

INTRODUCTION
Facial nerve embryology is discussed in detail by Sataloff and Sataloff.1 This chapter is a brief overview of material presented in that book. This chapter is also modified in part from an article on this topic, with permission.2 In studying the embryology of the facial nerve, it is helpful to keep in mind the final structure toward which development progresses. In the adult, the motor nucleus of the facial nerve (VIIIth cranial nerve) is located deep in the reticular formation of the caudal portion of the pons. The axons leave the motor nucleus and extend dorsally and medially, cranially, and superficially. They bend around the abducens nucleus to form the first genu of the facial nerve. The fibers then course deep through the pons and exit from the central nervous system between the olive and the inferior cerebellar peduncle. At this point, the axons join to form the motor root. The sensory root (nervus intermedius) consists of central processes of neurons located in the geniculate ganglion and axons of parasympathetic neurons from the superior salivatory nucleus. The nervus intermedius enters the central nervous system at the pontocerebellar groove lateral to the motor root and synapses with neurons in the upper part of the solitary tract of the medulla oblongata. The facial nerve and nervus intermedius course with the vestibuloacoustic nerve from the brainstem and enter the internal auditory canal (Fig. 1.1). For approximately 20% of its course, the nervus intermedius is fused with the VIIIth cranial nerve.3
At the point where the facial nerve enters the middle ear, it bends a second time at the geniculate ganglion (the second genu) and courses horizontally through the middle ear. It then curves (the pyramidal bend) to course vertically through the mastoid bone and exits at the stylomastoid foramen (Fig. 1.2). The nerve is ordinarily surrounded by a bony sheath called the fallopian canal. Several branches are given off during the intrapetrosal course. The facial nerve spreads extratemporally to innervate the facial musculature (Figs. 1.3A and B).


Fig. 1.1: The usual relationships of the 7th and 8th cranial nerves as they enter the internal auditory canal and temporal bone.
Medially to laterally, the facial nerve branches include 11 structures of note (Fig. 1.4):
- Communications in the internal auditory canal with the VIIIth cranial nerve
- The greater superficial petrosal nerve, which supplies taste fibers to the palatal mucosa, preganglionic parasympathetic axons to the pterygopalatine ganglion, and postganglionic axons to the lacrimal glands, nasal glands, and palatine mucosal glands; it also communicates with the lesser petrosal nerve3
The figures in this chapter originally appeared as part of Chapters 3 and 4: Embryology and Anomalies of the Facial Nerve by Sataloff RT and Sataloff JB. Philadelphia, Jaypee Medical Inc., 2014.4
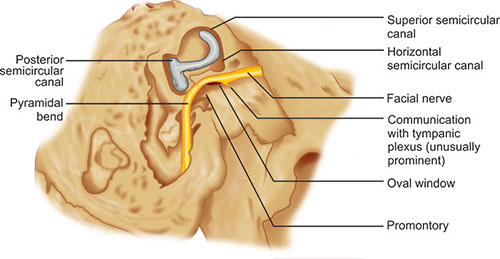
Fig. 1.2: The relationship of the facial nerve in its horizontal and vertical portions to other temporal bone landmarks.

Figs. 1.3A and B: (A) The distribution of the facial nerve to muscles of the face after the nerve has exited from the stylomastoid foramen. The extratemporal anatomy of the facial nerve is variable. (B) Common patterns of branching of the extracranial portion of the facial nerve. Type I is seen in 20% of cases; Type II, in 37.5%; Type III in 20%; Type IV, in 15%; Type V, in 15%; and Type VI, in 2.5%, according to Coker and Fisch. (T: Temporal branch; Z: Zygomatic branch; B: Buccal branch; M: Marginal mandibular branch; C: Cervical branch).

- The nerve to the stapedius muscle
- The chorda tympani nerve, which supplies taste fibers to the anterior two-thirds of the tongue, preganglionic parasympathetic fibers to the submandibular gland, and postganglionic fibers to the submandibular and sublingual glands
- The posterior auricular branch, which innervates the auricularis posterior, the cranially oriented muscles of the auricle, and the occipital muscles-communicates with the greater auricular nerve, the auricular branch of the vagus nerve, and the lesser occipital nerve3
- The branch to the posterior belly of the digastrics muscle
- The branch to the stylohyoid muscle
- The temporal branch that supplies the lateral intrinsic muscle of the auricle, the anterior and superior auricular muscles, the frontalis, the orbicularis oculi, and the corrugator
- The buccal branch, which innervates the procerus, the zygomaticus major and minor, the levator labii superioris, the levator anguli oris, nasal muscles, the buccinator, and the orbicularis oris
- The marginal mandibular branch to the risorius muscle and the muscles of the lower lip and chin
- The cervical branch to the platysma; there are interconnections between the facial nerve and primarily the sensory nerves, including the trigeminal, glossopharyngeal, vagus, and cervical nerves.4
The intracranial portion of the facial nerve is supplied by the anterior inferior cerebellar artery. The intrapetrosal portion is supplied by the superficial petrosal branch of the middle meningeal artery and the stylomastoid branch of the posterior auricular artery. The extracranial portion is supplied by the stylomastoid, posterior auricular, superficial temporal, and transverse facial arteries. The anastomosis between the intratemporal branches usually occurs in the upper one-third of the vertical portion.
EMBRYOLOGY OF THE INTRACRANIAL PORTION OF THE FACIAL NERVE
This discussion includes information on the development of only the extracranial portions of the facial nerve. We encourage the reader to consult other literature for a brief review of the embryology of the intracranial portions,1 and for new information on differentiation and migration of the facial nerve.1 This information is very helpful for the purpose of orientation.
Fertilization through week 4: The facioacoustic primordium appears during the third week of life. It is attached to the metencephalon just rostral to the otic vesicle.6

Fig. 1.5: A 4.2-mm embryo approximately 3-and-a-half weeks old. The region of the epibranchial placode of the second arch is labeled.
It becomes more superficial and rostral as it proceeds ventrally, and it ends adjacent to the deep surface of the epibranchial placode on the dorsal and caudal aspect of the first branchial groove. There are no branches, and the geniculate ganglion is not yet present (Fig. 1.5). During the fourth week, by the time the embryo reaches 4.8 mm in length, the facial nerve splits into two parts. The chorda tympani nerve comes off rostrally, courses ventrally to the first pharyngeal pouch, and enters the mandibular arch. The caudal main trunk terminates in mesenchyme. By the time the embryo reaches 6 mm in length, the nerve approaches the epibranchial placode, and large, dark nuclei mark the development of the geniculate ganglion.5
Weeks 5 and 6: By the time the embryo has reached 7 mm in length, near the beginning of the fifth week, the mesenchymal concentrations that form the cephalic muscles can be seen in association with their nerves (Fig. 1.6).6 The geniculate ganglion and the nervus intermedius also appear, although the latter is not always visible as a separate nerve until approximately the seventh week.5 The geniculate ganglion is lateral and rostral to the VIIIth nerve ganglion. The greater superficial petrosal nerve is present. The chorda tympani is large and enters the mandibular arch; it terminates near a branch of the mandibular nerve, which will become the lingual nerve. By the middle of the fifth week (embryo length: 10 mm), the facial nerve gives off small branches to the posterior digastric premuscle mass. The nerve terminates in mesenchyme.
In the 8-mm embryo, all the cranial nerves except the olfactory and optic nerves are recognizable. All the cranial nerves that carry sensory fibers have prominent ganglia near their points of connection with the brain. These include cranial nerves V, VII, VIII, IX, and X. The primarily efferent cranial nerves (III, IV, VI, and XII) have no external ganglia. In the 8- to 14-mm period, the posterior auricular nerve appears near the chorda tympani. Complete separation of the facial and acoustic nerves is apparent, and a discrete nervus intermedius develops.
By the time the embryo reaches 14 mm in length, the geniculate ganglion and the greater superficial petrosal nerve are well defined, and the epibranchial placode has disappeared. The greater superficial petrosal nerve courses ventrally and rostrally to the lateral aspect of the developing internal carotid artery. Here it joins the deep petrosal nerve and continues as the nerve of the pterygoid canal. It terminates in a group of cells that will become the pterygopalatine ganglion. At 16–17 mm (middle of the sixth week), a branch arises from the ventral aspect of the geniculate ganglion and courses caudally and dorsally to the glossopharyngeal ganglion. The chorda tympani and lingual nerves end near the developing submandibular ganglion. Some facial nerve fibers terminate in the mandibular arch superficially and caudally.
During this period, the superficial layer of the mesenchymal lamina of the second arch spreads to establish four laminae (Fig. 1.7):
- The occipital lamina (the occipitalis, auricularis posterior, and transverse nuchae muscles)
- The cervical lamina (the cervical part of the platysma)
- The mandibular lamina (the depressor labii inferioris, the mentalis, the risorius, the depressor anguli oris, the inferior part of the orbicularis oris, and perhaps the buccinator and the levator anguli oris)
- The temporal lamina, which spreads during the latter part of this stage (the auricularis superior).
When the embryo is between 10 and 18 mm in length, the deep layer of the second mesenchymal lamina differentiates into the posterior digastrics complex (the stapedius muscle, the posterior belly of the digastric muscle, the digastric tendon, and the stylohyoid muscle).
Weeks 7 through 9: By the beginning of the seventh week, the embryo has reached approximately 18 mm in length (Fig. 1.8). The nervus intermedius, which is smaller than the motor root of the facial nerve, passes into the brainstem between the acoustic nerve and the facial nerve motor root. The chorda tympani and lingual nerves unite proximal to the submandibular tympani nerves, and it divides into cranial and caudal branches.7

Fig. 1.6: Diagram of a 4-and-a-half-week-old embryo illustrating the mesenchymal concentrations that will give rise to the cephalic muscles, as well as the cranial nerves associated with them.

Fig. 1.7: A 6-week-old embryo (11 mm) showing further development of the premuscle masses of the cephalic muscles.
The caudal branches communicate with branches of cervical nerves C2 and C3. Several branches are visible in the peripheral portion of the VIIth nerve. The most caudal branches communicate with nerves from the second and third cervical ganglia in a plexus in the second arch. Another portion courses ventrally, terminating deep to the platysma myoblastic lamina. The rest of the branches course to the angle of the mouth, or caudally and superiorly into the mandibular arch. By the time the embryo is 19 mm long, some caudal branches have reached the infraorbital rim.8
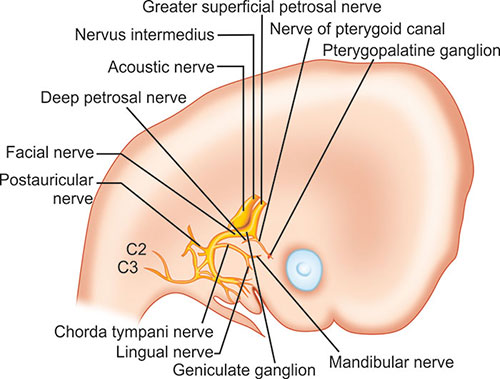
Fig. 1.8: The relationship between the facial nerve and parotid primordium at approximately 7 weeks (18 mm).
All of the peripheral branches lie close to the deep surfaces of the myoblastic laminae that will form the facial muscles. Very few fibers course dorsally. The zygomatic and temporal nerves will arise higher in the facial nerve. At 18 mm, the parotid bud is rostral and unbranched, appearing as an evagination from the lateral oral cavity area.
In the 22-mm embryo (middle of the seventh week), the posterior belly of the digastric muscle and the stapedius and stylohyoid muscles are developing (Fig. 1.9). A branch from the geniculate ganglion near the greater superficial petrosal nerve, which developed earlier, is reduced to a communication as the tympanic plexus and the lesser petrosal nerve develop from the IXth cranial nerve. The interanastomoses of the peripheral branches of the facial nerve are visible as separations of the main trunk. A small nerve branch approaches the buccal region superficial to the parotid bud.
Separations between nerve branches increase considerably in number and size by the end of the seventh week (26 mm). By then, the branch to the stapedius muscle is visible. This branch was probably present earlier, but it can be seen only after the branch separates from the main trunk.5 Peripheral branches course cranially to become the zygomatic and temporal divisions. The buccal, mandibular, and cervical divisions constitute approximately one-half of the peripheral branches. All the peripheral divisions can be identified, but the temporal branches have not yet reached the frontal region. Anastomoses are well established with the infraorbital, buccal, auriculotemporal, and mental branches of the trigeminal nerve. Previously established communications with branches of C2 and C3 have become communications with the greater auricular and transverse cervical nerves. A combined marginal mandibular-cervical branch appears between the time the embryo grows from 20 to 45 mm (seventh through the middle of the eighth week).

Fig. 1.9: By the middle of the 7th week (22 mm), additional branching has occurred. However, the structures of the facial nerve are still anterior with respect to the external auditory meatus, which is in the process of migration from its original location low on the developing embryo.
The superficial layer of the second-arch mesenchyme differentiates into two more laminae:4
- Infraorbital (zygomaticus major and minor, the levator labii superioris alaeque nasi, the superior part of the orbicularis oris, and possibly the compressor naris, the depressor septi nasi, the orbicularis oculi, the frontalis, the corrugator supercilii, and the procerus)
- Occipital platysma.
Between 24 and 26 mm, the zygomaticus major, the depressor anguli oris, and the buccinators appear. Between 27 and 45 mm, the frontalis and zygomaticus minor appear. The branch that connects the VIIth cranial nerve with the lesser petrosal nerve (from cranial nerve IX) apparently carries small myelinated fibers that contain interspersed autonomic fibers from the auricular branch of cranial nerve X. In addition, by 26 mm the embryo develops first-order ductules of the parotid primordium, which lies next to the masseter muscle, and several branches of the facial nerve course superficial to it.7 By 27 mm, second-order ductules appear. At this time, the buccal, marginal mandibular, and cervical nerve branches approach the parotid primordium. By 32 mm (eighth week), third-order ductules are present, and the primordium has entered the parotid space.9
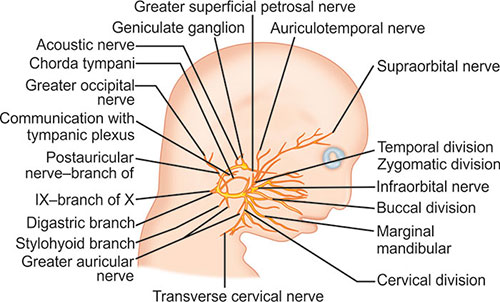
Fig. 1.10: During the 11th week (80 mm), extensive branching including communications with other cranial nerves can be seen. The vertical portion of the facial nerve is still anterior with respect to the external auditory meatus (not shown). The vertical portion and main trunk could be injured easily during surgery if the relationship of the auricle to the facial nerve were assumed to be that of an adult.
In the 37-mm embryo (8.5 weeks), fourth-order parotid ductules are present, and buccal nerve branches are superficial to the main duct. The temporal, zygomatic, and upper buccal branches are superficial on the parotid primordium. The lower buccal, mandibular, and cervical branches are deeper. The postauricular nerve goes to the occipital region, and a branch to the dorsal aspect of the auricle is present. Although there are no branches to the fused eyelids, yet a branch from the temporal division approaches the frontal region.
During the eighth week, a sulcus develops around the facial nerve, blood vessels, and stapedius muscle on the posterior aspect of the cartilaginous otic capsule. The sulcus is the beginning of the fallopian canal. The orbicularis oris, the levator anguli oris, and the orbicularis oculi also appear at approximately 37 mm.4 During the ninth week (50–60 mm), the auricularis anterior, the corrugator supercilii, the occipital and mandibular platysma, and the levator labii superioris appear. Also about the ninth week, the laterohyale fuses to the otic capsule to form part of the anterior wall of the fallopian canal and the pyramidal eminence. The segment of the anterior wall of the fallopian canal distal to the laterohyale is formed by Reichert's cartilage. The cranial nerves move closer to their adult relationships.
Weeks 10 through 15: During the 58- to 80-mm period, extensive branching of the peripheral portions of the facial nerve occurs (Fig. 1.10). Some divisions reach the midline. Extensive communication with branches of the trigeminal nerve occurs in the perioral and infraorbital regions. Communications exist between the nervus intermedius and both the VIIIth nerve and the motor root of the VIIth nerve. Despite extensive branching, the facial nerve begins its vertical course while still in the middle ear, and its relationship to the external and middle ear structures is far more anterior than it is in the adult.
During the 11th week (80 mm), the external petrosal nerve arises from the facial nerve distal to the geniculate ganglion and courses with a branch of the middle meningeal artery. Branches also arise from the facial nerve between the stapedius and the chorda tympani nerves. Together, these branches and branches of cranial nerves IX and X provide sensory innervation to the external auditory canal. Branches to the lateral aspects of the eyelids are present, and communication with the zygomaticotemporal nerve has begun to develop. Previous communications with branches of cervical nerves have now become communications with the lesser occipital and transverse cervical nerves. The horizontal portion of the facial nerve can be distinctly seen adjacent to the developing otic capsule. The nasal muscles arc also differentiated at approximately 80 mm.
The relationship between the facial nerve and the parotid gland is about the same at 12 weeks as it was at 7 weeks. However, by the time the embryo reaches 80 mm in length, complicated connections between the superficial and deep portions of the parotid primordium can be seen.7 At 14 or 15 weeks, the geniculate ganglion is fully developed, and facial nerve relationships to middle ear structures have developed more fully. During this growth period, the facial nerve has remained in association with the mesenchyme, which differentiates into the labyrinth and the mastoid.
Week 16 through birth: Between 16 and 20 weeks, the facial nerve, arterioles, venules, and the stapedius muscle lie in a sulcus on the canalicular wall. The mesenchyme in which they are surrounded is differentiating into connective tissue. Although the middle ear continues to enlarge, the facial nerve remains more superficial and anterior in relation to the auricle than it is in the adult. All definitive communications of the facial nerve are established by the 16th week (146 mm).
By 26 weeks, ossification has progressed, and growth of the outer layer of periosteal bone has resulted in a partial closure of the sulcus, forming the fallopian 10canal. The deep surface is completed first. By 35 weeks, a bony ridge has formed that separates the geniculate ganglion from the epitympanic rim. Late in fetal life, the facial canal in most cases is closed by bone except in the anterior cranial portion, where it remains open to form the facial hiatus along the floor of the middle cranial fossa. However, at least 25% of fallopian canals have this dehiscence; the most common site is adjacent to the oval window.8 The length of the dehiscence ranges from 0.5 mm to the length of the entire horizontal portion, but they are usually no larger than about 2 × 3 mm. This most common area of dehiscence is probably secondary to the failure of ossification after the stapedial artery (which passes through this area) resorbs prior to birth. The incidence of dehiscence has been reported to be as high as 55%.9
By the time of birth, the facial nerve has developed into a complex but generally consistent structure. In an interesting study of the mandibular ramus in stillborns by Sammarco et al.,10 the authors found that in 17 of 24 facial halves, some or all of the mandibular branches of the cervical facial ramus were below the angle of the mandible. Moreover, 19 of the 24 specimens had 2 or 3 mandibular branches. All mandibular branches were above the mandibular margin as they crossed the facial artery. In 16 specimens, all branches passed over the facial artery; in the other 8, they straddled the facial artery. At birth, the anatomy of the facial nerve approximates that of the adult with the exception of the nerve's exit through the superficially Iocated stylomastoid foramen. Adult anatomy occurs in this region as the mastoid tip develops postnatally.
CLINICAL APPLICATIONS
In patients with congenital malformations, it is usually possible to determine the fetal age at which developmental arrest occurred. This information allows the surgeon to predict the anatomy of the deformed ear and facial nerve on the basis of their usual embryologic development at the time when the arrest occurred. Moreover, if anomalies are also present in other organ systems (e.g., the kidney), they often reflect interference with development at the same time in fetal life. Hence, when a congenital anomaly of any portion of the ear can be observed visually, radiologically, or surgically, and if the clinician recognizes the fetal age at which normal development ceased in that portion, the physician should be able to predict the position of the facial nerve. If the facial nerve is anomalous, its development is most likely to have been interrupted at the same time that the development of the ear was interrupted, particularly in the case of a middle ear malformation.

Figs. 1.11A and B: (A) Appearance of the auricle prior to otoplasty. (B) CT scan revealing absence of the external auditory canal (open arrow), an atresia plate (AP) at the level where the tympanic membrane should be, and the ossicular mass (O). The dehiscent horizontal portion of the facial nerve (curved white arrow) is seen coursing above the oval window (OW) and entering the fallopian canal (FC) at the pyramidal bend.
To test the validity of such predictions, surgical observations were made of 13 ears in 11 patients with congenital malformations.1,11 We describe one of these cases to illustrate the clinical application of information about facial nerve embryology. The patient was a 6-year-old boy who had been followed by the author since the age of 3 months. His auricle was malformed, and only portions of the helix, lobule, and tragus were recognizable. Computed tomography (CT) revealed the absence of the external auditory canal and the presence of a small middle ear space with an ossicular mass (Figs. 1.11A and B).
The appearance of the auricle placed the time that the defect occurred at approximately the eighth week, and the relationship of the nerve to middle ear structures had been fairly well established. However, because the middle ear was small and not fully formed, it and the vertical portion of the facial nerve appeared to the surgeon to be anteriorly and inferiorly displaced. Moreover, the vertical portion of the nerve coursed more superficially than it does in the normal adult. The nerve coursed through the region where the surgeon planned to construct the new ear canal.
After creating an ear canal and removing the atresia plate, the surgeon identified the moderately malformed ossicles. The malleus and incus were fused, but an incudomallear joint was seen. The stapes was fully developed but immobile, although it was easily manipulated. The horizontal portion of the facial nerve was in a normal position relative to the stapes, but dehiscent. As predicted, the facial nerve and middle ear were more anterior than is the case in a fully developed ear, and the facial nerve coursed anteriorly and laterally more abruptly distal to the pyramidal bend.
If adult relationships are used to gauge the position of the middle ear with respect to the position of the external meatus, the surgeon would enter the middle ear and mastoid region posterior to the vertical portion of the facial nerve and hypoplastic middle ear. Exploration from the point of entry forward would put the facial nerve at risk of injury, especially in light of its abruptly superficial course from the pyramidal bend to the stylomastoid foramen. However, with an understanding of the embryology of the facial nerve, its location can be predicted easily and accurately.
REFERENCES
- Sataloff RT, Sataloff JB. Embryology and anomalies of the facial nerve, 2nd edn. Jaypee Brothers Medical Publishers; New Delhi, India: 2013.
- Sataloff RT, Selber JC. Phylogeny and embryology of the facial nerve and related structures. Part II: Embryology. Ear Nose Throat J. 2003;82:764–79.
- Rhoton AL, Jr, Kobayashi S, Hollinshead WH. Nervus intermedius. J Neurosurg. 1968;29(6):609–18.
- Vidic B. The anatomy and development of the facial nerve. Ear Nose Throat J. 1978;57:236–42.
- Gasser RF. The development of the facial nerve in man. Ann Otol Rhinol Laryngol. 1967;76:37–56.
- Patten BM. Human embryology. Blakiston; Philadelphia, PA: 1946. pp. 112–13, 306–14, 371–5, 435.
- Gasser RF. The early development of the parotid gland around the facial nerve and its branches in man. Anat Rec. 1970;167:63–77.
- Beddard D, Saunders WH. Congenital defects in the fallopian canal. Laryngoscope. 1962;72:112–15.
- Baxter A. Dehiscence of the Fallopian canal. An anatomical study. J Laryngol Otol. 1971;85:587–94.
- Sammarco GJ, Ryan RF, Longenecker CG. Anatomy of the facial nerve in fetuses and stillborn infants. Plast Reconstr Surg. 1966;37:566–74.
- Sataloff RT. Embryology of the facial nerve and its clinical applications. Laryngoscope. 1990;100:969–84.