

STRUCTURE OF SKIN
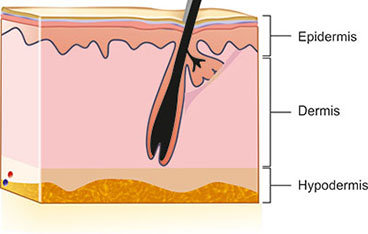
Skin is the largest organ of the body. It is a very complex structure composed of three layers viz., epidermis, dermis and subcutaneous tissue (Fig. 1.1). It is also composed of various appendages. The outermost layer or the epidermis is further composed of four layers, e.g. stratum corneum, stratum granulosum, stratum spinosum and stratum basale. There are melanocytes situated at the basal cell layer and Langerhans cells throughout the epidermis.
The dermis is predominantly composed of collagen and fibroblasts. There are elastic fibers also. Various structures situated in the dermis are composite structure of hair follicle with sebaceous gland known as pilosebaceous apparatus, eccrine or sweat glands. Beneath the dermis there is a layer of fat known as subcutaneous tissue. In the dermis there are dermal capillaries and venules which comprise dermal vasculature. There are also lymphatics situated in the dermis.

FUNCTIONS OF SKIN
The outermost layer or stratum corneum performs the barrier function and maintains the hydration of skin. It also prevents the penetration of irritants, toxins and organisms through the epidermis into the dermal capillaries from the environment. The rest of the epidermis act as protective layer. Melanocytes of the epidermis confers color of the skin by transferring melanin to the basal keratinocytes. It also protects the skin from deleterious effect of ultraviolet light. Langerhans cells present antigen to the immunological unit of the skin. Hence, it is considered as the first line of immunologic defence.
The collagen, elastic fibers act as a tough, leathery, mechanical barrier against cuts, bites, abrasions, bruises. Its collagenous matrix provides structural support for various cutaneous appendages. Hair grows from follicles placed in the deep dermis and imparts beauty to the individual. It also protects the scalp from the sunlight and various environmental allergens. Sebaceous glands produce oily secrertions and lubricate the skin and contribute to the protective function of epidermal barrier. Eccrine glands produce sweat and secrete on the skin surface through eccrine ducts. Thus it acts as an important organ responsible for thermoregulation. Cutaneous capillaries, venules and lymphatics act as perfusion unit of skin. The skin also contains specialized receptors for heat, pain, touch and pressure. Sensory inputs from these structures help to protect the skin surface against environmental trauma and noxious agents. The subcutaneous fat acts as a protective cushion for the skin and stores energy and provides insulation to the body. To summarize, various functions of the skin are as follows:
- Protection: It protects the body from physical, chemical and biological injuries.
- Perception: It perceives various sensations like pain, touch, temperature and vibration.
“A vision without the ability to execute is probably a hallucination.”—Stephen M Ease
- Temperature regulation: Eccrine sweat glands and dermal vasculature play important role of thermoregulation.
- Barrier function: Skin acts as a permeability barrier that regulates the diffusion of substances particularly water and electrolytes, etc.
- Secretory functions: Synthesis of vitamin D3 is an important secretory function with the help of sunlight.
- Storage functions: The dermis and subcutaneous fat act as a storage center for energy and other compounds.
- Excretory functions: Some of the harmful substances are excreted through the skin.
- Immunological function: Recognition of antigens and elicitation of immunological response is done by skin.
- Cosmetic function: Color and texture of skin along with the hair and nail play an important role in esthetic appeal of an individual.
SKIN TYPES AND SKIN COLOR
Skin color is of two types, constitutive skin color and facultative skin color.
Constitutive skin color is the basic skin color of an individual and is genetically determined. Facultative skin color is the skin color that results from ultraviolet ray (UVR) exposure. It is basically tanning of the skin. Depending on the response of the skin to UVR, various skin phototypes (SPT) have been described and different races with different SPTs possesses different types of skin color. Table 1.1 highlights color of skin and response to UVR in different skin phototypes.
Three types of melanin in humans have been demonstrated, eumelanin (brown-black melanin), pheomelanin (yellow-red melanin) and neuromelanin (black). While in most of the melanocytes there is a minimal admixture of pheomelanin and eumelanin, in red hairs exclusively pheomelanin is present. Neuromelanin is present in nerve cells. Neuromelanin is formed by an enzymatic pathway different from that of eumelanin or pheomelanin synthesis. Hence in oculocutaneous albinism (OCA) there is presence of pigment in substantia nigra.
BASIC MORPHOLOGY OF SKIN LESIONS
Various morphology of the lesions have been divided into 3 types, primary lesions, secondary lesions and special lesions.
PRIMARY LESIONS
Different types of primary lesions are:
- Macule: It is only the change of color of skin, texture remaining unaltered. A macule can be hyperpigmented, hypopigmented or erythematous.
- Papule: It is a circumscribed solid lesion measuring less than 1 cm in diameter. A papule can be erythematous, skin-colored or of any other color. The surface may be flat, verrucous or umbilicated.
- Plaque: It is a solid elevation more than 1 cm in diameter. There may be associated follicular plugging, telangiectasia, atrophy, etc.
- Nodule: It is a deep-seated solid three-dimensional lesion which may be hard, firm, soft, fleshy, tender or non-tender, fixed or mobile. The surface of the nodule can be smooth, keratotic, ulcerated or fungating.
- Pustule: It is a circumscribed elevated lesion containing free pus. Sometimes it may be sterile.
- Vesicle and bulla: A vesicle is a circumscribed raised lesion containing free fluid and less than 1 cm in diameter. A vesicle is circumscribed raised lesion containing free fluid, less than 1 cm diameter. Vesicles may be tense or flaccid and on rupture leave behind raw area.
- Wheal: It is a transient or evanescent elevated plaque-like lesions with erythema, edema and central pallor.
- Cyst: It is a sac that contains liquid or semisolid material.
- Abscess: It is a collection of pus either in the dermis or subcutaneous plane or both.
SECONDARY LESIONS
Secondary lesions are lesions which are basically modified primary lesions by scratching, rubbing or secondary bacterial infections. Various secondary lesions are:
- Scales are formed as a result of increased or abnormal keratinisation. They may be fine powder-like or large silvery white or even fish like.
- Crust is a collection of dried exudates, dead tissue and microorganisms. Crust may be brown/brownish-yellow, may be adherent or friable.
- Excoriation or scratch marks are predominantly seen in pruritic disorders.
- Erosion is a superficial ulceration covered with serous exudates and heals without scarring.
“A journey of a thousand miles begins with a single step.”—Confucius
- Ulcer is the result of breach in the continuity of skin with loss of epidermis and a part of dermis. Ulcer always heals with scarring.
- Lichenification is thickening, increased criss-cross markings and mild hyperpigmentation. It is the end result of chronic eczema.
- Atrophy: It is thinning of skin which appears shiny wrinkled with prominent blood vessels underneath.
SPECIAL LESIONS
Some of the lesions are pathognomonic of certain diseases as follows:
- Burrow Tunnel-like serpiginous lesions seen in the superficial part of the skin.
- Comedones are the result of plugging of the pilosebaceous duct by internal secretion. Comedones may be open (black) or closed (white).
- Milia are the small superficial cysts 1–2 mm in diameter commonly seen on the face.
- Telangiectasia means distinctly visible superficial blood vessels as a result atrophy of skin.
CONFIGURATION OF THE SKIN LESIONS
Characteristic configuration of lesions may suggest a diagnosis. Some classical are:
- Linear: Lesions are present in a line.Examples: Epidermal nevi, lichen striatus, warts, psoriasis, incontinentia, etc.
- Dermatomal: Lesions are present in a dermatome.Examples: Herpes zoster, vitiligo, nevus depigmentosus, port-wine stain.
- Serpiginous: Lesions follow a serpiginous track.Examples: Cutaneous larva migrans, elastosis perforans serpiginosa.
- AnnularExamples: Tinea, granuloma annulare, erythema annulare centrifugum, erythema marginatum.
- Herpetiform: Grouped lesions or clustered lesions.Examples: Herpes simplex infection, herpes zoster, dermatitis herpetiformis.
- Reticulated: Means ripple-like.Examples: Cutis marmorata, livedo reticularis, erythema ab igne.Filiform: Means thread-like.Examples: Filiform warts, dermatosis papulosa nigra, skin tags/acrochordons.
- GeographicExamples: Geographic tongue, psoriasis, erythema annulare centrifugum.
NEONATAL DERMATOSES AND CARE OF NEWBORN SKIN
This presents as macular blue-gray pigmentation at birth on the sacral area in normal infants of darker-skinned races.


“It is better to be in chains with friends, than to be in a garden with strangers.”—Persian Proverb


The patches are usually rounded or oval in shape, up to 10 cm in diameter and usually single. Other than the lumbosacral region, the buttocks, flanks or even shoulders may be affected in extensive lesions. The pigmentation develops in fetal life, increases in depth for a period after birth and then diminishes. It usually disappears in the first decade.
Natural History
It is considered as one of the physiological skin changes of the newborn. When Mongolian spots are associated with bilateral nevus of Ota, they take much longer time to disappear spontaneously.
Management
Explanation of the condition and its natural history to the parents helps to reassure them.
The sebaceous glands of neonates produce a considerable amount of sebum in first few weeks of life influenced by maternal androgen. Neonatal acne mostly affects male infants and face is affected almost exclusively.


“Give a man fish and feed him for a day; teach him to use the net and he won't bother you for weeks.”—Chinese proverb


Management
Lesions present as comedones and inflammatory papulas over cheeks. The lesions tend to subside by 2–3 weeks and require no treatment.
NEONATAL MILIA (Fig. 1.6)
Milia are one of the most common transient findings in the cutaneous survey in neonates. These consist of 2–3 mm white or yellow papules on the nose, chin, cheeks and forehead. Milia are epidermal cysts derived from the pilosebaceous follicle.

Natural History
They are normally spontaneously extruded in a few weeks.
The cause of toxic erythema of the newborn is unknown. In majority, the onset is during the first 48 hours after birth. The eruption appears as blotchy macular erythema, their number varying from one to several hundred, most profuse on the anterior trunk, and may also affect the face and thighs. In severe cases urticarial papules develop which in 10 percent cases are surmounted by pustules, 2–4 µm in diameter. Recovery occurs rapidly, usually within 3 days.
Differential Diagnosis
These lesions have to be distinguished from miliaria, transient neonatal pustular melanosis, incontinentia pigmenti, herpes simplex virus infection, varicella, and impetigo.
Diagnosis
Toxic erythema can be distinguished from all of these by microscopic examination of a smear of pustule contents stained with Giemsa and by bacterial and viral culture. The smear in case of toxic erythema reveals cluster of eosinophils. This is in sharp contrast to bacterial infections where cluster of neutrophils are seen.
“If one does not know to which port one is sailing, no wind is favorable.”—Seneca



Treatment
As the condition is a benign self-limiting and asymptomatic one, no treatment is required.
Intertrigo is a term applied to an inflammatory dermatosis that is more or less confined to the major body folds and provoked by moisture and constant friction between opposing skin surfaces. Obesity, poor hygiene, overwarm clothing, hot and humid climatic conditions are the predisposing factors. Relative obesity of well nourished infants accounts for the unusually high incidence during the early months of life. Intertrigo is likely to become colonized and secondarily infected by both bacteria and yeast, particularly Candida albicans. Clinically, it manifests as symmetrical areas of sharply marginated erythema confined to areas of skin apposition. In infants, the folds of the neck, the axillae, the genitocrural flexures and the intergluteal cleft are the predilection sites. Miliarial lesions are readily apparent within the affected area. When C. albicans infection supervenes, erythema takes on a deep red hue and the affected area may weep. Rarely it may become superinfected with group A streptococci and Corynebacterium diphtheriae.
A severe form of irritant dermatitis can result in burn in NICU set up either from phototherapy, heater, or undiluted antseptic.
Management
Cleaning the macerated areas with mild soaps and wet compresses help.

Application of mild topical corticosteroids, e.g. clobetasone or hydrocortisone either alone or in combination with an antifungal, e.g. miconazole or clotrimazole may be helpful.
“Always forgive your enemies, nothing annoys them so much.”—Oscar Wilde




If bacterial superadded infection is evident, a topical antibacterial-like mupirocin may be useful. Application of antifungal powders can keep the areas dry because of the absorbent property of powder in addition to its antifungal action.
Miliaria occurs when the flow of eccrine sweat is impeded by obstruction of the intraepidermal portion of the sweat duct. Miliaria crystallina appears to reflect obstruction of the sweat duct within the stratum corneum. Miliaria rubra occurs when there is sweat duct obstruction deeper in the epidermis.
Miliaria crystallina presents as crops of clear thin-walled, superficial vesicles, 1–2 mm in diameter without associated erythema on the head, neck and upper trunk, usually during the first two weeks of life. They rupture within 24 hours followed by branny desquamation.
Miliaria rubra, seen most commonly in the neonatal period comprises of erythematous papules and papulovesicled, about 1–4 mm in diameter on a background of macular erythema. Staphylococcal secondary infection of miliaria may lead to sweat gland abscesses. The symmetrical crops of miliaria rubra occurs most often in flexural areas, especially around the neck, in the groins and the axillae. The face, scalp and upper trunk are frequently affected. These lesions subside in 2–3 days but recurrences are common.
Differential Diagnosis
Miliaria crystallina is distinguishable from viral infections of the skin by the lack of background erythema and by the absence of inflammatory cells or giant keratinocytes on cytological examination of the vescicles.
“If you don't know where you are going, you can never get lost.”—Herb Cohen
Miliaria rubra 8can be distinguished from toxic erythema by its flexural predominance and by the frequent presence of vescicular lesions and by the tendency to recur.


Management
Avoidance of excessive heat and humidity is the most important aspect of management. Cool baths, light clothing and installation of air conditioner in the room are helpful. Topical application of ordinary spirit (or aftershave/deodorant/body spray) gives local cooling effect and drying up of miliaria lesions. Calamine lotion also helps in most of the cases. If itching is excessive, oral promethazine or chlorpheniramine syrup may be given for 7–10 days.

Staphylococcal scalded skin syndrome (SSSS) is caused by an epidermolytic toxin elaborated by certain strains of S. aureus, commonly phage gr II. The condition is most commonly seen in the first 5 years of life. It is particularly common during the neonatal period occurring in association with purulent conjunctivitis or an upper respiratory tract infection. Sites of predilection are the central part of the face, the axillae and groins. The orange-red, scarlatiniform eruption spreads rapidly. Tenderness of the skin is an early and striking feature. The eruption gradually becomes extensive and turns to a confluent deep erythema and edema in the next 24–48 hours. The surface becomes wrinkled before starting to separate out leaving raw red erosions. The child is pyrexial and distressed. Recovery is usually rapid even without antibiotic therapy. The only differential diagnosis which poses a problem is toxic epidermal necrolysis, which is however, relatively rare in young children and is characterized by marked mucosal involvement.
Diagnosis
The diagnosis of SSSS can be established by isolation of coagulase positive Staphylococcus aureus from the pyogenic skin lesions or from nostril and areas around eyes.
Prognosis
The condition has a mortality of approximately 5 percent and fatalities occur mostly in newborns and debilitated infants.
“Ability will never catch up with the demand for it.”—Confucius


Management
Treatment should be started promptly with a penicillinase resistant antistaplylococcal antibiotic like cloxacillin or a combination of amoxicillin and clavulanic acid or cefadroxil orally. Parenteral antibiotics may be required in cases of extensive skin lesions or severely ill patients. Local cleaning of the skin with distilled water or normal saline soaked cotton is sufficient. Antiseptic cleaning is better avoided, so also application of topical antibiotic for fear of emergence of resistant strains of Staphylococcus aureus.
SUCKLING BLISTER (Fig. 1.13)
Suckling blisters are seen in newborns at birth due to vigorous suckling by the fetus in utero of several areas of the body. Bullae or erosions of 0.5–2 cm are seen over the dorsal aspect of the fingers, thumbs, wrists, lips, etc.
Differential Diagnosis
These lesions need to be differentiated from a host of conditions, e.g. bullous impetigo, epidermolysis bullosa, neonatal herpes simplex, etc.
Treatment
Topical application of antibacterial creams may help drying up of the lesions.

Infection of the neonate by herpes simplex virus is a serious condition with high mortality. The majority of these infections result from transmission of HSV1 and HSV2 by genital tract secretions during delivery. Over 70 percent of an infection with neonatal HSV have skin or mucosal lesions. Pneumonia and/or encephalitis are frequent complications. In 10 percent of the cases, the disease remains confined to the skin.
“For to win one hundred victories in one hundred battles is not the acme of skill. To subdue the enemy without fighting is the acme of skill.”—Sun Tzu



Skin manifestations are in the form of multiple grouped vesicles on erythematous patches distributed randomly over the scalp, face trunk and extremities. The vesicles have a tendency to localize over mucocutaneous junctions. Onset is between 2 and 20 days. Oral lesions in the form of erosions of the tongue, palate, gingivae and buccal mucosa are also common. Primary neonatal herpes simplex is a devastating life-threatening infection which must be diagnosed and treated with antiviral drugs promptly.
Diagnosis
Diagnosis can be coestablished with the help of Tzanck smear preparation, viral culture, use of monoclonal antibodies and nucleic acid hybridization techniques.
Management
The neonates should be isolated. Ophthalmologic examination should be performed. Prophylactic ophthalmic topical preparations, e.g. trifluridine or vidarabine are to be used. Intravenous acyclovir is the treatment of choice. It is given in a dose of 30 mg/kg/day in 3 divided doses for 14–21 days. There is no role of topical acyclovir ointment application over the lesions.
It presents as a bright red shiny polypoidal growth over the umbilicus at birth and is the result of a partially patent omphalomesenteric duct. The lesions are usually asymptomatic and secrete serous, mucoid, and rarely serosanguinous exudate. Polyps may be accompanied by potentially serious internal omphalomesenteric remnant, such as Meckel's diverticulum attached to the umbilicus by obstructing fibrous bands.

“It is terrible to speak well and be wrong.”—Sophocles, Greek Tragic Poet

Treatment
The condition is treated by surgical excision. However, underlying intestinal and urinary tract abnormalities are to be ruled out.
UMBILICAL GRANULOMA (Fig. 1.19)
It is basically a granuloma pyogenicum of the umbilicus. It presents as a red raw granulomatous growth over the umbilicus with purulent discharge.
Treatment
Treatment is cauterization with either silver nitrate solution, 20 percent potassium hydroxide or phenol.

In congenital syphilis, the fetus becomes infected with the spirochete, Treponema pallidum by way of placenta. The clinical manifestations of early congenital syphilis (those occurring before 2 years of age) are anemia, fever, wasting, hepatosplenomegaly, lymphadenopathy, rhinitis, mucocutaneous eruptions, edema, desquamation and pseudoparalysis. Of these rhinitis or snuffles is the first sign to appear. It manifests between the 2nd and 6th week of life and is the result of an ulcerous lesion of the nasal mucosa. The cutaneous lesions are seen in 1/3rd to ½ of infants affected by this disorder and appear as maculopapular or papulosquamous lesions most prominent on the face, dorsal surface of the trunk and legs, diaper area and at times palms and soles. The eruptions generally develop slowly, is bright pink or red, gradually fades to copper brown. It disappears spontaneously over 1–3 months leaving hypo- or hyperpigmented areas.


“We're different; we're the same—Richard David Bach (1936–).”—Author; Jonathan Livingston Seagull
The rare vesiculobullous, hemorrhagic lesions, when seen on the palms and soles, are highly diagnostic of this disorder. The palms and soles may be fissured, erythematous and indurated. Desquamation of the skin in large dry flakes may occur over the entire body. Mucous membrane lesions, seen in 1/3rd of the infants, are seen as weeping lesions or fissures at mucocutaneous junctions which extend out from the lips in a radiating fashion over the skin. When deep, they leave residual scars (rhagades) in the adjacent circumoral region. Raised, flat, moist wart-like lesions of condylomata lata are seen commonly over the anogenital regions, around the nares and at the angles of the mouth. About 90 percent of the infants show radiologic evidence of osteochondritis and periostitis after the first month of life, most frequently affecting the long bones.
In late congenital syphilis, the disease persists beyond 2 years of age. It includes various signs and stigmata of congenital syphilis in infants in whom the diagnosis was overlooked or those who were inadequately treated early in the course of the disease. These include dental changes manifested in the form of Hutchinson's incisors, Moon's mulberry molars, gummas affecting the bones in the skull or tibias, syphilitic arthritis, paroxysmal cold hemoglobinuria and ocular changes.
Treatment
Penicillin is the treatment of choice for all forms of congenital as well as acquired syphilis. Treatment should be started immediately after the diagnosis with aqueous crystalline penicillin G in a dosage of 100,000 units to 150,000 units/kg administered intravenously every 8–12 hours or procaine penicillin G in dosage of 50,000 units/kg administered IM once daily for 10–14 days. Patients with congenital syphilis should have repeat quantitative, nontreponemal tests 3, 6 and 12 months after treatment.
SUBCUTANEOUS FAT NECROSIS (Figs 1.21A and B)
It is a benign self-limiting dermatosis which affects apparently healthy full-term newborns and young infants. It presents as sharply circumscribed areas of indurated and nodular plaques of skin over back, buttocks, thighs and arms. Its exact etiology is not known but proposed hypotheses are pressure on bony prominenes during delivery, fetal asphyxia or hypothermia. It is also seen in infants delivered by cesarean section and infants born to diabetic mothers. The onset of fat necrosis usually occurs in the first few days to weeks of life. The lesions at times may get calcified. However, most of the lesions undergo spontaneous resolution within 2–4 weeks.


Differential Diagnosis
The condition needs to be differentiated from sclerema neonatorum which primarily occurs in newborns with sepsis, severe diarrhea, respiratory failure or dehydration and is a fatal condition with high mortality rate.
Management
Subcutaneous fat necrosis in most newborns resolve spontaneously and requires no specific therapy. Fluctuant lesions in cases of calcification should be aspirated to prevent their spontaneous rupture and secondary infection. In rare cases of hypercalcemia, restriction of calcium and vitamin D intake, systemic corticosteroids may be required.
“Wise men talk because they have something to say; fools, because they have to say something.”—Plato
It is a diffuse, fast spreading, wax-like hardening of the skin and subcutaneous tissue that occurs in premature baby or debilitated infants during the first few weeks of life. This disorder is associated with a serious underlying conditions like sepsis, respiratory distress, dehydration or diarrhea, congenital heart disease and it is characterized by a diffuse nonpitting woody induration of the involved tissues. This disease is usually starts on buttocks and legs and most of the time it progresses to involve all areas except soles, palms and genitalia. When the disease spread, the skin becomes mottled, cadaver-like, cold, stony hard and yellowish white. At that time the face acquires a fixed mask-like expression and the limbs become immobile. The infants feed poorly, show clinical signs of shock, sluggish movements and in maximum cases the baby often die. Although the etiology of this disorder is unknown, it appears to represent a nonspecific sign of grave prognostic significance rather than a primary disease. In this disorder babies are usually small, premature, lethargic, cyanotic and debilitated. Near about 25 percent of cases the mothers are ill at the time of delivery. Exposure to cold, peripheral chilling with vascular collapse, hypothermia and an increase in the ratio of saturated to unsaturated fatty acids in the triglyceride fraction of the subcutaneous tissue have been hypothesized, but lack confirmation, as possible causes for this disorder.


Prognosis
Mortality occurs in 50–75 percent of affected babies. Death is commonly due to debilitation, inanition, and the associated underlying pathologic disorders. The infants, who survive this disease, resolve without residual sequelae.
Management
Sclerema neonatorum has not any specific therapy. Supportive care with heat and administration of oxygen, control of infection, treatment of the underlying disorder, and intravenous therapy for correction of fluid and electrolyte imbalance are essential. Although indications for their use are not clear and controlled studies fail to confirm their efficacy, systemic corticosteroids in addition to antimicrobial agents have been advocated for infants with this disorder.
HAIRY PINNA (Fig. 1.24)
It is a Y-chromosome mediated trait.

“History is the version of past events that people have decided to agree upon.”—Napoleon Bonaparte
POLYTHELIA (SUPERNUMERARY NIPPLES) (Fig. 1.25)
Supernumerary nipples are the remnants of the embryological milk line which runs from the anterior axillary fold to the inner thigh. Most often they are distributed over the anterior chest wall and upper abdomen as pink, umbilicated or elevated papules surrounded by a pigmented areola. A nipple may also be seen without areola, and vice versa. Usually there is only a single lesion, but multiple or bilateral nipples are possible. It has been shown to be on the higher side being located on the left side and male gender. Accessory nipples have been reported to be associated with malformations of the urinary tract, in particular the kidneys. The association has been questioned recently.
Treatment
The accessory breast tissue may underlay the nipple and enlarge at puberty or in pregnancy. In such cases, complete excision is recommended because of the risk, of malignant change.

Also known as neonatal desquamation. This is mostly seen in postmature neonates. The exact pathophysiology of it is not known. The baby at birth may present with a membrane-like sheet around it like a collodion baby. But soon it sheds the membrane and there is scaling all over the body starting from head to toe. However, there is no ectropion, eclabion or gloved appearance. The scaling gradually subsides over a period of 4–6 weeks.



“The most exciting phrase to hear in science, the one that heralds the most discoveries, is not Eureka! (I found it!) but That's funny...’.”—Isaac Asimov
Treatment
Application of oil and emollient (white soft paraffin) help to reduce scaling and moisturise the skin of the babies.
Cutis marmorata presents as reticulated bluish mottling of the skin seen on the trunk and extremities of newborn and infants. This phenomenon is a physiologic response to chilling with resultant dilatation of capillaries and small venules. It usually disappears as the infant is rewarmed. Although a tendency to cutis marmorata may persist for several weeks or months, this disorder bears no medical significance and no treatment is usually required. In some children cutis marmorata may tend to recur until early childhood. In patients with Down's syndrome, trisomy 18, and Cornelia de Lange syndrome, this reticulated marbling pattern may be persistent. In some infants a white negative pattern of this phenomenon (cutis marmorata alba) may be created by a transient hypertonia of the deep vasculature. It is known as cutis marmorata alba. It is a transitory disorder and appears to have no clinical significance.



Treatment
No treatment is required for this physiological condition in newborns and infants. Reassurance and counseling of the parents is important.
CUTIS MARMORATA TELANGIECTASIA CONGENITA (Figs 1.27C and D)
It is a condition which closely simulates cutis marmorata telangiectasia (CMT) but does not disappear on reworming. The condition presents at or shortly after birth.

“Twenty years from now you will be more disappointed by the things you didn't do than by the ones you did do. So throw off the bowlines, Sail away from the safe harbor. Catch the trade winds in your sails. Explore. Dream. Discover.”—Mark Twain [Samuel Langhorne Clemens] (1835–1910)

The pigmentation presents as red marbled mottled patches. The changes may be limited to a localized part of the body. The skin changes get accentuated by decrease in ambient temperatre. Contrary to CMT or livedo reticularis, there may be atrophy or ulceration of the skin. There may be associated limb hypoplasia, hyperplasia or vascular abnormalities, e.g. port-wine stain, Sturge-Weber syndrome, etc. Various associated neurological disorders like macrocephaly, seizures, hydrocephalus and ocular abnormalities like glaucoma, retinal pigmentation and retinal detachment have been associated. A condition named Adams-Oliver syndrome is characterized by CMTC with aplasia cutis congenital and distal tranverse limb defects.
Within first 2–3 years of life CMTC gradually improves on its own. When the lesions are present over face, ophthalmologic check up is necessary. When there is neurological symptoms, referral to a neurologist is necessary.
Irritant dermatitis develops within 24–48 hours of exposure to irritant chemicals. In newborn babies often various antiseptic cleansers and lotions cause dermatitis of the soft and sensitive skin.
Diagnosis
Intense erythema with formation of papules and vesicles over the areas of contact with the offending agents is seen. The newborn baby becomes restless and irritable.


Treatment
Avoidance of offending agent should be prompt. Cleaning of skin with distilled water or normal saline is to be done. Application of emollient viz., white soft paraffin 2–3 times a day for 7–10 days clears the dermatitis in most of the newborn babies. Occasionally mild topical steroids, e.g. hydrocortisone or clobetasone butyrate may be required.
HARLEQUIN COLOR CHANGES
It is usually seen in premature babies but occasionally in term babies also. Due to immaturity of hypothalamic centers that control the peripheral vasculature.
“If you want to make enemies, try to change something.”—Woodrow Wilson (1856–1924)
Diagnosis
The affected newborn lying on one side of body shows reddening over the side in contact with bed and blanching over the other half of the body with clear line of demarcation. The color change comes as frequent attacks in newborns on 2nd to 6th days and may last for 20 seconds to 20 minutes.
Treatment
The condition needs to be explained to the parents and they are to be reassured.
EPSTEIN’S PEARLS AND BOHN’S NODULES
Clinically these are counterpart of facial milia. These appear as multiple discrete 2–3 mm pearly white or yellowish papules over midline of hard palate (Epstein's pearls) or gum margins (Bohn's nodules).
Diagnosis
The characteristic appearance and location clinch the diagnosis.
Treatment
It is a physiological condition in newborns and usually disappears in 4–6 weeks. This very fact needs to be explained to the parents.
SEBACEOUS GLAND HYPERPLASIA (Fig. 1.29)
It manifests as yellowish-white pinpoint papules over nose-tip in 2–10 days’ old newborns. It is due to maternal androgen stimulation. It usually disappears within first few days of life.
Diagnosis
From its characteristic appearance and site
Treatment
Reassurance of anxious mother

It is a benign self-limiting disease of unknown etiology. This rare condition is mostly seen in darker skin.
Diagnosis
Small sterile superficial vesiculopustular develop which rupture easily and evolve into hyperpigmentation. The commonly affected areas are forehead, area below chin, neck, lower back and shins. There is no systemic involvement. The condition usually disappears within 2–3 days.
Treatment
No treatment is required.
ACROPUSTULOSIS OF INFANCY
Acropustulosis of infancy is an idiopathic non-infective pustulosis affecting infants and small babies. Usually it occurs between 2 months to 3 years of age. The lesions appear as crops on a weekly or monthly basis and tends to subside by 3–4 years of age.
“I haven't failed, I've found 10,000 ways that don't work.”—Ben Franklin


Diagnosis
The lesions typically appear as pinpoint erythematous papules which transform into pustules within 24–48 hours. Palms, soles, dorsum of hands and feet are the common sites affected. Usually it is associated with moderate to severe pruritus.
Differential Diagnosis
Various closely simulating conditions are scabies with secondary infection, impetigo, dyshidrosiform eczema, erythema toxicum nenatorum, neonatal pustular melanosis, etc.

Treatment
To control pruritus antihistamines, e.g. cetirizine, levocetirizine or hydroxyzine is required. Moderately potent topical corticosteroids like mometasone or fluticasone may be used for 2–3 weeks. In severe cases dapsone has also been used.
CONGENITAL EROSIVE AND VESICULAR DERMATOSIS
The condition presents as vesicles and ulceration in newborns, almost exclusively in premature babies. The exact cause is not known but intrauterine infection, amniotic membrane adhesion are proposed hypothesis. Essentially it is a nonhereditary condition.
Diagnosis
Extensive vesicles and erosions over extremities, trunk involving up to 75 percent of body surface during first month of life in premature babies is the usual presentation. The lesions soon get crusted and subsequently heal with rippled scars. The scars over the trunk have a cobblestone-like appearance. There may be associated scarring alopecia and ulceration over the tongue. Nails may be either absent or hypoplastic. Sweating is absent over the scarred areas and the baby may present with hyperthermia. Rarely neurological defects may be seen.
“The future belongs to those who believe in the beauty of their dreams.”—Eleanor Roosevelt
Differential Diagnosis
The condition needs to be differentiated from epidermolysis bullosa (EB). Lack of involvement of face, hands and feet, characteristic rippled scars on healing and progress of lesions characterize the condition and differentiates it from EB.
Treatment
It is symptomatic and essentially care of the wound. Reassurance of parents is extremely important.
INFANTILE GLUTEAL GRANULOMA (Figs 1.30C and D)
Also known as granuloma gluteale infantum, is basically a peculiar tumor response of newborn skin to topical potent steroids. Usually there is co-presence of candidal infection.
Diagnosis
The disease characteristically presents as multiple erythematous to violaceous papulonodules over external genitalia, inner thighs and lower abdomen in infants. Usually a preceding history of potent topical steroid application is forthcoming.


Treatment
Stoppage of topical steroid application is the first thing to be done. If there is any evidence of candidal infection, topical ketoconazole or clotrimazole should be prescribed. Otherwise the lesions subside very slowly without any treatment over a period of 3–13 months. Reassurance of parents and their counseling is of paramount importance.
TRICHOSTASIS SPINULOSA (Fig. 1.30E)
It is a common disorder characterized by comedon like papule which represent horny plug with 25–50 telogen vellus hair embedded within it. The basic defect is infundibular hyperkeratosis of hair follicle which prevents shedding hence retention of telogen vellus hair originating from a single hair matrix. This entity can be classified into two variants. Classically the disease represents as comedon like papules resembling black head distributed mainly over nose and forehead in elderly individuals. Other variant characterized by pruritic follicular papule resembling keratosis pilaris distributed over the trunk and extremities of young individuals or newborns. Pathological condition commonly associated with this entity is renal failure. Diagnosis can be established with the use of dermoscope and microscope. Various treatment modalities are depilation, keratolytic, topical and systemic retinoids and hydroactive adhesive pads. Pulsed diode laser shows encouraging result.
“The time to repair the roof is when the sun is shining.”—John F. Kennedy

It is the congenital absence of skin in newborn babies, a congenital defect. Histologically there may be absence of either epidermis, dermis or subcutaneous tissue. It usually affects scalp but face, trunk or extremities can also be affected. Most of the cases of aplasia cutis congenita (ACC) are sporadic. Antithyroid drug methimazole given to a pregnant mother is likely to produce ACC in newborn babies. However, the issue is far from being conclusive.
Diagnosis
Aplasia cutis congenita (ACC) classically presents as single (occasionally two or more) sharply demarcating granulating ulcerations over scalp. The size of the lesions usually vary from 1–3 cm. Occasionally lesions may look like either a membrane or keloid.
Associations
Although most infants with ACC are otherwise well, various associated anomalies reported are cleft lip, cleft palate, hemiatrophy of limbs, ocular abnormalities, gastrointestinal malformations, spinal dysraphism, hydrocephalus, seizures, mental retardation, trisomy 13, vascular anomalies, etc.
Differential Diagnosis
Forcep injury or other types of birth injury need to be differentiated.
Treatment
By and large ACC with small defects (up to 3 cm) do not require any treatment. Proper cleaning of the area daily with betadine is required in cases of granulating lesions. Prevention of infection is very important. Most of the lesions heal with scarring by 6 weeks to 6 months, occasionally, 12 months. The scars gradually become less conspicuous over next 4–5 years. However, for bigger defects (more than 3 cm), plastic surgery is advisable.


Venous Prominence Over Bridge of the Nose
This physiological condition is seen in 1 in 10,000 live births. A transverse superficial vein remains prominent over the bridge of the nose. This condition is usually seen in 3–9 month old babies mostly. Subsequently it disappears. Similar prominent veins over the chest of babies are seen admitted in neonatal intensive care unit (NICU) with respiratory distress.
“Vision without action is a daydream. Action without vision is a nightmare.”—Japanese Proverb




Treatment
Explaining the condition and its benign self-limiting nature to the anxious mother is all that is necessary.
Erythroderma a life-threatening entity during the first one month, and many a time, a manifestation of genodermatosis, immune deficiency, psoriasis, metabolic diseases, and infections. Atopic dermatitis presenting as erythroderma is usually observed later and hence not a common differential for neonatal exfoliative dermatitis. Various causes of neonatal erythroderma are:
Cutaneous Disorders
- Infantile seborrheic dermatitis
- Atopic dermatitis
- Psoriasis
- Pityriasis rubra pilaris
- Generalized mastocytosis
- Ichthyosis: Nonbullous ichthyosiform erythroderma, Conradi-Hünermann syndrome, bullous ichthyosiform erythroderma“Smooth seas do not make skilful sailors.”—African proverb
- Netherton syndrome
- Toxic epidermal necrolysis, ectodermal dysplasia.


Infections
- Staphylococcal scalded skin syndrome (SSSS)
- Toxic shock syndrome
- Candidiasis.
Immunodeficiency
- Omenn syndrome
- Graft-versus-host reaction.

Metabolic Disorders
- Disorders of biotin metabolism
- Essential fatty acid deficiency
- Acrodermatitis enteropathica
- Leiner's disease.
Drugs
- Ceftriaxone
- Vancomycin.
Diagnosis
Infantile seborrheic dermatitis(isd) which manifests in the neonatal period, usually presents with greasy scales on the scalp (cradle cap), skin folds like the axilla, neck, retroauricular, and diaper areas. Atopic dermatitis may have its onset in the first month; however, it is rarely erythrodermic in neonates. The lesions usually are vesicular and exudative in nature. Sometimes there is a significant overlapping between infantile seborrheic dermatitis and atopic dermatitis.
Neonatal psoriatic erythroderma is a rare entity and it commonly presents as recalcitrant diaper dermatitis which may become generalized with a widespread pustular form of the disease. This is accompanied by periodic high fever, and the child becomes very toxic with recurrent crops of superficial pustules appearing on erythematous plaques.
Psoriasis and pityriasis rubra pilaris may look similar with erythematous scaly plaques which may enlarge and become generalized to produce erythroderma. Heavy infiltration of the entire skin with mast cells results in diffuse cutaneous mastocytosis.
“It's much easier to turn a friendship into love, than love into friendship.”—Proverb
23The skin undergoes lichenification and is erythematous, producing urtication and bulla formation on mild trauma. Diarrhea, flushing, and respiratory symptoms are the common accompaniments. Darier's sign, a wheal which flares on stroking the skin, is often positive. Although a life-threatening condition, it improves with age. Several varieties of ichthysoses can manifest as erythroderma. Patients of nonbullous congenital ichthyosiform erythroderma have finer scales and are more inclined to develop erythroderma. The newborns have a collodion membrane which desquamates, revealing the erythroderma. It fades in mild disease but in the severe classic form, large platelike scales with erythema persist. Harlequin ichthyosis infants with hyperkeratotic fissured plates often die due to respiratory problems; if they survive with treatment, they manifest generalized erythroderma. Epidermolytic hyperkeratosis or bullous ichthyosis have widespread denuded areas which resolve slowly, manifesting underlying erythroderma. Netherton syndrome presents with features of generalized erythroderma, fragile hair with trichorrhexis invaginata (bamboo hair), and severe rhinorrhea, asthma, anaphylaxis due to food, and so on. Erythroderma at birth is often the onset and it is a diagnostic dilemma where sparse hair with shaft defects may take several microscopic examinations, especially of eyebrows and lashes, before clinching the diagnosis. These patients are atopic and often have intercurrent infective episodes with high rates of mortality. The serum IgE levels are markedly raised and are even more than seen normally in atopic subjects.
Because of the protective effect of maternal immunity, congenital immunodeficiency syndromes are rarely symptomatic at birth. Graft-versus-host reaction from maternal engraftment can, however, occur even during intrauterine development. Omenn syndrome is a familial reticuloendotheliosis with eosinophilia having erythroderma, failure to thrive, lymphadenopathy, and recurrent infections. Marked leukocytosis, eosinophilia, anemia, and hypogammaglobulinemia are some of the findings in this histiocytic disorder. Hypogammaglobulinemia can start with diarrhea and periodic fever together with erythroderma. Dermatitis begins by four weeks of age and rapidly generalizes. DiGeorge syndrome and severe combined immunodeficiency may also present with eczematous dermatitis leading to erythroderma.
Graft-versus-host reaction may occur in T cell immunodeficiency or as a result of transplacental transfer of maternal lymphocytes as a sequela of exchange transfusion. An erythematous nonspecific morbilliform rash may lead to erythroderma and epidermal sloughing. Neonatal cutaneous T cell lymphoma can present with congenital ichthyosis with atypical Sezary-like lymphoid cells in skin and lymph nodes and other immunological abnormalities.
Metabolic and nutritional disorders are suspected when the infant has failure to thrive and the dermatitis manifests periorificially at the onset before it generalizes. Severe protein malnutrition during infancy can present with widespread erythema, edema, erosion, and desquamation of the skin. Deficiency of zinc due to malabsorption as in acrodermatitis enteropathica or low concentration of zinc in breast milk can begin with psoriasiform dermatitis in circumoral or periorificial areas which may crust and spread to involve other areas; this has also been reported in children with acquired immunodeficiency syndrome. Diarrhea, failure to thrive, irritability, and photophobia can accompany such dermatitis. Essential fatty acids, mostly found in dairy products and vegetable oils, are supplemented in the diet. Diffuse desquamation, lichenification, and intertriginous dermatitis can develop in such situations. Cystic fibrosis dermatitis presents with psoriasiform diaper rash not responsive to topical steroids or antifungals. This dermatitis may spread and is associated with growth failure and irritability. Deficiency of holocarboxylase synthetase manifests with neonatal erythroderma. The children have alopecia, secondary cutaneous candidiasis, dehydration, and ketoacidosis which can lead to a fatal outcome. Deficiency of holocarboxylase synthetase in skin fibroblasts clinches the diagnosis. Deficiency of biotinidase presents with patchy alopecia and acrodermatitis enteropathica-like skin lesions. These conditions encompass the group of ‘multiple carboxylase deficiency’ disorders. Penicillins, aminoglycosides, and cephalosporins often produce erythematous maculopapular skin lesions, but rarely erythroderma. Ceftriaxone and vancomycin in neonates may produce erythroderma, and vancomycin may also induce hypotension on account of histamine release.
Leiner's disease is literally a clinical phenotype of acquired erythroderma, diarrhea, and failure to thrive. Desquamative generalized erythema and dermatitis with weight loss was thought to be common in breast-fed infants due to the deficiency of biotin. Cases of generalized dermatitis in seborrheic pattern due to immunodeficiencies were also included in this category.
Treatment
Managing neonatal erythroderma is a therapeutic challenge as it is very difficult to treat this potentially life-threatening situation. Careful monitoring of the vital signs, maintenance of fluid and electrolyte balance, and prevention of hyperpyrexia are mandatory in the management. Application of emollients, wet dressings, topical steroids, and systemic antibiotics are the other modalities. Maintaining the skin barrier and proper hydration is the key to managing most of the conditions.
“A real friend is someone who walks in when the rest of the world walks out.”—Proverb
CARE OF THE NEWBORN SKIN
The skin is the first barrier of the newborns to counter various noxious factors/agents of the environment once the baby comes out of the safe and secured intrauterine life to the external world. Various aspects of newborn skin care will be discussed under different headings.
Need for Special Skin Care for Babies
Baby's protective but delicate cover needs to be kept in a healthy condition and it should be disturbed as little as possible. Topical agents are more rapidly absorbed into infant skin due to deficient intercellular bridges. Besides, greater body surface area to weight ratio than adults also facilitates easy absorption and toxicity of topically applied substances. Infant skin cannot withstand the toxicity of most substances as they make this delicate skin more susceptible to electrolyte imbalance, fluid imbalance and thermal instability. Infant skin is particularly very sensitive to cleansing agents as they contain stronger chemicals and may be drying. Hence the product should be guaranteed of safety for use on babies.
Skin problems pertaining to dryness are common in babies due to inadequacies in the epidermal barrier. The skin irritation potential towards topical applicants is also more. Maintaining skin integrity and preventing exposure to toxic substances in childhood assures healthy skin for several years ahead.
Care of the Newborn Skin
Skin of the newborns performs the most challenging task as it is the outermost cover of the body. Moreover, it is confronted with various factors, viz, temperature changes, friction, microbes, etc of the external world once the baby is born. As the structure and functions of the skin depend on whether a child is born at term or prematurely, skin care is related to gestational age.
At birth, microbial colonization of newborn skin is almost nil. But over a few days, aerobic flora occupies skin at different concentrations at different sites, e.g. mostly over groins, axillae and scalp. Coagulase negative staphylococci (Staphylococcus epidermidis) are the most commonly found microorganisms. Staphylococcus aureus appears only as contamination, usually from mother or nursing staffs.
Skin Care at Birth
Removal of Vernix Caseosa
At birth the baby's skin is coated with vernix caseosa, blood, meconium and cellular debris. Vernix caseosa contains both epidermal (triglycerides and cholesterol) and sebaceous (squalene and waxes) fat. Premature infants tend to have less of vernix than term babies and postmature babies have little vernix. There is considerable interindividual variation in the quality of vernix caseosa.
Washing and Bathing
A bath is an ideal means of cleaning an infant completely. A bath in infant should not last for more than five minutes. The bath for more than 5 minutes increases the hydration of skin and, thereby, reduces the threshold for friction. Infants can be bathed immediately after birth irrespective of the falling of the umbilical cord stub. But usually the first bath is not given till 3rd/4th weeks of life. If there is history of premature rupture of membrane and the baby is meconium-stained, immediately the baby should get the bath. The water should be boiled and the temperature should not be exceeding 37°C for bathing newborns. A solid or liquid cleanser or a syndet can be used to clean baby skin. Bubble bath can also be given but not for too long or too frequently as can it can cause irritation. After bath, infants must be dried thoroughly, particularly over skin creases, groins and axillae.
Napkin Changes
Napkin should be changed frequently, at least at each nursing and feeding time. It should be carefully washed in lukewarm water and then rinsed off and dried thoroughly.
The diaper area is specifically vulnerable because it is a closed environment suitable for microorganisms and with frequent wetting, it is more often moist and dry; hence the skin becomes prone to maceration and increases its permeability to other irritants.
The skin here is constantly in contact with strong alkalinizing agents, e.g. urine and feces and the pH here is prone to high alkalinity that damages the skin integrity. It is, thus, very important to be well-aware of the need to change nappies and the range of products that are available to prevent any rash or irritation in the nappy area.
Nappy rash can be reasonably prevented by reducing moisture by the frequent changing of nappies. This would reduce contact between urine, feces and the skin. However, this does not seem feasible at most instances. In such cases, using partially occlusive agent like mineral oil on the buttocks can help to form a physiological barrier that minimizes this interface. As far as possible, air exposure should be increased by allowing the child to move around the house bare-bottomed. Plastic pants should be avoided as they reduce the air circulation to the skin. Warm water and soft cotton wool should be used to wipe the nappy area. Feces have a tendency to stick and scrubbing only worsens the status of the delicate skin. Here, the use of an emulsion like baby lotion can ease the removal by reducing the surface tension and cleaning the debris.
“A tree is known by its fruit; a man by his deeds. A good deed is never lost; he who sows courtesy reaps friendship, and he who plants kindness gathers love.”—Saint Basil the Great
25Skin should then be thoroughly dried each time the diaper is changed by exposing it for a few minutes. The bottom should be wiped from front to back to avoid fecal matter from reaching the genitals. After each wash, powder should be applied in the skin folds to prevent friction due to wetting as well as to avoid candidal colonization due to excess moisture in the area. Soaps should be mild and should be used very rarely if a rash has developed.
In general, the nappies should be made of cotton cloth and should be home laundered with mild detergents. Disposable diapers should be avoided as far as possible. However, some newer diapers allow the moisture to stay away from the baby's bottom. They keep the skin relatively dry and reduce the risk of developing the rash. Nappy pads with cotton padding are more suited.
Scalp
Shampoo helps to remove scales and crust from the scalp (cradle cap). If the first sign of seborrheic dermatitis appears, application of mineral or vegetable oil limits the spread of lesions.
Nails
Nail should be regularly cut and kept short and clean.
Ears
Cotton swabs soaked in boiled water should be used to clean ears. Special care should be taken not to hurt auditory canals.
Umbilicus
After birth umbilical cord dries out and drops off within five to ten days. Certain products containing eosin or others stains are often used. However, they act more as drying agents rather than as antiseptics.
Skin Care in the Premature Infants
After birth, skin maturation proceeds rapidly in preterm infants. These infants are kept warm and nursed in closed incubators. Environmental conditions in these units are potentially harmful for infant skin, which is subject to scarring. Cosmetically or functionally, significant lesions may be caused by needle marks, central venous catheters, transcutaneous oxygen monitoring, chest drain insertion, extravasation of intravenous fluid or skin stripping due to adhesive tape. To reduce the frequency and severity of skin damage, neonatal staffs need to know that many routine procedures can lead to long-term scarring and atrophy. Heaters should be kept at a safe distance, otherwise skin burn can occur in NICU set up (Fig. 1.33).

Preventive Measures
Disinfection
The most common infective agents causing septicemia are coagulase-negative staphylococci in relation to catheter placement. For prevention, maintain hygiene by hand washing of the staff and parents. Cleaning with chlorhexidine-alcohol and povidone-iodine, two consecutive 10 seconds cleaning destroys more than a single 10 seconds wipe.
Incubator
Frequent change of infants’ position in the incubator reduces the risk of skin erosion and impending bedsore. Fingers and toes must be kept visible. Catheters or needles should be secured with a transparent tape to allow easy detection of fluid extravasation. Scarring alopecia can develop following pressure ulcer. The occurrence of nonblanchable erythema and disruption of epidermis indicate impending ulcer. The occurrence of scarring alopecia has been reported in infants from pressure necrosis.
Transcutaneous Oxygen Monitors
Transcutaneous oxygen monitors should not be left in place for more than one hour without surveillance.
“There is no distance too far between friends, for friendship gives wings to the heart.”—Kathy Kay Benudiz
26Nonblanchable erythema has been reported with keeping such electrodes for prolonged period. The use of karaya electrodes has been demonstrated to be effective in cardiorespiratory monitoring with decreased trauma to the neonatal skin. Placement of electrodes on the limbs, especially in very low birth weight infants, can eliminate the need to frequently remove these pads to facilitate auscultation or other assessment of the chest wall.
Minimal Use of Tape and Adhesive
The skin of the premature infants may be damaged by repeated attachment and removal of adhesive tapes to secure electrodes, IV cannulas, drains, etc. Adhesives should be used on small areas of skin and removed gently with warm water soaked gauze and diluted soap, but not alcohol, which may be irritant for baby's skin.
Emollients
Application of emollient is a safe and effective way to decrease neonatal peeling and scaling dermatitis. Vegetable oil (e.g., olive oil), lanolin, petroleum-based ointments applied gently to the skin, reduce scaling and fissuring as well as increase skin hydration.
Skin Care of the Term Baby and Infant
The large number of infant skin-care products available over the counter is at times confusing for the average consumers. These have been the gifts of media and so-called health magazines for the lay people with all rosy advertisements. By and large the principle followed by a doctor should be to advice the parents to go for a product marketed by a multinational company or a company of good repute and stature or a product, which has been in the market for a considerable period of time and thus has stood “the test of time”. Several types of products are used; viz. soaps, shampoos, antiseptics, moisturizers, etc.
Detergents
The term ‘detergent’ designates a substance capable of cleaning the skin, i.e. of removing impurities (dust, grease organic secretions, microorganisms). Washing with water alone does not remove all the impurities on the skin surface. Some are only fat soluble, thus requiring the use of products capable of emulsifying the fatty substance into fine droplets, which can then, be carried away by rinsing. These products are known as surfactants, act by suppressing the surface tension, which allows fatty substances to remain on the skin surface. Detergents act by reducing the surface tension between water and air, creating a foaming effect not directly correlated with the cleaning properties of the product. As a rule, a higher foaming power increases the risk of damage to the skin. Detergents are classified as ionic or nonionic products. In infants detergents should be used cautiously, followed by a thorough rinsing. Too much removal of lipids from the stratum corneum would eliminate those essential to the surface ecosystem.
Soaps are the products of saponification, i.e. the action of alkali on a fatty substance. In hard water, soaps tend to precipitate.
Syndets or synthetic detergents do not have the theoretical disadvantages of soap but are subject to rapid disintegration. They can produce excessive dryness of skin, if moisturizers are not added to it. Antiseptic soaps are useful in preparation of an operative field, but are unsuitable for daily use in infants as they can cause irritation to infants’ skin. Moreover, antiseptic soaps remove the commensal organisms from the skin surface, thereby, making the skin prone to attack by virulent pathogenic organisms from outside.
Bubble bath products attract the infants and their parents because of its colorings and perfumes and, thereby, mask the risk of prolonging a bath and irritating the genital mucosa.
Most baby shampoos in the market contain anionic surfactant which ensure adequate cleansing. The pH should be close to that of tears and, thereby, won't cause irritation to the eyes. Special ingredients, e.g. selenium sulfide, ketoconazole or zinc pyrithione may be added to the shampoos for seborrheic dermatitis or seborrhea scalp. The basic principles of use of various antiseptics and emollients in term babies and infants are essentially the same as in preterm babies.
Protective Creams
These are basically prepared to reduce the risk of irritation, particularly napkin rash, by isolating skin from numerous irritants for baby's skin. The creams contain a fatty phase, an aqueous phase, a surfactant, additives (zinc oxide), scents and preservatives. These creams can paradoxically cause increased occlusion and irritant dermatitis to its ingredients.
Powders
These are useful to absorb moisture during hot and humid weather. They can prevent maceration over the skin folds in infants. However, too much of their use can lead to blockade of sweat-duct pores resulting in miliaria formation.
“And remember, no matter where you go, there you are.”—Confucius
Role of Massage
The act of touch fulfils the basic need to feel safe, comfortable and loved. Touch is also an intrinsic factor in child development. Touch is proposed to play a role in growth, development and overall well-being. Massage is one of the most beautiful and gentle methods of touch. It is practiced in most countries and has recently been researched extensively in western countries. Indian form of infant massage is appreciated all over the world. It has been seen that massage with oil is more beneficial as compared to massage without oil. It is important to note that the oil used in such a situation ought to be smooth, of optimum viscosity and friction free or else it would lead to abrasions on the skin surface. The oil should be nonocclusive so that it does not block the skin pores and allows the skin to breathe. It ought to be safe and mild to suit the baby's delicate skin and the ingredients should be thoroughly tested for their potential to cause contact sensitivity. Mineral oil is one of the best-known moisturizing ingredients ever found. It spreads easily and has a long lasting tactile effect, making it an extremely efficacious emollient. Omission of low molecular weight hydrocarbons alleviates risks of carcinogenicity while the large particle size renders it incapable of blocking pores making it noncomedogenic.
Massage should be started after one month and can easily continue till ten years and over. Benefits of massage are numerous. Appropriate knowledge of correct massage techniques is important in order to attain maximum therapeutic benefits from it. Complete head to toe massage should be a daily routine. But massage should be gentle and judicious. However, massage should be withheld for a few days in case either the baby has got any contagious infection of skin or the person offering massage has any infection over hands. Massage given by the mother increases the bondage between the mother and her baby. It helps in the physiological and psychological development of the babies.
“One loyal friend is worth ten thousand relatives.”—Euripides, Greek playwright