



INTRODUCTION
Occasionally, a biopsy is encountered that looks unremarkable on low power and resembles “normal skin”. In these cases, the possibility of a sampling error could be considered. However, a variety of diseases are associated with minimal histologic findings or requires closer scrutiny to notice abnormalities(Box 1.1). Definitive diagnosis often requires clinical patho-logic correlation. A systematic approach starting with examination of the stratum corneum, epidermis, dermis and then the fat may be useful to elucidate a specific diagnosis.
FINDINGS WITHIN STRATUM CORNEUM
- Tinea versicolor (Figs 1.1A to C)
- Erythrasma (Figs 1.2A to C).
Disorders of Epidermis andStratum Corneum
- Ichthyosis (Figs 1.3A and B)
- Focal acral hypokeratosis (Fig. 1.4)
- Keratoderma (Figs 1.5A and B).
Disorder Involving Epidermal Pigmentation
- Vitiligo (Figs 1.6A to D)
- Idiopathic guttate hypomelanosis: Small faint white macules on lower extremity (Figs 1.7A to C)
- Café au lait macule (Figs 1.8A to C)
- Becker's nevus (Figs 1.9A to C).


Figs 1.1A to C: Tinea versicolor. (A) Low power: normal skin appearance; (B) High power: hyphae within the stratum corneum; (C) Hyperpigmented patches on trunk giving patient multicolored appearance.

Figs 1.2A to C: Erythrasma. (A) Low power with normal skin appearance; (B) High powered H and E shows “debris” within the stratum corneum in erythrasma; (C) Periodic acid-Schiff stain demonstrates filamentous bacteria within the stratum corneum.

Figs 1.3A and B: Ichthyosis. (A) Hyperkeratosis: compare thickness of stratum corneum to epidermis; (B) Stratum corneum appears more compact then in “normal skin” also some areas of follicular plugging.

Fig. 1.4: Circumscribed focal acral hypokeratosis. Abrupt loss of stratum corneum in lesional skin tag.

Figs 1.5A and B: Keratoderma. (A) Orthohyperkeratosis; (B) Notice thickness of stratumcorneum relative to thickness of epidermis.

Figs 1.6A to D: Vitiligo. (A) Normal appearing skin; (B) Closer inspection reveals loss of melanocytes along basal layer of epidermis; (C) Melan-A stain confirms absence of melanocytes; (D) Porcelain white patches.

Figs 1.7A to C: Idiopathic guttate hypomelanosis. (A) Low power; (B) High power (note pigmentation along the basal layers of epidermis on left part of biopsy not right part); (C) Faint hypopigmented macules on lower extremity.
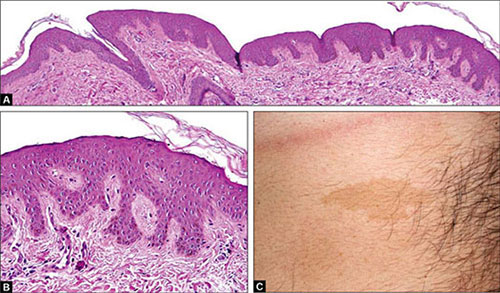
Figs 1.8A to C: Café au lait macule. (A and B) Low and high powered with increased pigmentation along the basal layers of the epidermis (C) Clinical: Brown coffee colored macule.


Figs 1.9A to C: Becker's nevus. (A) Increased pigmentation along the basal layers of anastomosing epidermal rete ridges; (B) Flat bottom rete ridges is clue to diagnosis; (C) Becker's nevus on shoulder picture.Courtesy: Dr Renee Straub
FINDINGS WITHIN THE DERMIS
- Melanophages:
- Postinflammatory pigmentary alteration (Figs 1.10A to C)

- Clue to deposition: Lichen amyloidosis, macular amy-loidosis (Figs 1.11A to D)

- Siderophages: Trauma
- Other pigment deposition:
- Tattoo (Figs 1.12A and B)

- Drug induced pigmentation (Figs 1.13A to C)

- Argyria (Figs 1.14A and B)

- Chrysiasis (Figs 1.15A and B)

- Ochronosis

- Deposition disorders:
- Amyloid (Figs 1.11A to D)

- Mucin: Scleredema (Figs 1.16A and B)

- Mixed inflammatory infiltrate
- Urticaria (Figs 1.17A to D)

- Altered Collagen:
- Connective tissue nevus/collagenoma (Figs 1.18A and B)

- Morphea/scleroderma/atrophoderma (Figs 1.19A to C)

- Injection due to filler (Figs 1.20A and B)

- Altered Elastic Fibers:
- Absence: Disorders of elastolysis

- Cutis laxa (Figs 1.21A and B)
- Mid dermal elastolysis
- Anetoderma (Figs 1.22A to E)
- Increased: Connective tissue nevus/Buchske-Ollendorff syndrome

- Calcified: Pseudoxanthoma elasticum (Figs 1.23A to C).

- Fat cells within the dermis:
- Focal dermal hypoplasia (Figs 1.24A and B)

- Nevus lipomatosus superficialis (lesion usually mami-llated)

- Telangiectatic blood vessels:
- No other finding: Causes for telangiectasias

- Idiopathic, essential, genetic, connective tissue dis-ease
- Mast cells and rare eosinophil present: Telangiectasia macularis eruptiva perstans (Figs 1.25A to C)

- Sweat glands absent: Anhidrotic ectodermal dysplasia.


Figs 1.10A to C: Postinflammatory pigmentary alteration. (A) Melanophages within the dermis along with sparse inflammatory infiltrate. (B) High power note colloid bodies and melanophages; (C) Clinical figure.

Figs 1.11A to D: Lichen amyloid. (A) Low power: expanded papillary dermis; (B) High power: papillary dermis contains eosinophilic globules separated by clefts; (C) Lichen amyloidosis; (D) Lichen amyloidosis with lichenified papules on lower legs.


Figs 1.13A to C: (A) Histology of phenothiazine pigmentation; (B) Yellowish brown dermal pigment; (C) Blue grey hyperpigmentation due to plaquenil.

Figs 1.14A and B: Argyria. (A) Low power; (B) High power-black granules predilection forbasement membrane zone around eccrine glands.

Figs 1.15A and B: Chrysiasis. (A) Medium power pigmentation not readily visible;(B) Higher power, black granules visible in dermis.

Figs 1.16A and B: Scleredema. (A) Low power; (B) Mucin appears as clear spaceswith faint stringy pale blue material between collagen bundles.


Figs 1.17A to D: Urticaria. (A) Low power; (B) High power sparsemixed inflammatory infiltrate; (C and D) Clinical figures.

Figs 1.18A and B: Collagenoma. (A) Low powered; (B) High powered: thickened haphazardlyorganized collagen bundles clue to diagnosis.

Figs 1.19A to C: Scleroderma/morphea. (A) Low powered: skin has a rectangular appearance; (B) High powered: decreased space between collagen bundles along with sclerotic collagen bundles and inflammatory infiltrate concentrated along dermal subcutaneous junction; (C) Clinical figure of linear morphea.

Figs 1.20A and B: Filler material restylane. (A) Low power;(B) High power: basophilic material seen at base of biopsy.

Figs 1.21A and B: Cutis laxa. (A) Low power; (B) Elastic tissue stain low power demonstrates loss of elastic fibers.


Figs 1.22A to E: Anetoderma. (A) Low power; (B) Low power elastic stain; (C) High power elastic stain of involved skin (notice decreased elastic fibers in contrast to 1.22D); (D) Uninvolved skin in patient with anetoderma: high power elastic stain; (E) Papules and nodules which are soft and compressible.

Figs 1.23A to C: Pseudoxanthoma elasticum. (A) Low power; (B) High power: Fragmented calcified elastic fibers; (C) Neck with yellow chicken wire like plaques.

Figs 1.24A and B: (A) Low powered view of Goltz's syndrome. Notice attenuated dermis; (B) High power fat cells within the dermis

Figs 1.25A to C: Telangiectasia macularis eruptiva perstans (A) Lower power; (B) Higher power: telangiectatic blood vessels with surrounding mast cells; (C) Clinical figure.

Disorders Involving Subcutaneous Tissue
- Fat decreased in amount:
- Lipodystrophy

- Fat cells hyalinized: Localized lipodystrophy (Figs 1.26A and B)
- Fat increased in amount in biopsy from scalp; lipedematous alopecia.
BIBLIOGRAPHY
- Farmer ER, Hood AF. Pathology of the Skin, 2nd edition. McGraw-Hill; New York: 2000.
- McKee PH, Calonje E, Granter SR. Pathology of the Skin with Clinical Correlations. Elsevier; Mosby: 2005.
- Weedon D. Weedon's Skin Pathology, 3rd edition. Elsevier; Churchill Livingstone: 2010.