

Embryologically airway starts developing by fifth week of gestational age in the form of lung buds which grow from ventral aspect of primitive foregut. Trachea and esophagus are also separated by fifth week. Hereafter tracheobronchial tree is formed from fifth to fifteenth week. There are 23–25 airway generations from trachea to bronchiole. Bronchus has cartilage in the wall, whereas bronchiole is devoid of cartilage.
Interstitium of lung is divided into axial interstitium, parenchymal interstitial interstitium and peripheral interstitium. Axial interstitium is made of bronchovascular sheaths and lymphatics. Parenchymal interstitium includes interalveolar septum along alveolar walls. Peripheral interstitium includes sub-pleural connective tissue and interlobular septa which encloses the pulmonary veins and lymphatics.
Pulmonary circulation includes primary pulmonary circulation, bronchial circulation and the anastomoses between the two. Primary pulmonary circulation consists of pulmonary arteries and veins that travel down to sub-segmental bronchial level and has a diameter same as that of the accompanying airway. Main pulmonary artery arises from the right ventricle. Bronchial circulation originates from thoracic aorta and supplies through the intercostals arteries which are two in number for each lung.
Mediastinum is the space between the lungs. It is divided into a superior and an inferior compartment. Superior compartment consists of the thoracic inlet. Inferior compartment has anterior, middle and posterior subcompartments. Retrosternal region is included in the anterior compartment, heart lies in the middle compartment and descending aorta with esophagus and paraspinal region is located in the posterior mediastinal compartment. Thymus is located in the anterior part of superior as well as inferior compartment of mediastinum.
The application of chest CT has greatly increased over the years, however, chest radiography remains the most frequently requisitioned and performed imaging examination. A good understanding of normal anatomy and variations is essential for the interpretation of chest radiographs.2



On posteroanterior (PA) view (Figs 1.1 and 1.2), the X-ray beam first enters the patient from the back and then passes through the patient to the film that is placed anterior to the patient‘s chest. It uses 80–120 kV 3and focus film distance of 6 feet. On a PA film, lung is divided radiologically into three zones (Fig. 1.3):

- Upper zone extends from apices to lower border of 2nd rib anteriorly.
- Middle zone extends from the lower border of 2nd rib anteriorly to lower border of 4th rib anteriorly.
- Lower zone extends from the lower border of 4th rib anteriorly to lung bases.
Radiological division does not depict anatomical lobes of the lung.
Anatomically, segmental division of lungs:
Right lung has three lobes:
- Upper lobe which has an apical, anterior and a posterior segment.
- Middle lobe has a lateral and a medial segment.
- Lower lobe has superior segment, medial basal segment, anterior basal segment, lateral basal segment and a posterior basal segment.
Left lung has two lobes:
- Upper lobe which has an apico-posterior, anterior, superior lingular and an inferior lingular segment.
- Lower lobe has superior segment, anterior basal segment, lateral basal segment and a posterior basal segment.
Left lung has no middle lobe.
In a well-centered chest X-ray, medial ends of clavicles are equidistant from vertebral spinous process. Lung fields are of equal transradiance.
Horizontal fissure might be seen on the right side as a thin white line that runs from right hilum to sixth rib laterally. For a fissure to be seen on a radiograph, the X-ray beam has to be tangential to it. The most frequently observed accessory fissure is the azygos lobe fissure which is 4seen in 1% of people. Apices are visualized free of ribs and clavicles on apicogram (Fig. 1.4).

Both hila are concave outwards. The pulmonary arteries, upper lobe veins and bronchi contribute to the making of hilar shadows. The left hilum is slightly higher than right hilum.
The normal length of trachea is 10 cm, it is central in position and bifurcates at T4–T5 vertebral level. Left atrial enlargement increases the tracheal bifurcation angle (normal is 60°). An inhaled foreign body is likely to lodge in the right lung due to the fact that the right main bronchus is shorter, straighter and wider than left main bronchus.
Normal heart shadow is uniformly white with maximum transverse diameter less than half of the maximum transthoracic diameter. Cardiothoracic ratio is estimated from the PA view of chest. It is the ratio between the maximum transverse diameter of the heart and the maximum width of thorax above the costophrenic angles: a = right heart border to midline, b = left heart border to midline, C = maximum thoracic diameter above costophrenic angles from inner borders of ribs. Cardiothoracic ratio = a + b: c. Normal cardiothoracic ratio is 1:2 (Fig. 1.5).
Borders of the mediastinum are sharp and distinct (Figs 1.2, 1.5 to 1.7). The right heart border is formed by superior vena cava superiorly and 5right atrium inferiorly, the left heart border is formed by the aortic knuckle superiorly, left atrial appendage and left ventricle inferiorly.


Right hemi diaphragm is higher than left. Costophrenic angles are acute angles.
To detect any pulmonary pathology, it is important to remember the normal thoracic architecture, both lungs are compared for areas of abnormal opacities, translucency or uneven bronchovascular distribution in the lungs.6

An abnormal opacity should be closely studied to ensure that it is not amalgamated opacity formed by superimposed normal structures such as bones, costal cartilages, vessels, muscules or nipple. Any opacity is evaluated by its extent, margins and location with presence or absence of calcification or cavitation. A general assessment survey is made to look for any other lesion or displacement of adjacent structures.
On CT chest, the sections are made in axial or transverse plane 8 to 10 mm in thicknesses, a miniature topogram should accompany each section or image to show the level of the sections relative to the anatomic structures at that level.
It is important to evaluate CT chest not only in soft-tissue and lung windows settings but also in intermediate windows by playing with window width and window center when considered essential specially when the lesions have intermediate densities.
The evaluation of CT chest should start with the soft tissues of the thoracic wall, the breasts and fat in the axilla (Figs 1.8 to 1.16), followed by assessment of mediastinum in soft-tissue windows. It is good to start with orientation to aortic arch (Fig. 1.10), and moving superiorly looking for any mass or node in region of the major branches of aorta, the brachiocephalic trunk, the left common carotid artery and the subclavian artery (Fig. 1.9). The brachiocephalic veins, superior vena cava, esophagus and trachea are also evaluated to exclude any abnormal mass lesion or deviation from normal.7
8
9









10Moving inferiorly from the aortic arch assessing aortopulmonary window (Figs 1.11 and 1.12), the tracheal bifurcation (Figs 1.8 to 1.16), the hilar and perihilar tissues (Figs 1.12 to 1.14), carefully looking for lymph nodes. The presence of less than 3 small nodes or single node measuring less than 10 mm in diameter in the aortopulmonary window can be considered normal. Heart is examined for any ventricular aneurysm or coronary calcification (Figs 1.14 to 1.16).
The right ventricle lies anteriorly, posterior to the sternum and the right atrium lies on the right lateral side (Figs 1.14 and 1.15). The left ventricle lies on the entire left side (Figs 1.14 to 1.16), the outlet of the left ventricle and the ascending aorta lie in the center of the heart. The left atrium is the most posterior chamber of the heart. The pulmonary veins join the left atrium posteriorly (Fig. 1.14). The inferior vena cava is seen further caudally just at the section the diaphragm appears together with the upper part of liver (Fig. 1.16).
The azygos vein lies dorsal to the trachea adjacent to esophagus; it arches as azygos arch above the right main bronchus and drains anteriorly into the superior vena cava.
Just caudal to aortic arch lies the pulmonary trunk, which divides into the right and left pulmonary arteries, at the level lies the aortopulmonary window. Inferior to the level of aorta the tracheal bifurcation takes place into right and left main bronchus. The aortopulmonary window and subcarinal region have predilection for mediastinal lymph nodes or malignant masses.
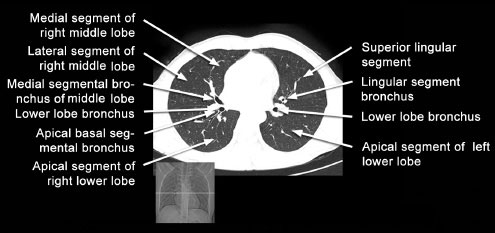
Now the lung parenchyma, ribs and other bony structures are assessed. The pattern of the pulmonary vasculature is scrutinized on the lung windows (Figs 1.17 to 1.28).
11
12
13
14











The lungs show negative density values in the Hounsfield range. The pulmonary vasculature continues from the hilum to the periphery with steady decrease in their thickness with relative oligemia in the periphery and along the margins of the lobes.
Just caudal to aortic arch lies the pulmonary trunk, which divides into the right and left pulmonary arteries, at the level lies the aortopulmonary window. Inferior to the level of aorta, the tracheal bifurcation takes place into right and left main bronchus. The aortopulmonary window and subcarinal region have predilection for mediastinal lymph nodes or malignant masses.
The pattern of the pulmonary vasculature is scrutinized on the lung windows. The lungs show negative density values in the Hounsfield range.