloves underneath plastic gloves while doing work.
- Patients taking phototoxic drugs can apply dark nail varnish to their nails.
- Use of frozen gloves by patients on Docetaxel chemotherapy has proved to be protective.
- In case of onycholysis, trimming or debridement of nail plate followed by gentle cleaning with 3% benzoyl peroxide.
-
Table 18.12 Nail changes induced by antineoplastic agents General nail toxicityCyclophosphamideDoxorubicinDaunorubicinVincristine5-fluorouracilTaxanesMee's linesDoxorubicinCyclophosphamideVincristineLeukonychiaCyclosporine5-fluorouracilLevamisoleMethotrexateMelanonychia (longitudinal, transverse or diffuse)VincristineAdriamycinHydroxyureaBleomycinBusulfanCyclophosphamideMethotrexateElectron beam therapyHemorrhagic onycholysisTaxanesIxabepiloneParonychiaPyogenic granulomasEpidermal growth factor inhibitorsMitozantroneTaxanesMethotrexateNail dystrophyBleomycinHydroxyurea
220Table 18.13 Multinational Association of Supportive Care in Cancer (MASCC) proposed grading of nail abnormalities Adverse eventGrade 1Grade 2Grade 3Nail plateOnycholysis or ridging without painOnycholysis with mild/moderate pain, any nail plate lesion interfering with instrumental ADL*Nail plate changes interfering with self-care ADL*Nail foldDisruption or absence of cuticle or erythemaErythematous/ tender/painful, or pyogenic granuloma or crusted lesions or any fold lesions interfering with instrumental ADL*Periungual abscess or fold lesions interfering with self-care ADL*Digit tipXerosis/erythema without painXerosis/erythema with mild/moderate pain or any digit tip lesion interfering with instrumental ADL*Digit tip changes interfering with self-care ADL**Instrumental ADL (activities of daily living) refers to preparing meals, shopping for groceries or clothes, using telephone, managing money, etc. Self-care ADL refers to personal care such as dressing, cleaning teeth, etc. - Pyogenic granulomas occurring in the proximal nail folds must be curetted under local anesthesia.
References
- Piraccini BM, Lorizzo M. Drug reactions affecting the nail unit: Diagnosis and management. Dermatol Clin. 2007; 25: 215–221.
- Eastwood J.B., Curtis J.R., Smith E.K., et al. Shedding of nails apparently induced by the administration of large amounts of cephaloridine and cloxacillin in two anephric patients. Br J Dermatol. 1969; 81: 750–752.
- Chen H.H., Liao Y.H.: Beau's lines associated with itraconazole. Acta Derm Venereol. 2002; 82: 398.
- De Doncker P., Pierard G.E. Acquired nail beading in patients receiving itraconazole—an indicator of faster nail growth? A study using optical profilometry. Clin Exp Dermatol. 1994; 19: 404–406.
- Miller E.: Levodopa an d nail growth. N Engl J Med. 1973; 288: 916.
- Chapman S., Cohen P.R. Transverse leukonychia in patients receiving cancer chemotherapy. South Med J. 1997; 90: 395–398.
- Shelley W.B., Humprey G.B. Transve rse leukonychia (Mees’ lines) due to daunorubicin chemotherapy. Pediatr Dermatol. 1997; 14:144–145.
- Wantzin G.L., Thomsen K. Acute paronychia after high-dose methotrexate therapy. Arch Dermatol. 1983; 119: 623–624.
- Zerboni R., Angius A.G., Cusini M., et al. Lamivudine-induced paronychia. Lancet. 1998; 351: 1256.
- Blumental G. Paronychia and pyogenic granuloma-l ike lesions with isotretinoin. J Am Acad Dermatol. 1984; 10: 677–678.
- Varotti C., Ghetti E., Piraccini B.M., et al. Subungual hematoma in a patient treated with an oral anticoagulant (warfarin sodium). Eur J Dermatol. 1997; 7: 395–396.
- Ghetti E., Piraccini B.M., Tosti A. Onycholysis and subung ual haemorrhages secondary to systemic chemotherapy (paclitaxel). J Eur Acad Dermatol Venereol. 2003; 17: 459–460.
- Nixon D.W. Alterations in nail pigment with cancer chemotherapy. Arch Intern Med. 1976; 136: 1117–1118.
- Ledbetter L.S., Hsu S. Melanonychia associated with PUVA therapy. J Am Acad Dermatol. 2003; 48: 31–32.
- Hendricks A.A. Yellow lunulae with fluorescence after tetracycline therapy. Arch Dermatol. 1980; 116: 438–440.
- Tosti A, Piraccini BM, Guerra L. Reversible melanonychia due to clofazimine. 18th World Congress of Dermatology, New York, (1992): 183A.
- Hodak E, David M, Feuerman EJ. Excess granulation tissue due to etretinate therapy. J Am Acad Dermatol. 1984; 11: 1166-7.
- West EA, Wong GA. Oxytetracycline onycholysis: case report. Minerva BMJ 334: 644.
- Ferder W, Auerbach R. Purple toes; an uncommon sequela of oral coumarin drug therapy. Ann Inter Med 55: 911-17.
Introduction
Nail manifestations can be a key to systemic disease. Although manifestations of the nails have been seen in different systemic disorders, most of these abnormalities are nonspecific. Although evaluating nails for signs, it is prudent to examine all the nails along with its surrounding tissues.
Interpretation of a nail change will not only hint towards systemic disease but also avoid unnecessary and expensive diagnostic workup. Clinical examination of the nails is important since it may precede, coexist or follow the disease state. Understanding of onychopathology may assist in prognosticating the disease and in proper institution of therapy.
There are no methods regarding clinical examination of nail changes, but several points are worthy of mention:
- A detailed history is important, including close attention to the chronologic sequence of events.
- Always examine all 20 nails because multiple nails are usually involved.
- Examine the rest of the skin and mucous membrane to detect additional abnormalities, and perform a complete physical examination.
- Obtain appropriate laboratory tests as indicated by the history and physical examination.
- Nail pigmentation associated with systemic diseases often arise in the area of the matrix. If this color change is transmitted to the nail plate, it will grow out with structure. By measuring the distance from proximal nail fold to the leading edge of the pigmentation, rate of nail growth (0.1–0.15 mm per day) can be calculated and one can estimate the time at which the initial insult occurred.
Classification
Nail abnormalities in systemic disease can be broadly classified as follows:1
- Nail abnormalities less specifically associated with systemic disease
- Splinter hemorrhages.
- Beau's lines
- Onycholysis
- Pitting
- Koilonychia
- Anonychia
- Nail abnormalities more specifically associated with systemic disease
- True leukonychia—Mee's lines (arsenic poisoning)
- Apparent leukonychia—Muehrcke's lines (hypoalbuminemia), half-and-half nails (renal disease), Terry's nails (hepatic cirrhosis)
- Clubbing—Cardiopulmonary disease
- Nail abnormalities associated with disease of a specific organ system
- Renal disease
- Pulmonary disease
- Gastrointestinal disease
- Cardiovascular disease
- Endocrine disease
- Autoimmune disease
- Infectious disease
- Central and peripheral nervous system disease
- Psychological disease
- Miscellaneous disease
- Nail abnormalities associated with specific syndromes or genodermatoses
Koilonychia
Koilonychia (Greek: koilos, hollow; onyx, nail) (Figures 19.1A and B), commonly called spoon nails, occurs when there is reverse curvature in the transverse and longitudinal axes giving a concave dorsal aspect to the nail. Fingers and toes may be affected, with signs most prominent in the thumb or great toe.1 In infancy it is a benign physiological feature of the great toe-nail but it may persist due to deficiency of cysteine-rich keratin in trichothiodystrophy. In adults it presents as a familial pattern which may be autosomal dominant.2 The most common systemic associations are iron deficiency anemia and hemochromatosis and the others being coronary artery disease, upper gastrointestinal carcinoma and hypothyroidism.1223

Digital Clubbing
(Synonyms—Hippocratic nails, Acropachy, Dysacromelia, Trommelschlagel finger, Digital hippocratism, Watch glass nails, drumstick fingers, parrot-beak fingers, serpent head nails).
Digital clubbing (Figures 19.2A and B) has boggled the minds of clinicians since the days of Hippocrates. Clubbing is characterized by increased longitudinal and horizontal curvature of the nail plate with increase in distal finger tip mass. Clubbing affects the fingernails and toenails. The geometric assessment can be performed by following three forms:
Lovibond's angle is found at the junction between the nail plate and the proximal nail fold, and is normally less than 160°. This is altered to over 180° in clubbing.
Curth's angle at the distal interphalangeal joint is normally about 180°. This is diminished to less than 160° in clubbing.
Schamroth's window (Figure 19.3) is seen when the dorsal aspects of two fingers from opposite hands are apposed, revealing a window of light, bordered laterally by the Lovibond angles. As this angle is obliterated in clubbing, the window closes.2
Stone and colleagues classified clubbing into three categories:2
- Congenital/Hereditary
- Acquired
- Idiopathic


Acquired clubbing is the most important category. Infectious, neoplastic and inflammatory pulmonary problems are most common. Pulmonary problems such as neoplasms of the lung, bronchiectasis, emphysema, pulmonary fibrosis, cystic fibrosis, sarcoidosis, pneumonia and lymphoma are all possible. Cardiovascular etiologies such as bacterial endocarditis, congenital heart/valve disease, congestive heart failure, and aortic aneurysms as do gastrointestinal and hepatic disorders such as cirrhosis, Crohn's disease and ulcerative colitis can be causes of clubbing. Others include endocrine disorders, hypertrophic osteoarthropathy, and human immunodeficiency virus infection. The regional distribution of clubbing will provide clues for diagnosing specific disorders. Idiopathic and congenital categories are less common.
Clubbing can be unilateral or bilateral. Unilateral clubbing is seen in neurologic (hemiplegia) and vascular disorders. Bilateral clubbing has been seen in pulmonary, cardiac, gastrointestinal, infectious, and endocrine diseases.3 In some cases of bronchiectasis, a variant of clubbing, “Shell nail syndrome”, can be seen. This is differentiated from clubbing by the presence of atrophy of underlying bone and nail bed and is seen more commonly in yellow nail syndrome than with clubbing.2
Many hypothesis about the pathophysiology of clubbing have been proposed. Some authors hypothesized that clubbing is associated with increased blood flow in the local arteriovenous anastomosis, provoked by alterations in vascular dynamics that allow blood to bypass capillaries. These anastomosis are neurohumoral end organs that allow the autonomic nervous system to regulate the digital microcirculation. Hypoxia and platelet derived growth factors are also postulated in causing clubbing.4
In new-onset clubbing, it is important to differentiate true clubbing from pseudoclubbing. At first glance, the digit may appear to be truly clubbed, but on closer examination the profile angle is normal in pseudoclubbing. It most commonly involves only a single digit, resulting frequently from a subungual mass.4
Beau's Lines
Beau's lines (Figures 19.4A and B) are transverse grooves in one or more nails due to a nail matrix growth arrest, resulting from trauma or systemic illness.5 They show up first at the cuticle and move distally as the nail grows. Beau's lines are seen more prominently on thumb and great toe 225nails.1

The time of the stressful event leading to Beau's lines can be calculated by measuring the distance of the depression from the proximal nail fold. The duration of the systemic insult can be judged by the width of the groove.4
The causes of Beau's lines can be endogenous or exogenous. When due to an endogenous cause such as drugs, high fever, viral illness, surgery, coronary thrombosis or pneumonia, the Beau's lines have an arcuate margin comparable to that of lunula. When its due to an exogenous cause such as manicures, dermatitis, paronychia, they have a margin comparable to that of the proximal nail fold. A systemic cause should be ruled out if the Beau's lines are present at the same level in all the nails.2
Leukonychia
Leukonychia means “white nails”
Types of Leukonychia4
True leukonychia—abnormalities in distal nail matrix keratinization.
Apparent leukonychia—abnormalities in the nail bed vascularization.
Pseudoleukonychia—nail plate pathology is exogenous.
True leukonychia can be total, subtotal, or partial. Total leukonychia is rare, inherited and porcelain white. In subtotal leukonychia, distal third is pink and proximal two-thirds are white. Transverse and punctate forms are more common forms than the longitudinal form of partial leukonychia.
Mee's nail is a single, transverse, narrow whitish line that runs across the width of the nail plate and can be seen on multiple nails. Arsenicosis is a known cause of Mee's lines. These are usually single but may present as multiple transverse lines. As the pathology lies in the nail matrix, the lines do not disappear on blanching. They are also found in Hodgkin's disease, congestive heart failure (CHF) patients, and patients with carbon monoxide poisoning.1,6
Depending on the clinical presentation, Apparent Leukonychia can be divided into three different types:4 226

- Half-and-half nails
- Terry's nails
- Muehrcke's paired white band
Half-and-half nails (Figures 19.5A and B) or Lindsay's nails are described as having a distal red/brown half and a proximal white half due to changes in the nail bed. Half-and-half nails can be seen in renal insufficiency and uremia. The nails come back to normal when renal function normalizes or following renal transplant.3 All nails are involved.4
Terry's nails (Figure 19.6) are milky white nails extending from the proximal nail fold to the narrow red-brown band in the area of the onychodermal band on the nail. The lunula is usually obscured by the white. Pressure on the nail plate changes the appearance and colour of the nail.5 They are most commonly seen in liver cirrhosis, in up to 82% of patients. The whole nail is affected except for a 1- to 2-mm distal band. All nails are involved uniformly. They are also frequently seen in chronic congestive heart failure and adult-onset diabetes mellitus, peripheral vascular disease, hemodialysis patients, renal transplant patients, and HIV patients.1,4 It is yet to determine whether the variant Neapolitan nails, with bands of white, brown and red, is seen in old age or it is a version of half-and-half or Terry's nails.2

Muehrcke's paired white bands are double white horizontal lines that represent an abnormality of the nail bed vascularization. On squeezing the distal digit they disappear temporarily, only to come back to normal when the pressure is released. Usually the 2nd, 3rd, and 4th fingernails are affected. The most common cause is chronic hypoalbuminemia and the lines disappear when the serum albumin levels drop below 2.2 g/100 ML. Conditions causing hypoalbuminemia like nephrotic syndrome and glomerulonephritis are indicated. Other causes like liver disease, chemotherapeutic drugs, and malnutrition should also be ruled out (Figure 19.7). Muehrcke's bands may be confused with Mee's lines, the difference being that they are fixed in place and disappear with normalization of the serum albumin.1227

Red Lunulas
Red lunulas are nonspecific signs seen in various conditions such as alopecia areata, rheumatoid arthritis, congestive heart failure, pulmonary disorders and carbon monoxide poisoning. The pathogenesis behind the erythema of the lunula is unclear.5
Splinter Hemorrhages
Splinter hemorrhages (Figure 19.8) are small linear dark red/brown lines in the nail bed, oriented in the longitudinal axis and occur in the distal portion of the nail. They are asymptomatic and are the result of small amounts of blood in the longitudinal grooves of the nail bed.5 They are more common in blacks than in whites with a male preponderance and usually involve the thumb and index finger of the dominant hand. Initially, they are plum colored but darken to brown or black within days. The blood attaches itself to the underlying nail plate and moves distally, whereas occasionally it appears to remain stationary, because of attachment to the nail bed. Although trauma is the most common cause, the commonest systemic cause is subacute bacterial endocarditis. Dermatological conditions include several primary nail disorders like onychomycosis and psoriasis.

Simultaneous appearance of splinter hemorrhages in multiple nails proximally near the lunula should indicate an underlying systemic disease. Splinter hemorrhages associated with pain are seen in subacute bacterial endocarditis, indwelling catheters, trichinosis and leucocytoclastic vasculitis.1,7 The major causes of splinter haemorrhages in conjuction with other diseases7 are given in Table 19.1.228
|
Yellow Nail Syndrome
Yellow nail syndrome was first described by Samman and White.1 It is a triad of yellow nails, lymphedema and pulmonary diseases (sinusitis, bronchitis, bronchiectasis, pleural effusion). It is a chronic disorder usually involving all 20 nails which is characterized by an arrest or a reduction in the nail growth (less than 0.2 mm/wk) resulting in nail thickening, hardening, and discoloration. Nail colour varies from pale yellow to orange. Nails are also longitudinally overcurved with a disappearance of the cuticle and absent lunula.4229
The pathogenesis of yellow nail syndrome is unknown, but a congenital abnormality of the lymphatic vessels is postulated, since nail pathology reveals ectatic lymphatics in the nail bed and nail matrix. The nail abnormalities improve or regress when the respiratory disease is treated successfully because of improvement of functional defects in the lymphatics.
In typical syndrome, nail abnormalities are not always present, hence the presence of typical nail alterations should clinch the diagnosis. The duration between the development of the systemic manifestations and nail abnormalities may range from months to years. In patients with paraneoplastic yellow nail syndrome, the nails often return to normal when the tumor regresses. It can lead to secondary onycholysis or onychomadesis. It may also produce a green-to-black discoloration of the nail plate due to colonization by Pseudomonas aeruginosa. Yellow nail syndrome has also been reported in infancy.4
Onycholysis
A distal and/or lateral separation of the nail plate from the nail bed is called onycholysis (Figure 19.9). It can be classified as primary (idiopathic) and secondary. Overzealous manicure, frequent wetting, and cosmetic solvents may be the cause of primary onycholysis. The systemic causes of secondary onycholysis include yellow syndrome, bronchogenic carcinoma, anemia, diabetes mellitus, pregnancy connective tissue disease, porphyrias, shell nail syndrome, and peripheral vascular disease. In thyrotoxicosis, nails are undulated and curved upwards. They are called Plummer's nails and are commonly seen in 4th or 5th finger nail.8
Anonychia
Anonychia describes permanent failure of the nail plate development, which may be complete or partial (micronychia). They can be seen in deafness, onychodystrophy, osteodystrophy and mental retardation (DOOR) syndrome, ectodermal dysplasias, Iso-Kikuchi syndrome and nail patella syndrome.1

Nail Changes Associated with Specific Organ Involvement
Blood groups may be demonstrated from nail clippings and may be important if only hands and feet are obtainable or if mummification has set in. Also a victim's blood-tinged material under an assailant's nails may be important in legal cases.
|
Nail Changes in Renal Disorders
Half-and-half nails are commonly associated with chronic renal disease in 9% to 20% of the patients.
Nail-patella syndrome (NPS), also known as hereditary osteo-onychodysplasia (HOOD), is a genetically determined disease involving organs of both ectodermal and mesodermal origin.
The diagnostic tetrad includes fingernail dysplasia, absent or hypoplastic patellae, the presence of posterior conical iliac horns, and deformation or luxation (i.e. hypoplasia) of the radial heads. Renal disease and glaucoma are now recognized as part of the syndrome. Nail dysplasia include triangular lunulae and ulnar sided nail dystrophy, discoloration, longitudinal ridging, koilonychias, and absent or dystrophic nails. Mees’ lines, Muehrcke's lines, splinter hemorrhages, and slow growth have been associated with renal disease.9
Nail Changes Associated with Gastrointestinal Disease
There are no specific nail findings in gastrointestinal disorders. But some are thought to be specific like Terry's nail.231
|
Azure lunulae are associated with Wilson disease. This discoloration is localized to the lunulae as opposed to a similar colour localized to the nail bed in argyria, with antimalarials, and pseudomonas infections.
Nail Changes in Pulmonary System
Shell nail syndrome exhibits excessive longitudinal curvature of the nail plate, dystrophic finger tips due to atrophy of the distal nail bed and onycholysis.
|
Nail Changes Associated with Metabolic, Hormonal and Endocrine Disorders
Almost all onychopathies associated with endocrine system are non specific. Onycholysis caused by thyroid disease can be distinguished by radiological methods. In general nails are brittle in hormonal disorders.
|
Nail Changes Associated with Malnutrition
Most of the findings are nonspecific. Slow growth and fissuring, koilonychias, spearlike nails, Muehrcke's lines are commonly seen. Vitamin A deficiency associated with egg shell nails and brittle nails have been associated. Chronic, severe hypocalcemia probably can contribute to abnormal nails.
Nail Changes Associated with Central and Peripheral Nervous System
Probably no onychopathy is specific in this group but one. Significant correlation has been noted between a family history of schizophrenia and the visibility of subcapillary plexus in the nail fold.233
|
Nail Changes in Infectious Diseases
|
Nails in Patients with Human Immunodeficiency Virus10
Patients with HIV-positive disease often have numerous cutaneous manifestations. Usually these follow their normal pattern but sometimes may be atypical.
Onychomycosis is common in patients with HIV disease, correlating with helper T cells less than 100 cells/mm3.
Differences from normal patients are:
- May spread rapidly to all finger nails and toe nails.
- Mycotic keratoderma of both palms may be found.
- Proximal subungual onychomycosis often occurs which is unusual in general population, especially in fingernails.
- In immunocompetent, superficial white onychomycosis is rare in fingernails and is usually caused by T. mentagrophytes. In HIV infected it is caused by T. rubrum.
Candida—Candida nail dystrophies are common in HIV-infected patients when the CD4 is less than 100 cells/mm3. Onycholysis and paronychia may occur. Multiple nails are involved. A hypertrophic nail bed candida infection is more typical in HIV infected patients.
Viral infection—Herpetic whitlow has been reported in adults and children with HIV. Papillomavirus may infect the nail unit. Biopsy should be performed to rule out squamous cell carcinoma. HPV type 16 and 35 have been reported.
Scabies—Crusted scabies can occur in patients with HIV infection.
Neoplastic disease—Squamous cell carcinoma, metastatic lesions, and kaposi's sarcoma may appear in the region of the nail.
Systemic disease—there may be a correlation between nail yellowing and pneumocystis carinii pneumonia. Other effects are slow growth, beau's lines, brittle nails, leukonychia.
Systemic drugs—Zidovudine may produce dark brown, bluish, or blackish discoloration of the nail apparatus.
Nail Changes in Autoimmune Disorders (Table 19.8)
|
Nail Changes in Psychological Disorders (Table 19.9)
|
Nail Abnormalities Associated with Specific Syndromes or genodermatoses1 (Table 19.10)
|
Diagnosis1
The nail changes in systemic diseases are diagnosed mostly clinically.
- Mycology: Onychomycosis can be diagnosed by doing a KOH mount.
- Biopsy: Fungal cultures may be required to support the diagnosis of onychomycosis.
- Nailfold capillaroscopy: Nail fold capillaroscopy is the oldest and the best technique for investigating microvascular pathological involvement in rheumatic disease and other collagen vascular diseases. The dermatoscope, on account of its larger field of view, is the preferable capillaroscopic instrument as compared to an ophthalmoscope.
- Radiology: Technetium Tc 99m skeletal imaging which shows increased uptake of the radionuclide, is helpful in determining the presence and extent of bone changes in clubbed digits.
- Thermography and positron emission tomography: These newer imaging studies may be useful for diagnosis and monitoring of nails in systemic diseases.
References
- Singh G. Nails in systemic disease. Indian J Dermatol Venereol Leprol 2011; 77: 646–51.
- Spicknall KE, Zirwas MJ, Clubbing: an update on diagnosis, differential diagnosis, pathophysiology and clinical relevance. J Am Dermatol 2005; 2005(52)6-1020.
- Tosti A, Iorizzo M, Piraccini BM, Starace M. The Nail in Systemic Diseases. Dermatol Clin 24 (2006) 341–347.
- Rich P, Scher RK. An Atlas of Diseases of the nail. New York: The Parthenon Publishing Group; 2005. Chapter 7, Nail signs of systemic disease; p. 95-109.
- Marino MJ. Mees's lines. Arch Dermatol 1990;126: 827–8.
- Saladi RN, Persaud AN, Rudikoff D, Cohen SR. Idiopathic splinter haemorrhages. JAm Acad Dermatol 2004;50 :289-92.
- Jadhav VM, Mahajan PM, Mhaske CB. Nail pitting and onycholysis. Indian J Dermatol Venereol Leprol 2009;75: 631–3.
- Valia RG, Valia AR. Indian Association of Dermatology, Venereology and Leprology textbook of Dermatology, 3rd Edition. Mumbai: Bhalani Publishing House; 2008. Chapter 29, Nail and its disorders; p. 968-978.
- Cribier B, Mena ML, Rey D, Partisani M, Fabien V, Lang JM, Grosshans E. Nail Changes in Patients Infected With Human Immunodeficiency VirusA Prospective Controlled Study. Arch Dermatol. 1998; 134(10):1216–1220.
- Tunc S, Ertam I, Pirildar T, Turk T, Ozturk M, Doganavsargil E. Nail changes in connective diseases: Do nail changes provide clues for the diagnosis? J Eur Acad Dermatol Venereol 2007;21: 497–503.
Anesthesia in Nail Surgery
The choice of anesthesia depends upon the type of procedure and personal preference. The various methods include proximal, distal and transthecal digital anesthesia and various regional blocks.
Distal Nail Blocks
It can be performed in various ways:
- Distal digital block (wing block):1 It causes immediate complete anesthesia of nail unit. A 30G needle is inserted 2–3 mm proximal to the junction of proximal and lateral nail fold (Figure 20.1). It is advanced vertically down and about 0.5 ML of anesthetic is injected. To minimize pain we can raise dermal papule with anesthetic before going deep. The procedure is repeated on opposite side. It can be used unilaterally for isolated procedure on lateral margins.238Figure 20.1: Distal digital block (wing block). A 30G needle inserted 2–3 mm proximal to junction of proximal and lateral nail fold
- Distal anesthesia through proximal nail fold (PNF):2 It is for anesthetizing PNF, matrix and the proximal bed. The needle is inserted right in center of PNF, and 0.5–1 ML of anesthetic is injected slowly (Figure 20.2). We can observe blanching of lunula and nail bed as injection is being done. It can be used in children and small toes.
- Distal anesthesia through hyponychium: This is used rarely, as it is painful. It anesthetizes hyponychium, nail bed and most of matrix. The needle is advanced from lateral part of hyponychium horizontally along the nail bed and injected while observing for blanching of nail bed and matrix (Figure 20.3).The advantages of distal nail blocks are it gives immediate anesthesia, carries low risk of neurovascular compromise as major digital vessels and nerves are not transected, and compression hemostasis due to addition of volume in tight compartment. However, it cannot be used in case of local infection and vasculopathy.


Proximal Nail Blocks
The proximal digital blocks are preferred by many surgeons. This is done in a variety of ways. It includes penetration of skin on lateral side of each finger where digital nerve lies and injecting 239the anesthetic.

The old technique of “complete ring block” is not preferred now a days. Plain 2% lignocaine is preferred. A 30G needle is introduced at the base of the finger (Figure 20.4A) and advanced laterally to place the anesthetic along ventral and dorsal digital nerves (Figure 20.4B). One to two ML of anesthetic is used along each collateral nerve. It is mandatory to wait for 10–15 min to ensure complete anesthesia.
Transthecal Digital Anesthesia3
Flexor tendon sheath can be used to introduce anesthetics to the core of the digit. This technique was described by Chiu et al in 1990. After a palmar percutaneous injection, the anesthetic diffuses to the dorsal digital nerves via centrifugal infusion through the flexor tendon sheath and by local diffusion around the puncture site. This is mainly used for anesthetizing central three fingers.
The hand is placed in supine position, flexor tendon sheath is identified by doing flexion and extension of finger desired to be anesthetized. A 27G needle is advanced just distal to metacarpo-phalangeal joint and after passing through subcutaneous space, flexor tendon sheath is entered where 3–5 ML anesthetic is injected (Figure 20.5).

Figures 20.4A and B: Proximal nerve block. (A) A 30G needle is introduced at the base of the finger; (B) Needle is advanced laterally to place the anesthetic along ventral and dorsal digital nerves

Figure 20.5: Transthecal block. A 27G needle is advanced just distal to metacarpo-phalangeal joint and after passing through subcutaneous space
Plain 2% lignocaine is preferred; however, bupivacaine can be used for longer effect. It takes 7–8 minutes to anesthetize the digit.
The advantages include single prick, no neurovascular compromise and long lasting effect. However, it doesn't work for anesthesia of 1st and 5th finger. The disadvantage is discomfort while penetrating palmer skin and sometimes focal pain at site of injection for few days.
Regional Blocks
It is indicated for advanced nail surgeries. It includes wrist blocks, individual ulnar, radial or median nerve blocks for fingers; anterior or posterior ankle blocks for toes.
Instruments
Most of the instruments used for nail surgery are not specific, but few instruments deserve to be mentioned. The instruments used in nail surgery needs to be delicate so as to minimize trauma to the tissue.
The nail plate avulsion needs some special instruments like nail elevators, nail nipper or nail splitter. For partial nail avulsion Lempert elevator 2 mm or 3 mm are used, to separate nail plate the nail bed. They are slightly curved to take the shape of nail plate while introducing from distal end to avoid trauma to nail bed. The complete nail avulsion requires larger Freer septum elevator (Figures 20.6A and B).
Nail nippers are used to cut the nail plate in partial nail avulsion. The most commonly used are English anvil-action nail nipper or Ruskin bone-cutting forceps (Figure 20.7). They are introduced from distal end and advanced proximally till end of nail plate is reached and nail is cut.241


Sutures
The approximation of skin can be done with 5-0 Prolene or Ethilon. Nail epithelium approximation is performed with absorbable sutures. Undyed (clear) coated Vicryl (polyglactin 910) suture or PDS II (polydioxanone) synthetic absorbable suture are preferred for nail bed and nail matrix approximations. We prefer 6-0 for matrix suturing and 5-0 for nail bed. Vicryl has advantage because of ease of knot tying, knot security, and knot sliding capabilities.
Tourniquet and Hemostasis
One of the requirements for nail surgery is bloodless operating field. In minor nail surgery this can be achieved by asking assistant to apply pressure at the lateral side of base of digit, to block the blood vessels temporarily.
In major surgeries, a digital tourniquet can be applied. A simple technique is to use sterile glove whose tip has been removed. It offers advantage as while rolling the glove back exsanguination can be achieved as well as sterility of operating area is ensured (Figure 20.8).242

References
- Salasche SJ, Peters VJ. Tips on nail surgery. Cutis 1985;35: 428–438.
- Abimelec P, Dumontier C. Basic and Advanced Nail surgery Part 1 Principles and techniques. In: Scher R, Daniel CR: editors. Nail Daignoses Therapy Surgery. 3rd Edition. USA: Elsiver Saunders; 2005. p.266-267.
- Chiu DTW Transthecal digital block: flexor tendon sheath used for anesthetic infusion. Journal of Hand Surgery 1990;15A: 471-473.
To perform successful nail surgery, a comprehensive understanding of nail anatomy, physiology, vascular and neural pathways supplying the nail complex and the functions and relationship of each component of the nail unit is essential. The nail surgeon should be equipped with knowledge of nail pathology, surgical techniques and instrumentation, anesthesia, preoperative evaluation, management of complications, wound care and healing after surgery.
Indications
There are multiple indications for surgical exploration of the nail unit, which include:
- Infections: bacterial paronychia
- Inflammation: psoriasis, lichen planus, etc.
- Congenital nail dystrophies, ingrown nails, onychogryphosis
- Neoplasms
- Traumatic causes.
- Informed written consent of the patient after explaining the surgical procedure in vernacular language should be taken.
- Detailed history regarding other metabolic disorder like diabetes mellitus, peripheral vascular disorders, bleeding disorders, and connective tissue disorders should be taken.
- History of drug intake by the patient like anti-coagulants, aspirin or vasodilators to avoid excessive bleeding during surgery, or corticosteroids leading to delayed wound healing.
- History of known hypersensitivity to anesthetic agents or vasoconstrictive drugs which would be used during surgery.
Nail Avulsion
Nail avulsion is the most common surgical procedure performed on the nail unit. It is the excision of the body of the nail plate from its primary attachments, the nail bed ventrally and the proximal nail fold (PNF) dorsally. Avulsion of the nail plate may be initially performed to allow full exposure of the nail matrix before chemical or surgical matricectomy.4,5,6 Other indications for performing nail avulsion are to treat recalcitrant onychocryptosis; to excise tumors of the nail unit; to allow full examination and exploration of the nail bed, the nail matrix, the PNF and the lateral nail fold (LNF), and the nail grooves for the presence of pathology; or to use as a preliminary step before performing biopsy on the nail bed and the nail matrix.
The 2 primary methods for performing nail avulsion are distal avulsion1,7–9 and proximal avulsion.1,10–12 A third method, chemical avulsion with urea paste, is a nonsurgical avulsion technique that may be performed. A partial or complete nail avulsion can be performed, depending on location and extent of the disease. In distal nail avulsion, the nail spatula is introduced under the distal free edge of the nail plate to separate it from the underlying nail bed. There is significant resistance till the matrix is reached, after which the surgeon feels a sudden loss of resistance. The nail spatula is reinserted with several forward and backward strokes until the nail bed is completely freed from the overlying nail plate. The nail plate is similarly freed from the proximal nail fold. Using an artery forceps, the nail plate is gently twisted until it becomes free of all the lateral and proximal nail folds (Figures 20.9A to E).
Proximal nail avulsion is done when there is distal nail dystrophy as seen in distal subungual onychomycosis. Here, the spatula is first inserted below the cuticle in the proximal nail groove to separate the nail plate from PNF, and is advanced distally till it reaches the distal edge of the nail plate, that is then removed using artery forceps as in proximal nail avulsion (Figures 20.10A to F).

Figures 20.9A to E: Distal nail avulsion (Courtesy: Department of Dermatology, BMCRI). a. Separation of distal nail plate, B. Releasing the nail plate from the sides, C. Separation of proximal nail fold, D. Removal of nail plate with artery forceps, E. Nail bed after complete nail avulsion

Figures 20.10A to F: Proximal nail avulsion (Courtesy: Department of Dermatology, BMCRI). A. Dystrophic nail, B. Retraction of proximal nail fold with skin hooks, C. Separation of nail plate proximally, D. Insertion of nail elevator proximally, E. The nail elevator has traversed through the nail plate, F. Avulsed nail plate
Surgery for Warts
Cryosurgery by using liquid nitrogen is used to freeze the warts. 10% salicylic acid with occlusion is applied 3 days prior to cryosurgery to the wart to accentuate freezing with liquid nitrogen.15,16 After ring block to the digit, liquid nitrogen is applied by a spraying action. The freeze-thaw time is 30–45 seconds after which another cycle is given for a total of 2–3 cycles.16 The patient may experience pain due to edema under the nail bed. Freezing of the proximal nail bed should be limited to avoid permanent damage to the underlying nail matrix.
Electrosurgery
It is the application of low-voltage current by means of electrodesiccation and enucleation to dehydrate and detach the wart from the dermis. After administering a local anesthetic, the nail plate is debrided to visualize the wart. In the first step (electrodesiccation), a needle is directly applied to the surface of small warts or intralesionally applied to larger, thicker warts under low-voltage current.4 The current burns and vaporizes the contents of the wart.
In the second step, the charred tissue is removed with a curette, carefully avoiding the dermis and the nail matrix to prevent scarring (enucleation). A smoke evacuator is used to remove infectious airborne viral particles. Healing occurs in 3–4 weeks. Potential complications of this procedure include thermal injury to surrounding soft tissues and the adjacent bony phalanx and significant scarring.16246
Bleomycin Treatment
The intralesional injection of bleomycin (1 μm/mL), mixed with sodium chloride solution is highly effective in controlling recalcitrant warts. Before treatment, ring block is given to control the pain associated with the injection. Bleomycin is contraindicated in women of reproductive age. Rarely nail dystrophy, local necrosis, scarring, and local Raynaud phenomenon in patients with previous vascular insufficiency may be seen.16
Laser Treatment
The carbon dioxide laser, Nd:YAG laser and flashlamp pulsed dye laser are beneficial in patients with multiple infected digits and in immunocompromised patient in the treatment of periungual and subungual warts as well as plantar warts.17
Thermal injury to the nail matrix may occur because periungual warts usually involve the PNF overlying the proximal matrix. Hypertrophic scarring and permanent onycholysis of the nail plate may be seen in excessive thermal damage to the nail bed.18
Paronychial Surgery
The paronychial region is defined by the PNF, the LNF, the nail walls, the distal cuticle; and the ventral eponychium. It prevents infection and inflammation from reaching the proximal nail matrix. Perionychium can be involved in acute and chronic paronychial infections, periungual and subungual verrucae, deep fungi, atypical mycobacteria, myxoid cysts, foreign body and pyogenic granulomas and tumors.4
In acute paronychial abscess, surgical management is indicated if antibiotic therapy fails. Pockets of collected pus can extend around the base of the nail under the PNF and inflame the nail matrix. The pus may dissect the nail from its proximal attachment and pressure necrosis can develop within 48 hours leading to nail dystrophy if surgery is delayed.
After giving ring block, a small incision is made parallel to the nail fold and directly over the collection of pus to drain the abscess. Formed septa in the abscess base are destroyed by using the tip of a curved artery forceps.4 If infection spreads under the distal nail bed, excision of the entire nail base along with distal avulsion is performed to expose the nail bed, and debridement is done.
Matricectomy
Matricectomy is the process of surgically, chemically, or electrically ablating or destroying the nail matrix. The nail matrix is the germinative epithelium that forms the nail plate by means of the continuous differentiation of its basal cells. Complete excision of the viable nail matrix results in loss of the nail plate.
Indications
- Onychogryphosis (ingrown toe-nails).
- Chronic nail dystrophies, such as onychauxis, onychogryphosis, onycholysis, psoriatic nail, onychomycosis that is unresponsive to aggressive antifungal therapy.
- Painful nail conditions, including pincer nail deformity.4
Complete matricectomy is reserved for cases of chronic or severe nail dystrophy. Partial matricectomies are especially useful in the management of persistent onycholysis and onychocryptosis.
Before matricectomy, the preoperative evaluation should include a medical history and physical examination to exclude patients with documented small and large vessel occlusive disease (e.g. atherosclerosis, diabetes mellitus, collagen vascular disease) in whom, because of delayed healing, this type of surgery is considered to be relatively contraindicated. Patients presenting with claudication, absent distal pulses on palpation and Doppler examination, poor capillary refill, poor wound healing, or low oxygen saturation should be excluded.19 Matricectomy should be deferred until all acute infection of the digit and paronychial tissues has resolved.
Matricectomy can be performed by using surgical, chemical, or electrical modalities. Ablative matricectomy involves the use of chemocautery, electrocautery, or laser19 to destroy the nail matrix. Excisional matricectomy uses cold steel surgery, cutting electrosurgery, or cutting laser to remove the matrix.
When performing a partial matricectomy, the digit is first prepared in a sterile environment and anesthetic is administered through a digital block. Hemostasis is achieved using a tourniquet.
A partial nail avulsion is performed. The PNF is reflected back to allow full visualization of the matrix.
After avulsion, a scalpel blade is used to make 2 longitudinal incisions, measuring 4 mm in width, beginning at the distal edge of the nail to include the hyponychium and advancing proximally. The nail bed, the nail matrix, and the lateral aspect of the PNF are excised. The incision also extends to include the LNF and the lateral matrix horn in the lateral nail groove. The surgical sample is a wedge of tissue containing the nail-producing components of the nail unit. Fine scissors are used to remove the tissue sample. After obtaining the sample, the PNF is repositioned to its original anatomical site. Hemostasis is achieved and the wound allowed to heal by secondary intention. Alternatively, the wound may be closed by passing sutures through the nail plate and the LNF. After surgery, the nail plate remains functional. As a result of partial excision of the nail matrix, the newly formed nail plate is narrower.
In total matricectomy, the entire nail plate is avulsed. A scalpel is used to make 2 incisions oriented proximally and laterally; these incisions extend to the PNF and the LNF. The PNF is dorsally reflected to allow full exposure of the nail matrix, including the lateral matrix horn area. During matricectomy, the first incision is made about 1 mm distally to the distal border of the lunula and is carried 4–5 mm proximally under the PNF in the proximal nail groove to include all matrix tissue. The excised matrix is removed with fine scissors. Sutures are used to place the PNF into its normal position. Hemostasis is controlled by direct pressure and electrocoagulation. After surgery, the extremity should be elevated to reduce subsequent pain and swelling. Systemic pain killers and broad spectrum antibiotics should be given to avoid delayed healing and secondary infection.
Chemical Matricectomy
Chemical cauterization of the nail matrix with the application of phenol is used to partially or permanently destroy the matrix. Phenol matricectomy is the most widely practiced procedure.4,19 Phenol denatures protein and retains antibacterial and anesthetic properties.20
After unilateral, partial bilateral, or total nail avulsion is performed under digital block, curettage of the hyponychium, the lateral nail groove, the lateral matrix horn, and the proximal 248matrix is done. Curettage lowers the rate of recurring nail spicules in the lateral nail horn area, resulting in higher cure rates and a better treatment outcome.19 Before applying phenol, the surrounding soft tissues are covered with petroleum jelly to protect them against chemical damage and resulting chemonecrosis. A supersaturated solution of 88% phenol is used. A total of three 30-second applications of phenol are required in partial matricectomy and five 30-second applications are used in complete matricectomy.4 A sterile cotton-tipped applicator dipped in the concentrated phenol solution is directed laterally into the recessed area of the lateral matrix horn and dorsally to contact the matrix tissue on the ventral surface of the PNF (Figures 20.11A and B).
During the procedure, the cotton applicator is used to vigorously massage the matrix with a twisting motion.19 After phenol application, lavage of the treated area is performed by using 70% isopropyl alcohol to neutralize the concentrated phenol. Sodium chloride solution, boric acid, or 3–5% acetic acid may also be used to neutralize phenol. Antiseptic pressure dressing is applied to the wound. The dressing is removed in 24 hours after a warm-water soak, and the wound is cleansed in diluted hydrogen peroxide solution. This procedure is the standard wound care used in all types of matricectomy procedures. The patient is instructed to perform dressing changes twice daily for 2–3 weeks.
Phenol matricectomy has a success rate of 95% and higher4,19 and postoperative morbidity is minimal. However, the associated risks of performing this procedure include pain, frequent recurrence, periostitis, unpredictable persistent wound drainage, and extended healing times.19 The wound usually heals completely within 2–4 weeks by secondary intention.
Chemocauterization of the nail matrix is contraindicated in patients with vascular disease. A newer approach to chemocauterization of the nail matrix involves the use of 10% sodium hydroxide.19 Chemocauterization of the nail matrix with sodium hydroxide is similar to the phenol alcohol method.
Ablative Matricectomy
The diseased portion of the nail plate is avulsed, followed by vigorous curettage of the exposed matrix and its lateral horn. Electrodesiccation of the area curetted is performed. Electric current is applied twice to the treatment site for 5 seconds to ensure complete destruction of all matrix tissue.18 A cooling period of 10–20 seconds should occur between treatments. Hemostasis is provided by means of electrocoagulation. A potential complication of this method is thermal destruction of the nail folds, the surrounding periungual tissues, and the underlying bony phalanx.

Figures 20.11A and B: Partial nail avulsion with chemical matricectomy (Courtesy: Department of Dermatology, BMCRI). A. Partial nail avulsion, B. Chemical matricectomy with 88% phenol using a tooth pick
Carbon dioxide laser vaporization matricectomy is associated with minimal postoperative morbidity, protracted healing time, decreased edema and inflammation, and absence of extensive necrosis of the adjacent dermal tissue.19
After laser, an antibiotic pressure dressing is placed over the digit. The surgical site heals by secondary intention, and healing is rapid with minimal patient discomfort.
Radical Matricectomy
Radical matricectomy (Syme procedure) is the radical en bloc excision of the entire nail complex. This procedure is reserved for patients with symptomatic, recurrent onychocryptosis that is refractory to repeated treatments of total nail matricectomy. The plantar flap formed from amputation of the distal half of the terminal phalanx is sutured dorsally over the defect created from the excision of the nail bed and the nail matrix for primary wound closure.19 Radical matricectomy has a success rate of almost 100%, with low postoperative morbidity, despite the poor cosmetic and functional outcome.1
Surgery of Myxoid Cysts
Myxoid cysts are usually asymptomatic. However, surgical removal of the cysts is indicated when they become large and cause pressure on the underlying matrix, resulting in longitudinal nail deformities, such as splitting of and ridging on the nail plate. Other indications for surgery include pain, persistent drainage, and development of secondary infection. Conservative treatment may initially be attempted with intralesional corticosteroid injections, by freezing with cryotherapy and as well as injection of scleroscant.4 When conservative measures prove unsuccessful, elective en bloc excision of the PNF is performed. The goal during surgery is to perform a full-thickness excision of the PNF that includes symmetric small portions of the LNF.
Standard preparation of the digit is performed under sterile conditions. Ring block is given and hemostasis is achieved. A nail spatula is placed in the proximal nail groove to help define the proximal extent of the cyst and to direct movement of the scalpel.4 Hemostasis of the wound may be achieved by spot electrodesiccation.
Antibiotic dressing is applied over the wound. The wound is cleansed twice daily with dilute hydrogen peroxide followed by the application of an antibiotic ointment and a replacement of the dressing (Figure 20.12).
Surgery of Pyogenic Granulomas
Surgical management of the granuloma is by means of an excision. An electrocauterizing unit or a scalpel is used to perform the excision at the base of the lesion. The excised material is sent for histopathological examination to confirm the diagnosis. A newer conservative approach for treatment is by use of intralesional injection of sclerosants such as 3% sodium tetradocyl sulphate or polidocanol (Figure 20.13).
Surgery of Fibrokeratomas

Figures 20.12A to E: Excision of myxoid cyst (Courtesy: Department of Dermatology, BMCRI). A. Swelling on the proximal nail fold causing nail dystrophy, B. Retraction of proximal nail fold to reveal myxoid cyst, C. and d. Dissection of the cyst, E. The incisions closed primarily with sutures

Figures 20.13A and B: Sclerotherapy for pyogenic granuloma (Courtesy Department of Dermatology, BMCRI). A. Pyogenic granuloma, B. Near complete resolution 2 weeks after sclerotherapy
Surgery of Glomus Tumors
Smaller glomus tumors are excised by creating a 6-mm punched out hole in the nail plate. An incision is made through this hole, enucleating the tumor from its fibrous covering and incising the nail bed tissue. The punched out nail disc is replaced to function as a physiologic dressing. Surgical treatment of larger glomus tumors is proximal nail avulsion. The matrix and the nail bed are incised and elevated from the periosteum and the tumor is excised. A nonadhesive 251gauze pad is placed on the wound to prevent the formation of adhesions between the nail bed and the skin fold. Standard wound care is necessary after surgery.
Surgery of Basal Cell Carcinoma, Squamous Cell Carcinoma, and Melanoma
Surgical management of basal cell carcinoma, SCC, and melanoma involves excision of the tumor with clear margins if bone metastasis is absent; this is usually accomplished by Mohs micrographic surgery. The surgical site is covered with a skin graft, and the patient is closely monitored for recurrence. If bone metastasis has occurred, the extremity is amputated at the distal interphalangeal joint (DIP) joint or more proximally.21
Mohs micrographic surgery has been recommended in the treatment of well-differentiated, potentially aggressive tumors of the nail unit.22 The Mohs technique of horizontal sectioning allows examination of 100% of peripheral and deep tissue margins of the specimen, resulting in the smallest possible defect and the highest possible cure rates.
The benefits of applying Mohs micrographic surgery in treating nail unit tumors include the following:
- The Mohs technique is a nail-sparing procedure that provides high cure rate.22 The treatment outcome is excellent in cases of localized disease.
- Mohs micrographic surgery is ideal for obtaining tumor-free margins, while maximally preserving the integrity of the surrounding healthy tissues.22
- The Mohs surgical technique is both diagnostic and therapeutic.
- The Mohs micrographic technique is an alternative to amputation by providing the option of preserving the nail unit and maintaining digital function in cases where the tumor has not yet invaded the underlying deep structures.
Complications
All nail surgeries may have complications, that depends upon the type of procedure. The complications of nail surgeries are:
- Pain and swelling: This is the most frequently observed complication. Postoperative analgesics can help to relieve pain. The delicate handling of tissue, non over compressive bandage and postoperative elevation of hand can help to reduce swelling.
- Hematoma: It should be avoided as it is painful and may lead to secondary infection. Proper nail plate repositioning and compressive dressing will help to avoid this complication.
- Necrosis: The fingertip or toe-tip necrosis is reported due to failure to remove the tourniquet after surgery.
- Infection: Most infections follow postoperative hematoma or necrosis. It can be treated with proper antibiotics after culture. All local infections must be taken care of before taking patient for nail surgery.
- Other rare complications include pyogenic granuloma, inclusion cyst, reflex sympathetic dystrophy.
Nail surgeries are delicate procedures requiring special training. Lack of skills and knowledge leading to inappropriate intervention cannot be labelled as complication.252
References
- Siegle RJ, Swanson NA. Nail surgery: a review. J Dermatol Surg oncol 1982;8:659–66.
- Fleckman P, Allan C. Surgical anatomy of the nail unit.. J Dermatol Surg. 2001;27:257–60.
- Baran R, Haneke E. Surgery of the nail. Skin surgery ( Epstein E, Epstein E Je eds) 6th ed. Philadelphia: WB Saunders Co. 1987:534-47.
- Salasche SJ. Surgery. In: Scher RK, Daniel CR, eds. Nails: Therapy, Diagnosis, Surgery. Philadelphia, PA: WB Saunders; 2005:326-49.
- Lai WY, Tang WY, Loo SK, Chan Y. Clinical characteristics and treatment outcomes of patients undergoing nail avulsion surgery for dystrophic nails. Hong Kong Med J. Apr 2011;17(2):127–31.
- Han D, Li QF. New technique for nonmicrosurgical reattachment of avulsed fingertips in adults. J Plast Surg Hand Surg. Nov 2010;44(4-5):204–8.
- Scher RK. The nail. In: Roenigk RK, Roenigk HH, Ratz JL, eds. Dermatologic Surgery-Principles and Practice. New York, NY: Marcel Dekker; 2006:281-88.
- Dawber RP, Baran R. Nail surgery. In: Samman PD, Fenton DA, eds. The Nails in Disease. Boston, Mass: Butterworth-Heinemann; 1994:209-21.
- Scher RK. Surgical avulsion of nail plates by a proximal to distal technique. J Dermatol Surg Oncol. Apr 1981;7(4):296–7.
- Zaias N. The Nail in Health and Disease. Norwalk, Conn: Appleton & Lange; 1990.
- Dawber RP, Baran R. Diseases of the Nail. Oxford, England: Blackwell Science; 1994.
- Scher RK. Nail surgery. In: Epstein E, Epstein E JR, eds. Techniques in Skin Surgery. Philadelphia, PA: Lea & Febiger; 1970:164-70.
- South DA, Farber EM. Urea ointment in the nonsurgical avulsion of nail dystrophies--a reappraisal. Cutis. Jun 1980;25(6):609–12.
- Averill RW, Scher RK. Simplified nail taping with urea ointment for nonsurgical nail avulsion. Cutis. Oct 1986;38(4):231–3.
- Norton LA. Tumors. In: Scher RK, Daniel CR, eds. Nails: Therapy, Diagnosis, Surgery. Philadelphia, PA: WB Saunders; 2005:262-75.
- Clark RE, Madani S, Bettencourt MS. Nail surgery. Dermatol Clin. Jan 1998;16(1):145–64.
- Geronemus RG. Laser surgery of the nail unit. J Dermatol Surg Oncol. Aug 1992;18(8):735–43.
- Borovoy MA, Borovoy M, Elson LM, Sage M. Flashlamp pulsed dye laser (585 nm). Treatment of resistant verrucae. J Am Podiatr Med Assoc. Nov 1996;86(11):547–50.
- Ceilley RI, Collison DW. Matricectomy. J Dermatol Surg Oncol. Aug 1992;18(8):728–34.
- Rinaldi R, Sabia M, Gross J. The treatment and prevention of infection in phenol alcohol matricectomies. J Am Podiatry Assoc. Sep 1982;72(9):453–7.
- Herndon JH, Myers SR, Akelman E. Advanced surgery. In: Scher RK, Daniel CR, eds. Nails: Therapy, Diagnosis, Surgery. Philadelphia, PA: WB Saunders; 2005:350-62.
- Goldminz D, Bennett RG. Mohs micrographic surgery of the nail unit. J Dermatol Surg Oncol. Aug 1992;18(8):721–6.
Introduction
Fantasy has entered nail fashions in recent years. Both women and men can be disturbed by nails that split, chip, and break which may affect employability, self-esteem, and interaction with other people. Moreover, any abnormality of the nail can cause impaired function of the hand or foot. Nail cosmetics is gaining popularity among dermatologists as they can improve the condition and appearance of the nails if used wisely. Since the nails are often difficult to treat and takes longer time to respond, nail cosmetics may be an effective support to medical treatment. They may help the patients to cope with their nail dystrophies while waiting for treatment to show its efficacy. It may also be the only choice to hide irreversibly damaged nail. Although, their popularity is greatest among women, the market for male manicures is also growing rapidly. The adornment and grooming of nail is an enormous industry, with over US $ 6 billion spent annually at nail salons in the US alone.1 Although, we do not have this data in India, it is well known that the nail salons is mushrooming rapidly in Indian metro cities. Nails are painted with exotic colors and designs. Ornaments and even expensive jewels are used to decorate the nails. Nails have thus created a great deal of interest among people as well as among cosmetic industries. However, injudicious use of nail cosmetics and nail grooming tools itself may result in adverse reactions promoting nail disorders and sometimes even deformities. This can be a 254constant source of concern for the physician. Hence, dermatologists must be familiar with nail cosmetics, develop the ability to recognize possible cosmetic etiology in nail disorders and to know the clinical usage of these nail cosmetics in nail disorders.
Familiarity with nail anatomyis essential before one can understand nail cosmetics. Readers are suggested to refer chapter on ‘Basic Science’ for details.
History of Nail Art
Ancient women used to strive for beauty and were eager to discover various means to capture the imagination of men. It is due to this factor that nail art origins were concentrated mainly in the sphere of men-women relations. History dates back to 5000 years ago when henna was used for the first time for manicure in India. Nail art origins are traced from the term mehendi, used synonymously for henna, derives its name from the Sanskrit word mehandika. In ancient India when a young girl has had her first menstrual cycle, she was considered ready to enter into a marriage and this was when her lips and finger nails were painted bright red henna. Much of the modern revival of henna which is well-appreciated worldwide today derives from its popularity in India.
Ancient Egyptians were very nail conscious, and Kings and Queens colored their finger and toe nails ruby red. Cleopatra used to use henna to tint her nails (Figure 21.1). Archaeologists have found many solid gold manicure tools in Egyptian tombs.
Traced back to 3000 B.C., the first nail polish has been used in China. During the 17th century, the upper class in Chinese society used finger nails to demonstrate their wealth. Empress Dowager Cixi, the last empress of China, grew her thumb nails about an inch long which were far longer than the rest of her fingernails (Figure 21.2).
The whole nail art history may also surprise those who use them: nail polish, for example, can contain the shimmery substance of fish scales called “pearl essence”. Nail art origins indicate, that pearl essence is obtained primarily from herring and is one of many by-products of large-scale commercial fish processing. Modern nail art trends include the primary source of the pearl escent shine used in artificial nails, that is a natural, mined mineral.


French Revlon company founded in 1932, started with a single product—a nail enamel and subsequently developed a unique manufacturing processes. Soon Revlon was able to offer women a rich-looking, opaque nail enamel in a wide variety of shades. The nail salon industry grew quickly in the late 1970s and flourished during the 80's and early 90's. Modern nail art trends are fascinating and innovative. Fancier manicures include painting pictures or designs on the nails or applying small decals or imitation jewels. Pure carmine dye is usually more expensive than gold!
Nail Implements
Nail implements are mechanical objects used in the physical manipulation of the nail plate and surrounding structures of the nail unit.2 Commonly used implements are shown in Figure 21.3 of which few need description.
- Emery boards (E on Figure 21.3): They have a coarse side, which file down the nail plate and have a fine side, which bevel the surface.
- Nail brushes and buffers: They are used to cleanse and polish the nail.256Figures 21.3A to F: Nail implements: (A) Cuticle trimmer; (B) Cuticle cutter; (C) Cuticle Pushers; (D) Nail nipper; (E) Emery boards; (F) Clipper
- Orange wood sticks (Figure 21.4) and cuticle pushers: They are firm implements that loosen the cuticle and push it back from the nail plate.
- White pencil (Figure 21.5): Used often to color the underside of the free edge of the nail plate.

Adverse Effects
- Many nail salons uses only soapy solutions to sterilize them between each use and such improper sterilization practice may lead to transmission of bacterial, fungal, or viral infections including the dreaded blood-borne viral infections.3 When emery boards are used to file nails of digits affected with verruca, it can result in spread of virus particles to other locations on the hand/foot or to other clients.Measures to Prevent Infections
- Clean the instruments in an ultrasonic cleaner, then soak them for atleast 10 min in a cold sterilization solution (2% glutaraldehyde or benzyl alconium chloride).4
- The porous implements like emery boards cannot be sterilized because they do not survive soaking or autoclaves.5 Emery boards, files and orange sticks should be disposable or the users should bring their own implements to the salon.
- Injury to any of the structures of the nail unit during handling these implements, may result in temporary or sometimes permanent deformities. Common deformities include:
- Trauma to nail matrix which may cause scarring, longitudinal (may be permanent scar) or transverse furrows (may be temporary) in the nail plate.
- Injury to cuticle while pushing it back may cause paronychia, Beau's lines, striate or punctate leukonychia. Use of cotton–tipped applicators may minimize this trauma.
- High-speed electric drills are occasionally used to file nails rapidly. These drills can injure the periungual and subungual tissue and the file bit is often used for weeks at a time on numerous users without cleaning, creating a high-risk situation.5


Nail Grooming/Manicure
Professional grooming of the nails is known as manicure (grooming of finger nails) and pedicure (grooming of toe nails). The word “manicure” comes from the Latin word manus, meaning “hand,” and cura meaning “care”.
Procedure4
- Hands are first soaked in a warm water and soapy solution to soften the nail plate and cuticles.
- Nails should be trimmed with as slight a curve as possible and with the corners left untouched to avoid ingrown and paronychia. The free edge should be filed in only one direction with a nail file. Ideally, nails should be shaped with the sides straight and the tops gently rounded which are stronger than pointed nails. Unfortunately, many people do not prefer to have cuticle and try to cut it (Figure 21.6). It is highly recommended not to cut cuticle to avoid Beau's lines and paronychia. Few individuals try to push their cuticle proximally with an orange stick or a metallic cuticle pusher. The latter is more likely to cause injury to proximal nail fold and hence should be strongly discouraged.
- A base coat, color enamel, and top coat can then be applied over the nail plate.
Nail Grooming Techniques
They can be categorized as:

Nail Coats/Enamels
Nail enamel is the preparation which not only enhances the appearance of the nail by adding color but also acts as protectant in preventing dryness due to contact with water and detergents.
- Nail enamel:2 It provides color to the nail and is known by synonyms like nail lacquer, varnish and polish.
- Base coat: It is usually transparent, fills in irregularities of the nail plate and provides a uniform, neutral color as the starting point for the pigmented nail polish. They contain more resin for better adherence.
- Top coat: It is a clear enamel that adds gloss and prevents premature chipping.6 Top coats contain more nitrocellulose and plasticizer to improve gloss and are abrasion resistant.
- Nitrocellulose: It is a film former and is nonsensitizing. Its other important properties are stability, physical strength, and water insolubility. It forms shiny film that adheres to the nail plate.
- Thermoplastin resin: It is composed of toluene sulphonamide formaldehyde resin (TSFR)which improves adhesion, gloss, and flow of the enamel.
- Plasticizers: It is made of dibutyl phthalate and camphor which provide flexibility, prevents shrinkage, enhance adhesion, prolong wear by softening and plasticizing the nitrocellulose to prevent wrinkling and distortion of the enamel.
- Solvent extender: Solvent extenders forms more than 70% of the enamel. They include toluene, butyl acetate, ethyl acetate, or isopropanol. They maintain liquidity thus allowing the other components of the polish like resin, film former, and plasticizer remain liquid.
- Pigment: It is colorant that contributes to the color of the enamel and sometimes, give sheen, fluorescence, or sparkle. They contain insoluble organic colors as well as titanium oxide or iron oxide. Few soluble organic dyes are used to tint colorless polishes. The nacreous pigments guanine, bismuth oxychloride, and mica are added to pearlized polishes.
- The proportions of these five basic components determine whether a product will be useful as a base coat, enamel, or top coat. Table 21.1 summarizes the components of nail coats.
- Additional ingredients
Advantages
Nail polish may act as a protectant in preventing contact with water and detergents and may slow down evaporation of water from the nail plate from 1.4 to 0.6 mg/cm2 per hour, thus enhances nail moisturization and flexibility. Drying may instead be due to nail polish removers that are usually acetone-based solvents.9 A layer of enamel can add about 5% to a nail's strength. 259
|
Adverse Effects
Contact dermatitis to nail polish is a well-documented phenomenon (1–3% of the population may be affected). Toluene sulphonamide formaldehyde resin (TSFR) is the main allergen responsible. Interestingly, Fisher reported nail polish to be a potent sensitizer as a liquid but not when solidified, making it usable even by sensitized individuals, provided they take care to apply it in such a way that none of the liquid comes in contact with skin.10 Contact dermatitis is less common once the resin is dry. However, reaction to water-soluble components of TFSR in dry polish has been documented.11,12
Dermatitis may be:
- At the site of application.
- Ectopic reaction—when the hand transfers a small amount of nail cosmetics to other areas (eyelids, face, and neck) (Figure 21.7).
Few manufacturers like Almay (Almay, New York, NY) and Clinique (Clinique Laboratories, New York, NY) have introduced hypoallergenic nail varnishes that do not contain resins.13 Few attempts were made where an alkyl polyester resin was substituted for toluene sulfonamide formaldehyde resin. However, these products wear poorly, often resulting in chipping and peeling.7

Patch test: Nail polish can be patch tested open or closed. To avoid irritation from volatile solvents, the enamel should be dried thoroughly before covering a closed patch test. A 10% concentration of toluene sulfonamide formaldehyde resin in petrolatum should be used for patch testing.
- Distal end of the nail may develop yellow or red discoloration, due to keratin staining, after 7 days of continuous wearing of pigmented nail polish (Figure 21.8). However, this discoloration is harmless and it disappears in 14 days after the nail polish has been removed and can be avoided by the application of a basecoat. Samman has reproduced this phenomenon with the dyes D&C Red Nos 6,7, and 34 and FD & C Yellow No. 5 Lake.14
- Enamels can be photosensitizers when they contain fluorescents like eosin, erythrosin, fluorescein, or rhodomine B7.
- Black, blue, and green nail polishes have been shown to lower pulse oximeter readings of oxygen saturation significantly.15 This should alert emergency physicians.
- Nail keratin granulations presenting as superficial, fine, and scaly white spots have been documented in women who are used to applying fresh nail polish on top of the old one, without using the nail polish remover (Figure 21.9). This can be avoided by following a 5-7 days nail care schedule including 2 days with the nails free of cosmetic agents.16
- Chipped fingernail polish worn longer than 4 days can increase retention of bacteria.17 Thus, nail enamel can be a source of infection.
Variants of Manicure
Nail Buffing
It is used as an alternative to nail enamel. Useful in women who already have beautiful nails and to enhance the esthetic appearance. It needs more time and motivation to buff the nails daily.
Composition
Buffing powder contains—stanning oxide, talc, silica, chalk, or kaolin.18

Figure 21.8: Yellowish red discoloration and fragility of the nail plate after continuous wearing of nail polish

Mode of Application
Buffing powder, paste, or cream is applied to nail, and a chamois–covered buffer is used to polish the nails till the shine is achieved (Figure 21.10).
Adverse Effects
Impatient and rough handling causes injury to the nail matrix and grooving of the nail.19
French Manicure
It is a variant that imitates the natural appearance of the nail. The nail plate is painted with a pink or beige color, then a thin strip of white is applied to the tip to simulate the free edge of the nail.

Press-on Nail Polish
Press-on nail polish is a plastic film available in various colors and designs. They can be fixed to the nail plate with its self-adherent property. It is quick and easy to use giving appearance similar to regular nail polish and it does not need a nail polish remover. Unfortunately the wear is poor.
Appliques
Appliques are available in variety of forms like decals, which are pre-glued and hence, can be affixed to the nail plate directly (Figure 21.11). They may be painted on with acrylic–based paint and the designs are often elaborate.
Nail Jewelry
Nail jewelry ranges from inexpensive costume accouterments to precious metals and gems. They are attached to nail plate either by glues or mechanically by inserting a post through a hole drilled in the distal nail plate just like how ear ring on a post is fastened to the pierced earlobe (Figure 21.12).2
Nail Printers
It is an innovative recently introduced grooming technique where nails are printed with various attractive fascinating designs. Hand is placed inside the printer and all the nails are printed instantly with desired designs.

Figure 21.11A and B: Various appliques available commercially; C and D Finger and toe nails groomed with appliques

Nail Enamel Removers
Enamel removers are liquid material designed to remove nail enamel safely. Chipping off the old nail enamel with another fingernail should be strongly discouraged as this habit can damage the nail plate.
Composition
They are made of organic solvents such as acetone, ethyl acetate, butyl acetate, and MEK (methyl ethyl ketone). However, acetone is discouraged today because of its property of dehydration which can result in brittle nails. Conditioning nail enamel removers are available, containing fatty materials such as cetyl alcohol, cetylpalmitate, lanolin, castor oil or other synthetic oils. These substances act as occlusive nail moisturizers retarding water evaporation.20
Adverse Effects
Nail dehydration is a known side effect and hence, should be used only weekly. If it comes in contact with skin, it may cause irritation of paronychial folds.7
Patch test: If ingredients are to be patch tested, the recommended concentrations are 10% acetone in olive oil; 10% ethyl acetate in petrolatum; 25% butyl acetate in olive oil; and plain MEK.10,21
Cuticle Removers
Interestingly, the cuticle is one of the stickiest tissues on the entire body which obliterates the space between proximal nail fold and nail plate thus protecting the underlying nail matrix. Under no circumstances should the cuticle be removed or traumatized. Unfortunately, the cuticle is not liked by most manicure artists because it complicates the even application of nail polish. Cuticle removers are substances which dissolve keratin by breaking the disulfide bonds of cysteine and soften the cuticle to its allow easier removal.2
Composition: Available inliquid or cream base, they are made of alkaline materials such as sodium hydroxide and potassium hydroxide in a concentration of 2–5%; and humectants like glycerine and propylene glycol to decrease evaporation, irritation and increase viscosity. 264Milder preparations, which are less effective contain the inorganic salts trisodium phosphate or tetrasodium pyrophosphate andorganic bases such as triethanolamine.
Method of Application
Cuticle removers are applied to the base of the nail for 15–20 minutes. Once the cuticle has become soft, it is pushed back off the nail plate by gently rubbing with orange wood stick (Figure 21.13). Professional manicurists may use cuticle knife to lift the cuticle from the nail plate and a V-shaped sharp trimmer or nippers to cut the cuticle.
Adverse Effects
Most common adverse effect is damage to proximal nail fold. Other risks include fungal or bacterial paronychia, irritant contact dermatitis if left for long period and leukonychiastriata.
Proper councelling of patients about the importance of cuticle and avoiding cuticle removers is strongly recommended. However, if the patient demands for cuticle removers, gentle care in handling cuticle must be emphasized.
Patch test: These ingredients are irritants and hence, patch testing is not indicated. If performed, however, the ingredients may be used in the concentration of 5% potassium hydroxide in water; 1–2% propylene glycol in water; 2% trisodium phosphate in water; and 2% triethanolamine in petrolatum.10,21
Cuticle Creams
Cuticle creams unlike cuticle removers are emollients to which quaternary ammonium compounds or urea are sometimes added to promote softening of the cuticle.18 These are used in between the manicures to maintain a soft, supple cuticle. It is applied on proximal part of nail plate as well as on the proximal and lateral nail fold as frequently as necessary.

Hardeners
Hardeners are essentially a modification of nail polish with different solvent and resin concentrations and with the addition of various other substances. They coat fragile or soft nail plates to provide strength.
Composition
Originally, the active ingredient of hardeners was 10% formaldehyde which was discouraged due to its adverse effects. However, US Food and Drug Administration has now permitted low concentration of free formaldehyde (1–2%).2 Currently, keratin, calcium fluoride, natural oils, nylon fibers, teflon, and silk have been added to make it formaldehyde free.4
Mode of Application
They are applied with brush. Hardeners with 1–2% formaldehyde should be applied only to the free edge of the nail while the adjacent skin is shielded. Hardeners should be periodically removed with a nail polish remover.
Adverse Effects
- They may parodoxically cause brittle nails. Products with relatively high (– 5%) formaldehyde concentration can cause reversible subungual hemorrhage, bluish discoloration of the nail plate, onycholysis, subungual hyperkeratosis, dryness and scaling of the skin with intense throbbing pain.8,22 Some patients may remain symptomatic for many years even after discontinuation of high formaldehyde products.
- Pterygiuminversum unguis, painful thickening of the hyponychium which is usually associated with scleroderma; and peripheral vascular insufficiency have been reported to follow the inappropriate use of a nail hardener.16
- Dyschromia in the form yellow, red-blue, and brown, has also been associated with use of hardeners (Figure 21.14).
- Lamellar onychoschizia and transverse leukonychia are other rare side-effects.

Nail Conditioners
Nail conditioners or moisturizers are oil-in-water emulsions designed to treat dry and brittle nails. They help counteract the drying effects of repeatedly immersing the hands in water and detergents.
Composition
They contain the hydrophobic emulsions, proteins, mineral oils, fatty acid esters, triglycerides, and microcrystalline waxes; occlusives, such as lanolin or petrolatum; and humectants, such as glycerin and propylene glycol. A–Hydroxy acids and urea may also be added to increase the water binding capacity of the nail plate.4,7 Few products also contain vitamins and collagen. Newer products are made of organic silicon combined with a thiol derivative. These constitute a mercapto-silanol compound that promotes nail growth and strength. It encourages the formation of keratin and the proliferation of peptide bridges between the keratin chains.
Mode of Application
They are applied with a brush or rubbed on. Recently, applicators in the form of highlighter pens are available. They work better if applied under occlusion with a light cotton glove, preferably at bed time for atleast 3 months.
Elongators
Elongators are preformed plastic nails glued with an acrylic-based cement to the natural nail plate to lengthen short nails or cover the entire nail plate (Figure 21.15). These artificial nails may be prepolished, or decorated with designs. The glue used is ethyl cyanoacrylate.
Mode of Application
- Nails should be prepared by washing and buffing.
- Antiseptic dehydrator is applied with a cotton tip of orangewood stick.
- Size of the artificial nail should be appropriately selected such that tips do not tend to pop off because of mechanical pressure.
- Adhesive (cyanoacrylate glue) is applied to the prepared nail plate.267
- Selected plastic tip is then pressed on nail for 5-10 seconds. Artificial nails should be carefully glued to the affected nails so that glue should not come in contact with adjacent skin.
- Nails can be shaped to achieve desired finish.

They are too occlusive to use for long periods and hence, should be frequently changed.
Adverse Effects
- Shelley and Shelley have reported a case of dystrophic changes in the nail secondary to cyanoacrylate sensitivity.24
Sculptured Nails
Sculptured nails are artificial nails formed by molding the resins on the natural deformed nail plate which results in attractive nails. They are formed to fit and are not preformed. They have become increasingly popular in recent years.
Composition
Nail is sculptured using both polymers and monomers. Polymers include polymethylmethacrylate and benzoyl peroxide available in powdered form, whereas monomers include ethyl or isobutyl methacrylate available in liquid form.4,18 Benzoyl peroxide acts as an accelerator. The liquid may also contain a stabilizers, such as hydroquinone, resorcinol, eugenol, thymol, or N,N-dimethyl-p-toulidine; plasticizers, such as tricresyl or phthalate phosphate; solvents; and dyes.
Mode of Application
- Initial preparations are same as for elongators.
- Template of nail shape, disposable or metallic shield is positioned on the planned digit taking care to align the template in the natural arch of the nail.
- Primer is applied.
- A small brush is dipped into liquid monomer and then into the powder polymer and the brush is rotated so that a ball of mixed material is picked up.
- This wet material in the brush is then applied on the tip of the nail over the template (Figure 21.16). This process is repeated over the other parts of the nail and the material is then spread to the cuticle.
- The material is then allowed to harden and polymerize.
- Smoothening and shaping the sculptured nail is done using file and polish can then be applied as desired. An acrylic nail can thus be molded producing a long, smooth, and attractive nail.
- As the nail grows out, the gap between the proximal nail fold and the acrylic nail must be filled with more acrylic material to maintain the original appearance.6 This is necessary once in 2 weeks.268
- Patients who wear sculptured nails must use acetone-free nail polish removers to remove polish. Failure to do so may result in removal of the nail sculpture from the natural nail.26

Modified Sculptured Nails
Gel nails: These are the modified sculptured nails which require ultraviolet radiation for polymerization and hardening. The gel is a mixture of ethyl cyanoacrylate and polymethyl methacrylate monomers, and is combined with the same powder polymer used for the regular acrylic nail.4 Colored gels nails are available for women who do not change polish color very often.
Adverse Effects
- Monomers have potent sensitizing property compared to polymers. Contact dermatitis may occur in distant site.27 Patch test can be done using 1-5% of the monomer in petrolatum or olive oil. Controls may be required if the patient reacts to 5% but not to 1% of the monomer.
- Susceptibility to onychomycosis and paronychia is increased with sculptured nails due to prolonged occlusion.
- Natural nail may grow out thin and brittle after application of the acrylic nail.
- Microorganism colonization is greater on artificial nails than on natural nails. Moreover, artificial nails have also been linked to poor hand washing practices and more tears in gloves. These can result in increased risk of transmitting bacteria to patients by health care workers.30 Hence, it should be avoided by health care workers.
- Two cases of severe toxic reactions to cyanide were reported as following accidental pediatric ingestion of a product intended for removal of sculptured nails.31269
Nail Wrapping
Nail wrapping is the procedurewhere layers of fibrous substances made of tissue paper, cottonwool, silk, linen, plastic film or fiber glass is applied to the distal edge of the nail plate to either repair and strengthen the free edge (Figure 21.17) or to elongate the nail plate.2
Mode of Application
- Initial preparations are same as for elongators. Nails should be long enough to have a distinct free edge in order to be wrapped.
- Small trimmed piece of paper is glued and wrapped over the free edge of the nail so that it should cover only a small portion of the attached nail.
- Nail shaping and desired finishing can be done.
- Clear nail polish followed by desired colored enamel may then be applied.
- The procedure must be repeated every 2 weeks after removing the previous wrapping with nail polish remover.
Adverse Effect
Nail enamel or acrylic used to glue wrapping may cause allergic contact dermatitis or may cause eye irritation.
Cosmetic Therapy in Nail Disorders
Nail cosmetics can be a promising tool in treating many nail disorders. However, abnormal nail itself is often more susceptible to the adverse effects of cosmetics. Dermatologist should be able to diagnose the disorder appropriately before considering the cosmetic options. Nail scrapings, cultures and biopsy samples should be obtained, especially in the case of presumed bacterial or fungal infection, or in case of pigmented bands, which may represent malignant melanoma. If use of cosmetic products is not contraindicated, they can be used effectively to treat or camouflage diseased and misshapen nails.

Certainly, priority should be to treat the underlying condition. Few commonly encountered nail disorders and their cosmetic uses are discussed below and are summarized in Table 21.2.
|
Onychogryphosis
It is an acquired disorder in which the affected nail becomes thickened, curved and long. It may be secondary to trauma.
Cosmetic treatment: Palliative treatment include paring, trimming and thinning the nail with a clipper, file or a mechanical burr. Nail conditioners are useful. This method although somewhat unsatisfactory, is recommended in the elderly because of poor vascularity of their lower extremities. However, complete avulsion either surgically or using CO2 laser, occasionally followed by matricectomy is the preferred option in adults.
Koilonychia
It may be associated with avitaminosis, iron-deficiency anemia, hemochromatosis, or trauma.
Cosmetic Treatment
Concave depression can be filled with acrylicforms orplastic nails may be applied.
Nail Dyschromia
Nail dyschromia may be due to use of several systemic and topical agents, cosmetic preparations, or idiopathic. Antibiotics, chemotherapeutic agents, and antimalarials may cause toxicity to the matrix, nailbed, hyponychial region, or periungual structures resulting in dyschromia. Splinter hemorrhages often associated with psoriasis or trauma may actually herald subacute bacterial endocarditis; and the hyperpigmented lesion of a malignant melanoma may be confused with subungual hematoma. Hence, dermatologist must always diagnose the nail disorder after obtain accurate history.
Cosmetic treatment: Nail enamels can be used on a limited basis in such patients as nail plate takes around 6 months to grow out. Men can use slightly tinted enamels or basecoats to avoid embarrassment.273
Beau's Lines/Onychomadesis
Beau's lines are transverse grooves in the nail plate whereasonychomadesisis shedding of nails. These are associated with serious systemic illness, idiopathic or traumatic. The thickness of the lines is proportional to the duration of the illness. Therapyintended to treat the underlying disease will allow normal nail plate regeneration with eventual growing out of the affected areas.
Cosmetic Treatment
Buffing the nail plate with pumice–containing buffing cream and applying elongators for the duration of the abnormality can benefit these patients.
Longitudinal Grooves
Longitudinal grooves can be seen on the nail plate which may be caused by aging or trauma, especially to the nail matrix or may be secondary to underlying nail disorders like lichen planus or psoriasis.
Cosmetic Treatment
These grooves may be camouflaged by applying acrylic filler, buffing, and applying enamel. Alternatively, sculptured nails or elongators may be applied. When the groove is trauma induced, it may have its origin in a scar in the matrix, which may be helped by steroid injection or scar excision.
Longitudinal Splitting of the Distal Nail Plate
It occurs due to vigorous filing or trauma, especially in dehydrated nails.
Cosmetic Treatment
Nail conditioners should be applied often. Acrylic fill or nail wrapping is useful in palliative therapy.
Nail Pits
Nail pits are tiny punctate depressions in the nail plate due to parakeratosisin the proximal nail matrix. They have diverse causes like psoriasis, alopecia areata, eczema, pityriasisrosea, secondary syphilis, and trauma.
Cosmetic Treatment
Nail camouflage using several layers of basecoat and nail enamel or by application of nail prostheses can be considered. 274
Rough Nails
Rough nails can occur in psoriasis, alopecia areata, ichthyosis, lichen planus, anddue to exposureto chemicals. The hallmarks of this disorder are a rough, brittle nail surface with gray opacities and frequent splits of the distal edge of the nail plate.
Cosmetic Treatment
Application of conditioners is helpful. Buffing and wrapping offer additional modalities of cosmetic treatment.
Soft Nail
This nails may bend easily or split at the free edge.
Cosmetic Treatment
Nail fortification with hardener or wrapping are beneficial. Application of plastic nails is another cosmetic option to be considered in such patients.
Hard Nail
Hard and thick nail as seen in pachyonychiacongenital, must be soaked in warm water before they can be cut, to prevent irregular chipping. Nail conditioners should be applied for 2–3 months.
Brittle Nails
Brittle nail results due to dehydration if nail plate water content is less than the normal 18%. They can manifest in the formonychorrhexisoronychoschizia.
- Onychorrhexisis excess longitudinal ridging. It has diverse etiologylike iron deficiency anemia and peripheral vascular disease which is due to hypoxia of the matrix; endocrinologiclike hyperthyroidism; metabolic disorders; psoriasis and may be idiopathic.
- Onychoschizia is splitting of the nail plate, usually along a plane that divides the thickness of the nail plate in to the superficial one-third and deep two-thirds, with frequent flaking. The cause of this disorder is most often chronic dehydration and rehydration of the nail plate, which may be experienced by people involved in dishwashing or gardening or by those whose profession requires frequent hand washing. It may also be due to poorly formed manicure. It is also seen in X-linked dominant chondro-dysplasia punctate, polycythemia vera, Darrier's disease, aging, impaired peripheral circulation, HIV infection, glucagonoma and in lichen planus and psoriasis treated with retinoids.
Cosmetic Treatment
- Wearing protective gloves with cotton lining can minimize contact with water and chemicals.
- Mechanical measures that act to reduce trauma to the nail include buffing and filing with an emery board to smooth the free edges, thus reducing the likelihood of inadvertent catching and tearing of the nail plate.32 Trimming and filing should take place after the nails have been well hydrated or after they are polished and let dry.
Hang Nails
Hang nails are common in nail biters but may also result from injury. Hang nails consist of small portions of horny epidermis breaking away from the lateral nail folds (Figure 21.18). The splits become painful when they penetrate to the underlying dermis.
Cosmetic Treatment
Frequent use of cuticle creams can prevent hang nails.
Habit Tic Deformity
It is a nail dystrophy which occurs as a result of self-induced habit when one rubs the central portion of the proximal nail fold of the thumb with the ipsilateral index fingernail consciously or inadvertently. It manifests as central transverse Beau's lines of the thumb nail plate.
Cosmetic Treatment
Spontaneous resolution occurs if the patient stops injuring the nail matrix. Nail sculpture and conditioners are the good cosmetic options till the nail grows normally.

Oral Supplements Supporting Effect of Nail Cosmetics
There is no evidence based-data proving that oral supplements are effective. However, vitamin supplements, oligoelements, and aminoacids could be sometimes useful in certain nail disorders.
Vitamin E— 600-1200 IU daily for 6-18 months may induce a complete clearing of nail changes in yellow nail syndrome. Although the mechanism of action is still unknown, antioxidant properties of A-tocopherol may account for its efficacy.33
Biotin (Vitamin H)—Can be useful in improving nail strength because it may help in the lipid molecule synthesis which produce binding between nail plate keratinocytes. Studies showing clinical improvement in patients who received biotin supplements have been documented.34
Iron—It can be very effective in improving nail fragility. It is recommended when ferritin levels are below 10 ng/mL.4
Cystine—May be useful in promoting proper finger nail growth, hardness, and functionality.4
Measures necessary to ensure safe nail aesthetic service:
- It is necessary to establish national guidelines to nail art salons.
- Nail technicians should be licensed to perform services only on healthy nails and skin.
- Nail salons should seek opinion of qualified dermatologists if a client has visible abnormal skin or nail conditions.
- Nail art technicians should be well-trained on universal precautions to avoid blood borne infections.
Conclusion
Nail cosmetics are useful to disguise and conceal nail imperfections and unsightly dystrophies. Although many of the cosmetic products offer palliative therapy of nail disorders, they may also be a source of significant adverse effects. There is a general lack of proper information and/or advanced training on use of nail cosmetics. It is necessary for dermatologist to get familiarized with these products and their potential risks. Education of manicurists and the public about the safe salon methods is vital in preventing complications.277
References
- Rich P, Daniel CR III. Nail Cosmetics: The benefits and pitfalls. In: Nails diagnosis, therapy, surgery. Ed. Scher RK, Daniel CR III. 3rd edn. Elsevier/Saunders Pennsylvania 2005, p221-27.
- Barnett JM, Scher RK, Taylor SC. Nail Cosmetics. Dermatology clinics 1991; 9(1): 9–17.
- Sekula SA, Havel J, Otillar LJ. Nail salons can be risky business. Arch Dermatol 2002; 138: 414–5.
- Lorizzo M, Piraccini BM, Tosti A. Nail cosmetics in nail disorders. Journal of Cosmetic Dermatology 2007, 6: 53-58.
- Sachdev M, Mogra S. Cosmetic Problems of Nails and their Management. In: Venkataram M (ed). ACS (I) Textbook on Cutaneous & Aesthetic Surgery, 1st Edition. New Delhi: Jaypee; 2012; 744-747.
- Moosavi M, Scher RK. Nail care products. ClinDermatol; 2001: 445-8.
- Scher RK. Cosmetics and ancillary preparations for the care of nails: Composition, chemistry, and adverse reactions. J Am AcadDermatol 1982; 6:523–8.
- Baran R, Dawber RPR (Eds): Diseases of the Nails and Their Management. Boston, Oxford, 1984, 25-79.
- Stern DK, Diamantis S, Smith E, et al. Water content and other aspects of brittle versus normal fingernails. J Am AcadDermatol. Jul 2007; 57 (1):31-6. [Medline].
- Fisher AA: Contact Dermatitis. 3 Ed. Philadelphia : Lea & Febiger; 1986.
- Tosti A, Guerra L, Vincenzi C et al. Contact sensitization caused by toluene sulfonamide – formaldehyde resins in women who use nail cosmetics. Am J Contact Dermatitis 1993; 4:150.
- Hausen BM, Milbrodt M, Koenig WA. The allergens of nail polish: allergenic constituents of common nail polish and toluene sulfonamide formaldehyde resins (TSFR). Contact Dermatitis 1995; 33:157–64.
- Gendler E. Adverse reactions to cosmetics. Cutis 1987; 39: 525–526.
- Samman PD. Nail disorders caused by external influences. J SocCosmetChem 1977; 28: 351.
- Cote CJ, Goldstein EA, Fuchsman WH, et al. The effect of nail polish on pulse oximeter. AnesthAnalg 1988; 67: 683–686.
- Daly BM, Johnson M. Pterygiuminversum unguis due to nail fortifier. Contact Dermatitis 1986; 15: 256-257.
- Baran R. Nail beauty therapy: an attractive enhancement or a potential hazard? J Cosmet Dermatol. 2002; 1: 24-9.
- Patricia G, Engassar, Matsunaga J. Nail cosmetics. In: Scher RK, Daniel CR (Eds). Nails: Therapy, Diagnosis, Surgery. Philadelphia: W B Saunders Company; 1990; 214-223.
- Braun JB. Grooving of nails due to P. Shine: A new manicure kit. Cutis 1977:19; 323.
- Baran R. Nail cosmetics allergies and irritations. Am J ClinDermatol. 2002;3: 547–55.
- Maibach HI, Akerson JM, Marzulli FN, et al: Test concentrations and vehicles for dermatological testing of cosmetic ingredients. Contact Dermatitis 1980; 6: 369.
- De Wit FS, De Groot AC, Weyland JW, et al. An outbreak of contact dermatitis from toluene sulfonamide formaldehyde resin in a nail hardener. Contact Dermatits 1988; 18: 280–283.
- Guin JD, Baas K, Nelson-Adesokan P. Contact sensitization to cyanoacrylate adhesive as a cause of severe onychodystrophy. Int J Dermatol 1998; 37: 21–6.
- Shelley ED, Shelley WB: Nail dystrophy and periungual dermatitis due to cyanoacrylate glue sensitivity. J Am AcadDermatol 19: 574, 1988.
- Scott DA, Scher RK. Exogenous factors affecting the nails: Cosmetics, trauma, and occupational influences. DermatolClin 1985; 3: 409–413.
- Kechijian P. Nail polish removers: are they harmful? Semin Dermatol. 1991; 10:26–8.
- Fisher AA. Adverse nail reactions and paresthesia from “photobondedacrylate ‘sculptured’ nails.” Cutis 1990; 45: 293–4.
- Fisher AA. Permanent loss of fingernails from sensitization and reaction to acrylic in a preparation designed to make artificial nails. J DermatolSurgOncol 1980; 6: 70–71.
- Jeanes A, Green J. Nail art: a review of current infection control issues. J Hosp Infect 2001; 49: 139–42.
- Caravati EM, Litovitz TL. Pediatric cyanide intoxication and death from an acetonitrile-containing cosmetic. JAMA 1988; 260: 3470–3473.
- Kechijian P: Brittle fingernail. DermatolClin 1985; 3:421-429.
- Piraccini M, Iorizzo M, Antonucci A, Tosti A. Treatment of nail disorders. Therapy 2004; 1: 159–67.
- Hochman LG, Scher RK, Meyerson MS. Brittle nails: response to daily biotin supplementation. Cutis 1993; 51: 303–5.