

Pathology is a science dealing with the study of diseases. Four important components of pathology are etiology (causative factors), pathogenesis (mechanism or process by which disease develops), morphology (appearance of cells, tissues or organs) and clinical features.
CELL INJURY
Disease occurs due to alteration of the functions of tissues or cells at the microscopic level. The various causes of cell injury include:
-
Hypoxia: It is the most common cause of cell injury. It results due to decrease in oxygen supply to the cells. Hypoxia may be caused by
-
Physical Agents: Cell injury may occur due to radiation exposure, pressure, burns, frost bite etc.
-
Chemical Agents: Many drugs, poisons and chemicals can result in cell injury.
-
Infections: Various infectious agents like bacteria, virus, fungus and parasites etc can cause cell injury.
-
Immunological reactions: These include hypersensitivity reactions and autoimmune diseases.
-
Genetic causes: Cell injury can also result due to derangement of the genes.
-
Nutritional imbalance: Cell injury can result due to deficiency of vitamins, minerals etc.
Clinical Importance
In response to injury, a cell/tissue can have following consequences:
-
Adaptation: The cell changes its physiological functions in response to an injurious stimulus.
-
Reversible cell injury
-
Irreversible cell injury.
-
REVERSIBLE CELL INJURY: As already discussed, hypoxia is the most common cause of cell injury. Oxygen is an important requirement of mitochondria for the formation of ATP; therefore, hypoxia will result in earliest involvement of mitochondriaQ resulting in decreased formation of ATP. All cellular processes requiring ATP for normal functioning will be affected. Important organelles affected are cell membranes (require ATP for functioning of Na+ - K+ pump), endoplasmic reticulum (require ATP for protein synthesis) and nucleus.


All the features discussed above are of reversible cell injury because if the injurious agent is removed at this point, cell can recover back to its normal state of functioning. However, if the stimulus continues, then irreversible cell injury ensues.
-
IRREVERSIBLE CELL INJURY: Features of irreversible cell injury include
-
Damage to cell membrane: It results due to continued influx of water, loss of membrane phospholipids and loss of protective amino acids (like glycine). Damage to cell membranes result in massive influx of calcium.
-
Calcium influx: Massive influx of Ca2+ results in the formation of large flocculent mitochondrial densities and activation of enzymes.
-
Nuclear changes: These are the most specific microscopic features of irreversible cell injury. These include: *Pyknosis, *Karyorrhexis and *Karyolysis.
-

Irreversible cell injury may be necrosis or apoptosis (Programmed cell death)
Necrosis | Apoptosis |
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

APOPTOSIS
Apoptosis or programmed cell death can be induced by intrinsic or extrinsic pathway. Normally, growth factors bind to their receptors in the cells and prevent the release of cytochrome C and SMAC. So, withdrawal or absence of growth factors can result in release of these mediators and initiate the intrinsic pathway.
Intrinsic pathway: It is initiated by the release of cytochrome C and SMAC (second mitochondrial activator of caspases) from the mitochondrial inter-membrane space. Upon release into the cytoplasm, cytochrome C associates with dATP, procaspase-9 and APAF-1 (apoptosis activating factor -1) leading to sequential activation of caspase-9 and effector caspases {Caspases- 3 and -7}. On the other hand, upon release, SMAC binds and blocks the function of IAPs (Inhibitor of Apoptosis Proteins). Normally, IAPs are responsible for causing the blocking the activation of caspases and keep cells alive and so, neutralization of IAPs permits the initiation of a caspase cascade.
Extrinsic pathway: It is activated by binding of Fas ligand to CD95 (Fas; member of TNF receptor family) or binding of TRAIL (TNF related apoptosis inducing ligand) to death receptors DR4 and DR5. This induces the association of FADD (Fas- associated death domain) and procaspase-8 to death domain motifs of the receptors resulting in activation of caspase 8 (in humans caspase 10) which finally activates caspases- 3 and 7 that are final effector caspases. Cellular proteins particularly a caspase antagonist called FLIP, binds to procaspase-8 but can not activate it. This is important because some viruses produce homologues of FLIP and protect themselves from Fas mediated apoptosis.

REGULATION OF APOPTOSIS
Regulation is primarily by bcl-2 family of genes located on chromosome 18. Some members of this family like bak, bid, bin, bcl-xS (to remember, S for stimulate apoptosis) stimulate apoptosis whereas others like bcl-2, bcl-xL (to remember, L for lower apoptosis) etc inhibit apoptosis.

Normal cells have bcl-2 and bcl-xL present in the mitochondrial membrane. They inhibit apoptosis because their protein products prevent the leakage of mitochondrial cyt ‘c’ into the cytoplasm. When there is absence of growth factors or hormones, bcl-2 and bcl-xL are replaced by bax, bin etc. resulting in increased permeability of mitochondrial membrane. This result in stimulation of intrinsic pathway of apoptosis (described above in flowchart).
EXAMPLES OF APOPTOSIS
Physiological conditions | Pathological conditions |
|---|---|
|
|
-
ADAPTATION: Cells may show adaptation to injury by various processes like atrophy, hypertrophy, hyperplasia, metaplasia, dysplasia etc.
Atrophy | Hypertrophy | Hyperplasia |
|---|---|---|
|
|
|
Metaplasia | Dysplasia |
|---|---|
|
|
INTRACELLULAR ACCUMULATIONS
Various substances like proteins, lipids, pigments, calcium etc. can accumulate in cells.
-
Proteins: Proteins are synthesized as polypeptides on ribosomes. These are then re-arranged into α-helix or β sheets and folded. Chaperoneshelp in protein folding and transportation across endoplasmic reticulum and golgi apparatus. Chaperones thus can be induced by stress (like heat shock proteins; hsp 70 and hsp 90). They also prevent ‘misfolding’ of p roteins. However, if misfolding occurs, chaperones facilitate degradation of damaged protein via ubiquitin-proteasome complex.7
Disorders with protein defects
Defect in transport and secretion of proteins | Misfolded/unfolded proteins |
|---|---|
Accumulation of proteins inside cells | Initially increase chaperone concentration, Later, these induce apoptosis by activating caspases |
|
|
-
Lipids:
-
Triglycerides: Fatty change in liver, heart and kidney (stained with Sudan IV or Oil Red O).
-
Cholesterol: Atherosclerosis, xanthoma
-
Complex lipids: Sphingolipidosis
-
-
Endogenous Pigments:Lipofuscin (wear and tear pigment)MelaninHemosiderin
-
Perinuclear, brown coloured pigment
-
Responsible for brown atrophyQ of liver and heart
-
It is derived through lipid peroxidation of polyunsaturated lipids of subcellular membranes and is indicative of free radical injury Q to the cell
-
Seen in aging, protein energy malnutrition and cancer cachexia.
-
Only naturally occurring endogenous black pigment derived from tyrosineQ
-
Responsible for pigmentation of skin and hair
-
Golden yellow pigment
-
Seen at sites of hemorrhage or bruiseQ
-
Also seen in hemochromatosisQ (Iron overload)
-
-
Hyaline change: It is any intracellular or extracellular accumulation that has pink homogenous appearance.IntracellularExtracellular
-
Mallory alcoholic hyaline
-
Russell bodies (seen in multiple myeloma)
-
Zenker's hyaline change
-
Hyaline membrane in newborns
-
Hyaline arteriosclerosis
-
Corpora amylacea in prostate, brain, spinal cord in elderly, old lung infarct
-
-
Calcification: Pathologic calcification is the abnormal tissue deposition of calcium salts, together with smaller amounts of iron, magnesium, and other mineral salts. It can be of the following two types:DystrophicMetastatic
-
Seen in dead tissuesQ
-
Serum calcium is normalQ
-
Seen at sites of necrosisQ
-
Often causes organ dysfunction
-
Examples include:R – Rheumatic heart disease (in cardiac valves)A – Atheromatous plaqueT – Tubercular lymph nodeTumors (MOST for PG)
-
M – Meningioma, Mesothelioma
-
O – Papillary carcinoma of Ovary (serous ovarian cystadenoma)
-
S – Papillary carcinoma of Salivary gland
-
T – Papillary carcinoma of Thyroid
-
Prolactinoma
-
Glucagonoma
-
-
Seen in living tissues also
-
Association with elevated serum Ca2+
-
Does not cause clinical dysfunction
-
Seen in
-
HyperparathyroidismQ
-
Renal failureQ
-
Vitamin D intoxicationQ
-
SarcoidosisQ
-
Milk alkali syndromeQ
-
Multiple myelomaQ
-
Metastatic tumors to boneQ
-
-
Found in organs which loose acid and have alkaline environment inside them [like lungs (most commonly), kidneys, stomach, systemic artery, pulmonary veins etc]
-
REPERFUSION INJURY
It is seen with cerebral or myocardial injury. On re-establishment of blood flow, there is increased recruitment of white blood cells which cause inflammation as well as generation of more free radicals.
CELLULAR AGEING
Features of ageing include decreased oxidative phosphorylation, decreased synthesis of nucleic acids and proteins, deposition of lipofuscin, accumulation of glycosylation products and abnormally folded proteins. The most effective way to prolong life is calories restriction because of a family of proteins called SIRTUINS. The latter have histone deacetylase activity and promote expression of genes whose products increase longevity.
-
Ends of the chromosomes are known as telomeres. Enzyme telomerase helps in keeping the length of telomere constant. Decreased activity of this enzyme is associated with ageing whereas excessive activity is associated with cancers.

FREE RADICAL INJURY
Free radical injury is caused by the following mechanisms:
-
Oxidative stress/reactive oxygen species (O2–, H2O2, OH)
-
Radiation exposure
-
Drugs (carbon tetrachloride, paracetamol)
-
Metals (iron, copper):
Mechanism of Free Radical Injury
It can result in lipid peroxidation, DNA breaks and fragmentation of the proteins. This is associated with formation of more free radicals thereby making free radical induced injury as an autocatalytic reaction.9
Antioxidants
Antioxidants may act by inhibiting the generation of free radials or scavenging the already present free radicals. These may be divided into enzymatic and non-enzymatic.
Enzymatic | Non-enzymatic |
|---|---|
|
|
-
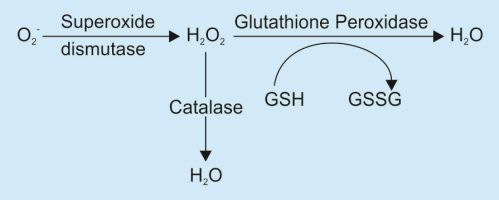
Catalase is present in peroxisomes and decomposes H2O2 into O2 and H2O. (2 H2O2 → O2 + 2 H2O).
-
Superoxide dismutase is found in many cell types and converts superoxide ions to H2O2. (2 O2- + 2 H→ H2O2 + O2).This group includes both manganese-superoxide dismutase, which is localized in mitochondria, and copper-zinc-superoxide. dismutase, which is found in the cytosol.
-
Glutathione peroxidase also protects against injury by catalyzing free radical breakdown. (H2O2 + 2 GSH → GSSG [glutathione homodimer] + 2 H2O, or 2 OH + 2 GSH →GSSG + 2 H2O).
CHEMICAL FIXATIVES
-
Chemical fixatives are used to preserve tissue from degradation, and to maintain the structure of the cell and of sub-cellular components such as cell organelles (e.g., nucleus, endoplasmic reticulum, mitochondria).
-
The most common fixative for light microscopy is 10% neutral buffered formalin (4% formaldehyde in phosphate buffered saline).
-
For electron microscopy, the most commonly used fixative is glutaraldehyde, usually as a 2.5% solution in phosphate buffered saline.
-
These fixatives preserve tissues or cells mainly by irreversibly cross-linking proteins.
-
Frozen section is a rapid way to fix and mount histology sections. It is used in surgical removal of tumors, and allow rapid determination of margin (that the tumor has been completely removed). It is done using a refrigeration device called a cryostat. The frozen tissue is sliced using a microtome, and the frozen slices are mounted on a glass slide and stained the same way as other methods.
Commonly Used Stains
Substance | Stain |
|---|---|
Glycogen | Carmine (best), PAS with diastase sensitivity |
Lipids | Sudan black, Oil Red ‘O’ |
Amyloid | Congo Red, Thioflavin T (for JG apparatus of kidney) and S |
Calcium | Von Kossa, Alzarine Red |
Hemosiderin | Perl's stain |
Trichrome | CollagenQ appears blue, while smooth muscleQ appears red. |
MULTIPLE CHOICE QUESTIONS
CELL INJURY, NECROSIS, APOPTOSIS
1. CD 95 is a marker of
(AIIMS Nov 2012)
-
Intrinsic pathway of apoptosis
-
Extrinsic pathway of apoptosis
-
Necrosis of cell
-
Cellular adaption
2. Which of the following is the characteristic of irreversible injury on electron microscopy?
(AIIMS May 2012)
-
Disruption of ribosomes
-
Amorphous densities in mitochondria
-
Swelling of endoplasmic reticulum
-
Cell swelling
3. Caspases are associated with which of the following?
(AIIMS May 2010)
-
Hydopic degeneration
-
Collagen hyalinization
-
Embryogenesis
-
Fatty degeneration
4. Caspases are seen in which of the following?
(AI 2010)
-
Cell division
-
Apoptosis
-
Necrosis
-
Inflammation
5. Light microscopic characteristic feature of apoptosis is:
(AI 2010)
-
Intact cell membrane
-
Eosinophilic cytoplasm
-
Nuclear moulding
-
Condensation of the nucleus
6. Coagulative necrosis is found in which infection?
(AI 2009, AIIMS May’ 10)
-
TB
-
Sarcoidosis
-
Gangrene
-
Fungal infection
7. Organelle which plays a pivotal role in apoptosis is:
(AI 2011, 09, AIIMS May 2010)
-
Cytoplasm
-
Golgi complex
-
Mitochondria
-
Nucleus
8. All of the following statements are true regarding reversible cell injury, except (AI 2005)
-
Formation of amorphous densities in the mitochondrial matrix
-
Diminished generation of adenosine triphosphate (ATP).
-
Formation of blebs in the plasma membrane.
-
Detachment of ribosomes from the granular endoplasmic reticulum.
9. Fibrinoid necrosis may be observed in all of the following, except: (AI 2005)
-
Malignant hypertension
-
Polyarteritis nodosa
-
Diabetic glomerulosclerosis
-
Aschoff's nodule
10. In apoptosis, Apaf-I is activated by release of which of the following substances from the mitochondria?
(AI 2005)
-
Bcl-2
-
Bax
-
Bcl-XL
-
Cytochrome C
11. Which of the following is an anti-apoptotic gene?
(AI 2004)
-
C-myc
-
p 53
-
bcl-2
-
bax
12. Annexin V on non-permeable cell is indicative of:
(AIIMS May 2009)
-
Apoptosis
-
Necrosis
-
Cell entering replication phase
-
Cell cycle arrest
13. Ultra-structural finding of irreversible injury
(AIIMS Nov 2007)
-
Ribosomal detachment from endoplasmic reticulum
-
Amorphous densities in mitochondria
-
Formation of phagolysosomes
-
Cell swelling
14. Caspases are involved in
(AIIMS Nov 2007)
-
Necrosis
-
Apoptosis
-
Atherosclerosis
-
Inflammation
15. True about Apoptosis are all except:
(AIIMS May 2007)
-
Inflammation is present
-
Chromosomal breakage
-
Clumping of chromatin
-
Cell shrinkage
16. The following is an antiapoptotic gene
(AIIMS Nov 2006)
-
Bax
-
Bad
-
Bcl-X
-
Bim
17. Cytosolic cytochrome C plays an important function in
(AIIMS Nov 2006)
18. Most pathognomic sign of irreversible cell injury
(AIIMS Nov 2006)
-
Amorphous densities in mitochondria
-
Swelling of the cell membrane
-
Ribosomes detached from endoplasmic reticulum
-
Clumping of nuclear chromatin
19. Internucleosomal cleavage of DNA is characteristic of
(AIIMS Nov 2005)
-
Reversible cell injury
-
Irreversible cell injury
-
Necrosis
-
Apoptosis
20. Programmed cell death is known as:
(AIIMS Nov 2005)
-
Cytolysis
-
Apoptosis
-
Necrosis
-
Proptosis
21. Ladder pattern of DNA electrophoresis in apoptosis is caused by the action of the following enzyme:
(AIIMS Nov 2004)
-
Endonuclease
-
Transglutaminase
-
DNAse
-
Caspase
22. Which finding on electron microscopy indicates irreversible cell injury?
(AIIMS Nov 2002)
-
Dilatation of endoplasmic reticulum
-
Dissociation of ribosomes from rough endoplasmic reticulum
-
Flocculent densities in the mitochondria
-
Myelin figures
23. True about apoptosis is all, except:
(AIIMS Nov 2001)
-
Considerable apoptosis may occur in a tissue before it becomes apparent in histology
-
Apoptotic cells appear round mass of the intensely eosinophilic cytoplasm with dense nuclear chromatin fragments
-
Apoptosis of cells induce inflammatory reaction
-
Macrophages phagocytose the apoptotic cells and degrade them
24. Morphological changes of apoptosis include
(PGI Dec 01)
-
Cytoplasmic blebs
-
Inflammation
-
Nuclear fragmentation
-
Spindle formation
-
Cell swelling
25. True about apoptosis
(PGI June 2003)
-
Migration of Leukocytes
-
End products are phagocytosed by macrophage
-
Intranuclear fragmentation of DNA
-
Activation of caspases
-
Annexin V is a marker of apoptotic cell
26. Which of the following is the hallmark of programmed cell death?
(Delhi PG 2009 RP)
-
Apoptosis
-
Coagulation necrosis
-
Fibrinoid necrosis
-
Liquefaction necrosis
27. Which of the following is an inhibitor of apoptosis?
(Delhi PG-2006)
-
Bad
-
Bax
-
Bcl-2
-
All of the above
28. Inhibitor of apoptosis is:
(Delhi PG-2005, DNB-2007)
-
p53
-
Ras
-
Myc
-
Bcl-2
29. Apoptosis is associated with all of the following features except:
(Karnataka 2009)
-
Cell shrinkage
-
Intact cellular contents
-
Inflammation
-
Nucleosome size fragmentation of nucleus
30. Liquefactive necrosis is typically seen in
(Karnataka 2006)
-
Ischemic necrosis of the heart
-
Ischemic necrosis of the brain
-
Ischemic necrosis of the intestine
-
Tuberculosis
31. All of the following are morphological features of apoptosis except
(Karnataka 2004)
-
Cell shrinkage
-
Chromatin condensation
-
Inflammation
-
Apoptotic bodies
32. Coagulative necrosis as a primary event is most often seen in all except:
(AP 2002)
-
Kidneys
-
CNS
-
Spleen
-
Liver
33. Liquefactive necrosis is seen in:
-
Heart
-
Brain
-
Lung
-
Spleen
34. Irreversible injury in cell is
(UP 2000)
-
Deposition of Ca++ in mitochondria
-
Swelling
-
Mitotic figure
-
Ribosomal detachment
35. Apoptosis is
(UP-98, 2004)
36. Pyogenic infection and brain infarction are associated with
(UP 2008)
-
Coagulative necrosis
-
Liquefactive necrosis
-
Caseous necrosis
-
Fat necrosis
37. In apoptosis initiation:
(UP 2008)
-
The death receptors induce apoptosis when it engaged by fas ligand system
-
Cytochrome C binds to a protein Apoptosis Activating (Apaf-1) Factor – 1
-
Apoptosis may be initiated by caspase activation
-
Apoptosis mediated through DNA damage
38. Apoptosis is alternatively called as
(RJ 2005)
-
Ischemic cell death
-
Programmed cell death
-
Post traumtic cell death
-
All
39. First cellular change in hypoxia:
(Kolkata 2003)
-
Decreased oxidative phosphorylation in mitochondria
-
Cellular swelling
-
Alteration in cellular membrane permeability
-
Clumping of nuclear chromatin
40. About apoptosis, true statement is:
(Bihar 2003)
-
Injury due to hypoxia
-
Inflammatory reaction is present
-
Councilman bodies is associated with apoptosis
-
Cell membrane is damaged
41. Fournier's gangrene is seen in:
(Jharkhand 2006)
-
Nose
-
Scrotal skin
-
Oral cavity
-
All are true
42. Coagulative necrosis is seen in:
(Jharkhand 2006)
-
Brain
-
Breast
-
Liver
-
All
43. A patient Fahim presents to the hospital with jaundice, right upper quadrant pain and fatigue. He tests positive for hepatitis B surface antigen. The serum bilirubin levels is 4.8mg/dl (direct is 0.8mg/dl and indirect bilirubin is 4.0mg/dl), AST levels is 300 U/L, ALT is 325 U/L and alkaline phosphatase is within normal limits. The elevation in AST and ALT can be explained by which of the following?
-
Bleb formation
-
Cell membrane rupture
-
Clumping of nuclear chromatin
-
Swelling of endoplasmic reticulum
44. A 23-year-old lady Sweety was driving her car when she had to apply brakes suddenly. She suffered from “steering wheel” injury in the right breast. After 5 days of pain and tenderness at the site of trauma, she noticed the presence “lump” which was persistent since the day of trauma. Dr. M. Spartan does an excision biopsy and observed the presence of an amorphous basophilic material within the mass. The amorphous material is an example of
-
Apocrine metaplasia.
-
Dystrophic fat necrosis
-
Enzymatic fat necrosis
-
Granulomatous inflammation
45. A patient Subbu is diagnosed with a cancer. It was observed that he shows a poor response to a commonly used anti-cancer drug which acts by increasing programmed cell death. Inactivation of which of the following molecules/genes is responsible for the resistance shown in the tumor cells?
-
Granzyme and perforin
-
Bcl-2
-
p53
-
Cytochrome P450
46. Dr Maalu Gupta is carrying out an experiment in which a genetic mutation decreased the cell survival of a cell culture line. These cells have clumping of the nuclear chromatin and reduced size as compared to normal cells. Which of the following is the most likely involved gene in the above described situation?
-
Fas
-
Bax
-
Bcl-2
-
Myc
47-49. …Read the following statement for questions 49, 50 and 51 carefully and answer the associated questions.
A 50-year old male Braj Singh presented to the medicine emergency room with retrosternal chest pain of 15 minutes duration. He also had sweating and mild dyspnea. The physician immediately gave him a nitrate tablet to be kept sublingually following which his chest pain decreased significantly.
47. Which of the following best represents the biochemical change in the myocardial cells of this patient during the transient hypoxia?
-
Decreased hydrogen ion concentration
-
Increase in oxidative phosphorylation
-
Loss of intracellular Na+ and water
-
Stimulation of anaerobic glycolysis and glycogenolysis
48. Which of the following if accumulated is suggestive of reversible cell injury due to hypoperfusion of different organs during this duration of myocardial ischemia?
49. If we presume that the patient has experienced several similar episodes of pain over the last 10 hours, which of the following ultra-structural changes would most likely indicate irreversible myocardial cell injury in this patient?
-
Myofibril relaxation
-
Disaggregation of polysomes
-
Mitochondrial vacuolization
-
Disaggregation of nuclear granules
50. A 55-year-old man, Vikas develops a thrombus in his left anterior descending coronary artery. The area of myocardium supplied by this vessel is irreversibly injured. The thrombus is destroyed by the infusion of streptokinase, which is a plasminogen activator, and the injured area is reperfused. The patient, however, develops an arrhythmia and dies. An electron microscopic (EM) picture taken of the irreversibly injured myocardium reveals the presence of large, dark, irregular amorphic densities within mitochondria. What are these abnormal structures?
-
Apoptotic bodies
-
Flocculent densities
-
Myelin figures
-
Psammoma bodies
-
Russell bodies
51. Which one of the listed statements best describes the mechanism through which Fas(CD95) initiates apoptosis?
-
BCL2 product blocks channels
-
Cytochrome activates Apaf-1
-
FADD stimulates caspase 8
-
TNF inhibits Ikb
-
TRADD stimulates FAD
53. Psammoma bodies are seen in all
except:
(AI 2011,09)
-
Follicular carcinoma of thyroid
-
Papillary carcinoma of thyroid
-
Serous cystadenoma of ovary
-
Meningioma
54. True about metastatic calcification is
(AIIMS May 2009)
-
Calcium level is normal
-
Occur in dead and dying tissue
-
Occur in damaged heart valve
-
Mitochondria involved earliest
55. Both hyperplasia and hypertrophy are seen in?
(AIIMS May 2009)
-
Breast enlargement during lactation
-
Uterus during pregnancy
-
Skeletal muscle enlargement during exercise
-
Left ventricular hypertrophy during heart failure
56. Which of the following is not a common site for metastatic calcification?
(AIIMS Nov 2005)
-
Gastric mucosa
-
Kidney
-
Parathyroid
-
Lung
57. Calcification of soft tissues without any disturbance of calcium metabolism is called
(AIIMS Nov 2004)
-
Inotrophic calcification
-
Monotrophic calcification
-
Dystrophic calcification
-
Calcium induced calcification
58. The light brown perinuclear pigment seen on H & E staining of the cardiac muscle fibres in the grossly normal appearing heart of an 83 year old man at autopsy is due to deposition as:
(AIIMS May 2003)
-
Hemosiderin
-
Lipochrome
-
Cholesterol metabolite
-
Anthracotic pigment
59. Dystrophic calcification is seen in:
(AIIMS Nov 2002)
-
Rickets
-
Hyperparathyroidism
-
Atheromatous plaque
-
Vitamin A intoxication
60. The Fenton reaction leads to free radical generation when:
(AIIMS Nov 2002)
-
Radiant energy is absorbed by water
-
Hydrogen peroxide is formed by Myeloperoxidase
-
Ferrous ions are converted to ferric ions
-
Nitric oxide is converted to peroxynitrite anion
61. Mallory hyaline is seen in:
(PGI Dec 2000)
-
Alcoholic liver disease
-
Hepatocellular carcinoma
-
Wilson's disease
-
I.C.C. (Indian childhood cirrhosis)
-
Biliary cirrhosis
62. Heterotopic calcification occurs in:
(PGI Dec 2000)
-
Ankylosing spondylitis
-
Reiter's syndrome
-
Forrestier's disease
-
Rheumatoid arthritis
-
Gouty arthritis
63. Pigmentation in the liver is caused by all except:
(PGI Dec 01)
-
Lipofuscin
-
Pseudomelanin
-
Wilson's disease
-
Malarial pigment
-
Bile pigment
64. Wear and tear pigment in the body refers to
(Karnataka 2006)
-
Lipochrome
-
Melanin
-
Anthracotic pigment
-
Hemosiderin
65. Mallory hyaline bodies are seen all Except:
(AI 97) (UP 2004)
-
Indian childhood cirrhosis
-
Wilson's disease
-
Alcoholic hepatitis
-
Crigler-Najjar syndrome
66. “Russell's body” are accumulations of:
(UP 2006)
-
Cholesterol
-
Immunoglobulins
-
Lipoproteins
-
Phospholipids
67. Dystrophic calcification is seen in:
(UP 2006)
-
Atheroma
-
Paget's disease
-
Renal osteodystrophy
-
Milk-alkali syndrome
68. Brown atrophy is due to
(AP 2000)
-
Fatty necrosis
-
Hemosiderin
-
Lipofuscin
-
Ceruloplasmin
69. Psammoma bodies are typically associated with all of the following neoplasms except
(AP 2001)
-
Medulloblastoma
-
Meningioma
-
Papillary carcinoma of the thyroid
-
Papillary serous cystadenocarcinoma of the ovary
70. Transformation of one epithelium to other epithelium is known as
(AP 2001)
-
Dysplasia
-
Hyperplasia
-
Neoplasia
-
Metaplasia
71. All are true about metaplasia except
(AP 2004)
(AIIMS 1996, UP 2002)
-
Slow growth
-
Reverse back to normal with appropriate treatment
-
Irreversible
-
If persistent may induce cancer transformation
72. About hyperplasia, which of the following statement is false?
(AP 2007)
73. Example of hypertrophy is:
(Kolkata 2004)
-
Breast in puberty
-
Uterus during pregnancy
-
Ovary after menopause
-
Liver after resection
74. Metastatic calcification occurs in all except:
(Bihar 2005)
-
Kidney
-
Atheroma
-
Fundus of stomach
-
Pulmonary veins
75. Dystrophic calcification is:
(Jharkhand 2006)
-
Calcification in dead tissue
-
Calcification in living tissue
-
Calcification in dead man
-
None
76. An old man Muthoot has difficulty in urination associated with increased urge and frequency. He has to get up several times in night to relieve himself. There is no history of any burning micturition and lower back pain. On rectal examination, he has enlarged prostate. Which of the following represents the most likely change in the bladder of this patient?
-
Hyperplasia
-
Atrophy
-
Hypertrophy
-
Metaplasia
77. An increase in the size of a cell in response to stress is called as hypertrophy. Which of the following does not represent the example of smooth muscle hypertrophy as an adaptive response to the relevant situation?
-
Urinary bladder in urine outflow obstruction
-
Small intestine in intestinal obstruction
-
Triceps in body builders
-
None of the above
78. A patient Ramu Kaka presented with complaints of slow progressive breathlessness, redness in the eyes and skin lesions. His chest X ray had bilateral hilar lymphadenopathy. His serum ACE levels were elevated. On doing Kveim test, it came out to be positive. Final confirmation was done with a biopsy which demonstrated presence of non-caseous granuloma. A diagnosis of sarcoidosis was established. Which of the following statements regarding calcification and sarcoidosis is not true?
-
The calcification in sarcoidosis begins at a cellular level in mitochondria
-
There is presence of dystrophic calcification
-
The granulomatous lesions contain macrophages which cause activation of vitamin D precursors
-
None of the above
79. A 50-year-old male alcoholic, Rajesh presents with symptoms of liver disease and is found to have mildly elevated liver enzymes. A liver biopsy examined with a routine hematoxylin and eosin (H & E) stain reveals abnormal clear spaces in the cytoplasm of most of the hepatocytes. Which of the following materials is most likely forming cytoplasm spaces?
-
Calcium
-
Cholesterol
-
Hemosiderin
-
Lipofuscin
-
Triglyceride
80. A 36-year-old woman, Geeta presents with intermittent pelvic pain. Physical examination reveals a 3-cm mass in the area of her right ovary. Histologic sections from this ovarian mass reveal a papillary tumor with multiple, scattered small, round, laminated calcifications. Which of the following is the basic defect producing these abnormal structures?
-
Bacterial infection
-
Dystrophic calcification
-
Enzymatic necrosis
-
Metastatic calcification
-
Viral infection
81. A 28-year-old male executive presents to the doctor with complaints of “heartburn” non responsive to usual medicines undergoes endoscopy with biopsy of the distal esophagus is taken. What type of mucosa is normal for the distal esophagus?
-
Ciliated, columnar epithelium
-
Keratinized, stratified, squamous epithelium
-
Non-keratinized, simple, squamous epitheliu
-
Non-keratinized, stratified, squamous epithelium
83. Which of the following is the most common fixative used in electron microscopy?
(AIIMS Nov 2012)
-
Glutaraldehyde
-
Formalin
-
Picric acid
-
Absolute Alcohol
84. The fixative used in histopathology:
(AIIMS May 2012)
-
10% buffered neutral formalin
-
Bouins fixative
-
Glutaraldehyde
-
Ethyl alcohol
85. Which is the most commonly used fixative in histopathological specimens?
(AI 2011)
-
Glutaraldehyde
-
Formaldehyde
-
Alcohol
-
Picric acid
86. Lipid in the tissue is detected by:
(AIIMS Nov 2009)
-
PAS
-
Myeloperoxidase
-
Oil Red O
-
Mucicarmine
87. The most abundant glycoprotein present in basement membrane is:
(AI 2004)
-
Laminin
-
Fibronectin
-
Collagen type 4
-
Heparan sulphate
88. Enzyme that protects the brain from free radical injury is:
(AI 2001)
-
Myeloperoxidase
-
Superoxide dismutase
-
MAO
-
Hydroxylase
89. Increased incidence of cancer in old age is due to
(AIIMS May 2009)
-
Telomerase reactivation
-
Telomerase deactivation
-
Inactivation of protooncogene
-
Increase in apoptosis
90. Stain not used for lipid
(AIIMS Nov 2007)
-
Oil red O
-
Congo red
-
Sudan III
-
Sudan black
91. Acridine orange is a fluorescent dye used to bind
(AIIMS Nov 2007)
-
DNA and RNA
-
Protein
-
Lipid
-
Carbohydrates
92. PAS stains the following except
(AIIMS Nov 2007)
-
Glycogen
-
Lipids
-
Fungal cell wall
-
Basement membrane of bacteria
93. All are components of basement membrane except
(AIIMS Nov 2007)
-
Nidogen
-
Laminin
-
Entactin
-
Rhodopsin
94. Which of the following pigments are involved in free radical injury?
(AIIMS Nov 2006)
-
Lipofuscin
-
Melanin
-
Bilirubin
-
Hematin
95. True about cell ageing:
(AIIMS Nov 2001)
-
Free radicals injury
-
Mitochondria are increased
-
Lipofuscin accumulation in the cell
-
Size of cell increased
96. Neutrophil secretes:
(PGI Dec 2002)
-
Superoxide dismutase
-
Myeloperoxidase
-
Lysosomal enzyme
-
Catalase
-
Cathepsin G
97. Which of the following is a peroxisomal free radical scavenger?
(Delhi PG 2006)
-
Superoxide dismutase
-
Glutathione peroxidase
-
Catalase
-
All of the above
98. Crooke's hyaline body is present in:
(Kolkata 2001)
-
Yellow fever
-
Basophil cells of the pituitary gland in Cushing's syndrome
-
Parkinsonism
99. An autopsy is performed on a 65-year-old man, Suresh who died of congestive heart failure. Sections of the
liver reveal yellow-brown granules in the cytoplasm of most of the hepatocytes. Which of the following stains would be most useful to demonstrate with positive staining that these yellow-brown cytoplasmic granules are in fact composed of hemosiderin (iron)?
-
Oil red O stain
-
Oil red O stain
-
Periodic acid-Schiff stain
-
Prussian blue stain
-
Sudan black B stain
-
Trichrome stain
100. An AIDS patient Khalil develops symptoms of pneumonia, and Pneumocystis carinii is suspected as the causative organism. Bronchial lavage is performed. Which of the following stains would be most helpful in demonstrating the organism's cysts on slides made from the lavage fluid?
-
Alcian blue
-
Hematoxylin and eosin
-
Methenamine silver
-
Trichrome stain
101. Which process makes the bacteria ‘tasty’ to the macrophages:
(Kolkata 2008)
-
Margination
-
Diapedesis
-
Opsonisation
-
Chemotaxis
102. In an evaluation of a 7-year-old boy, Ram who has had recurrent infections since the first year of life, findings include enlargement of the liver and spleen, lymph node inflammation, and a superficial dermatitis resembling eczema. Microscopic examination of a series of peripheral blood smears taken during the course of a staphylococcal infection indicates that the bactericidal capacity of the boy's neutrophils is impaired or absent. Which of the following is the most likely cause of this child's illness?
-
Defect in the enzyme NADPH oxidase
-
Defect in the enzyme adenosine deaminase (ADA)
-
Defect in the IL-2 receptor
-
Developmental defect at the pre-B stage
-
Developmental failure of pharyngeal pouches 3 and 4
EXPLANATIONS
In the activation of Extrinsic pathway of apoptosis,
binding of Fas ligand takes place to CD95 (Fas; member of TNF receptor family) or binding of TRAIL (TNF related apoptosis inducing ligand) attaches to death receptors DR4 and DR5. This induces the association of FADD (Fas- associated death domain) and procaspase-8 to death domain motifs of the receptors resulting in activation of caspase 8 (in humans caspase 10) which finally activates caspases- 3 and 7 that are final effector caspases
2.
Ans. (b) Amorphous densities in mitochondria
(Ref: Robbins 8/e p14-19, 9/e p42,50)
Two phenomena consistently characterize irreversibility:
-
The first is the inability to reverse mitochondrial dysfunction (lack of oxidative phosphorylation and ATP generation) even after resolution of the original injury.
-
The second is the development of profound disturbances in membrane function
So, the answer for the given question is ‘Amorphous densities in mitochondria’.
However, please remember friends that the Robbins in its 8th edition pg 14 mentions small amorphous densities to be present in reversible cell injury also. Therefore, the best answer for characterizing irreversibility of an injury is ‘profound disturbances in membrane function’.
3.
Ans. (c) Embryogenesis
(Ref: Robbins 8/e p25, 9/e p52)
Caspases are cysteine proteases and are critical for the process of apoptosis. Physiologically, apoptosis is required to eliminate the cells no longer required and to maintain a steady number of various cell populations in tissues. The programmed cell death (apoptosis) is required at the time of different processes in embryogenesis like implantation, organogenesis, developmental involution and metamorphosis.
4.
Ans. (b) Apoptosis
(Ref: Robbins 8/e p27, 9/e p53)
5.
Ans. (d) Condensation of the nucleus
(Ref: Robbins 8/e p14-15, 26-27, 9/e p53)
The morphologic features characteristic of apoptosis includes
- Cell shrinkage: The cell is smaller in size having dense cytoplasm and the organelles are tightly packed.
- Chromatin condensation: This is the most characteristic feature of apoptosis.
- Formation of cytoplasmic blebs and apoptotic bodies
Regarding option ‘a’…’Plasma membranes are thought to remain intact till late stage of apoptosis, as well as is a normal cell.
Regarding option “b”, eosinophilic cytoplasm, it is a common feature of necrosis and apoptosis.
6.
Ans. (a) TB > (c) Gangrene
(Ref: Robbins 8/e p16, 9/e p43)
In the 7th edition of Robbins it was clearly stated that…“Caseous necrosis, a distinctive form of coagulative necrosis, is encountered most often in foci of tuberculous infection. The term caseous is derived from the cheesy white gross appearance of the area of necrosis.”
Regarding the option gangrene, it is not specified the type of gangrene and therefore, we go with the better option as tuberculosis in the given question. Moreover, according to Robbins, gangrenous necrosis is not a specific pattern of necrosis but is a term used in clinical practice.
7.
Ans. (c) Mitochondria
(Ref: Robbins 8/e p28, Harrison 18/e p681, 9/e p53)
8.
Ans. (a) Formation of Amorphous densities in mitochondrial matrix
(Ref: Robbins 7/e p19, 9/e p42)
Formation of amorphous densities in the mitochondrial matrix is a feature of irreversible injury and not reversible injury.
- Decreased formation of ATP constitutes the critical mechanism of cell injury and occurs in both reversible as well as irreversible cell injury.
Features of Reversible cell injury
|
Features of irreversible cell injury
|
|---|---|
|
|
9.
Ans. (c) Diabetic glomerulosclerosis
(Ref: Robbins 7/e p214, 594, 1008, 9/e p44)
Fibrinoid necrosis is a distinctive morphological pattern of cell injury characterized by deposition of fibrin like proteinaceous material in walls of arteries. Areas of fibrinoid necrosis appear as smudgy eosinophilic regions with obscured underlying cellular details.
Fibrinoid necrosis is seen in
- Malignant hypertension
- Vasculitis like PAN
- Acute Rheumatic Fever.
10.
Ans. (d) Cytochrome C
(Ref: Robbins 7/e p30; Harrison 17/e p506, 9/e p55)
Apoptosis or programmed cell death can be induced by intrinsic or extrinsic pathway. As can be seen in the intrinsic pathway; cyt c gets associated with APAF-1 which activates caspase and cause cell death. For detail see text.
11.
Ans. (c) bcl – 2
(Ref: Robbins 7/e p29-30, Harrison 17/e p506)
12.
Ans. (a) Apoptosis
(Ref: Robbins 8/e p27, 9/e p56)
Apoptotic cells express phosphatidylserine in the outer layers of their plasma membranes. This phospholipid moves out from the inner layers where it is recognized by a number of receptors on the phagocytes. These lipids are also detected by binding of a protein called Annexin V. So, Annexin V staining is used to identify the apoptotic cells.
13.
Ans. (b) Amorphous densities in mitochondria
(Ref: Robbins 7/e p12, 9/e p42)
See earlier explanation.
14.
Ans. (b) Apoptosis
(Ref: Robbins 7/e p28, 9/e p53)
Caspases are present in normal cells as inactive proenzymes and when they are activated they cleave proteins and induce apoptosis. These are cysteine proteases.
15.
Ans. (a) Inflammation is present
(Ref: Robbins 7/e p31, 27, 9/e p56)
In Apoptosis the dead cell is rapidly cleared, before its contents have leaked out, and therefore cell death by this pathway does not elicit an inflammatory reactionQ in the host.
16.
Ans. (c) Bcl-X
(Ref: Robbins 7/e p29, 9/e p55)
17.
Ans. (a) Apoptosis
(Ref: Robbins 7/e p26, 9/e p55)
18.
Ans. (a) Amorphous densities in mitochondria
(Ref: Robbin's 7/e p12, 9/e p50)
Two phenomenon's consistently characterize irreversible cell injury:
-
Large amorphous densities in the mitochondria (this indicates inability to reverse mitochondrial dysfunction)
-
Development of profound disturbance in membrane function
19.
Ans. (d) Apoptosis
(Ref: Robbin's 7/e p27; Robbins 8/e p27, 9/e p52)
The inter-nucleosomal cleavage of DNA into oligonucleosomes (in multiples of 180-200 base pairs) is brought about by Ca2+ and Mg2+ dependent endonucleases and is characteristic of apoptosis.
20.
Ans. (b) Apoptosis
(Ref: Robbins 7/e p26, 27, 9/e p52)
21.
Ans. (a) Endonuclease
(Ref: Robbins 7/e p26, 27, 28; 8/e pg28)
-
Endonucleases are enzymes which cause internucleosomal cleavage of DNA into oligonucleosomes, the latter being visualized by agarose gel electrophoresisas DNA ladders.
-
In necrosis, smeared pattern is commonly seen
23.
Ans. (c) Apoptosis of cells induce inflammatory reaction
(Ref: Robbins 7/e p27, 9/e p56)
Remember important features of apoptosis
24.
Ans. (a) Cytoplasmic blebs; (c) Nuclear Fragmentation:
(Ref: Robbins 7/e p26, 9/e p53)
Apoptosis is a programmed cell death.
During apoptosis, cells destined to die activate enzymes that degrade the cell's own nuclear DNA and nuclear and cytoplasmic proteins. There is no inflammatory reaction elicited by host.
- Spindle formation is found in cell division in mitosis.
- During necrosis, cell swelling is seen.
Differences between apoptosis and necrosis
| ||
|---|---|---|
Feature
|
Necrosis
|
Apoptosis
|
Cell size | Enlarged (swollen) | Reduced (shrink) |
Nucleus | Pyknosis/Karyorrhexis/Karyolysis | Fragmentation into nucleosome-sized fragments |
Plasma membrane | Disrupted | Intact; altered structure, especially orientation of lipids |
Cellular contents | Enzymatic digestion; may leak out of cell | Intact; may be released in apoptotic bodies |
Adjacent inflammation | Frequent | No |
Role in body | Invariably pathologic (culmination of irreversible cell injury) | Often physiologic. May be pathologic after cell injury as DNA damage. |
Proapoptotic | Bak; Bax; Bim; P53 gene; Caspases TNFRI; Fas [CD95]; FADD (Fas associated death domain) | |
Anti-apoptotic | Bcl-2/bcl-X; FLIP; Apaf-1 (Apoptosis activating factor-1) Cytochrome C | |
25.
Ans. (b) End products are phagocytosed by macrophage; (c) Intranuclear fragmentation of DNA; (d) Activation of caspases; (e) Annexin V is a marker of apoptotic cell
(Ref: Harsh Mohan 5th/53, Robbins 7/e p25-3l, 9/e p53)
26.
Ans. (a) Apoptosis
(Ref: Robbins 8/e p25, 9/e p52)
27.
Ans. (c) Bcl-2
(Ref: Robbins 7/e p31, 32)
Inhibitors of apoptosis:
|
Promoters of apoptosis:
|
Sensors of apoptosis:
|
|---|---|---|
Bcl-2 Bcl-XL | Bax BAK P-53 activation Ischemic injury Death of virus infected cells Neurodegenerative diseases | Bad Bim Bid Noxa Puma |
28.
Ans. (d) Bcl-2
(Ref: Robbins 7/e p29, 31, 32, 9/e p55)
29.
Ans. (c) Inflammation
(Ref: Robbins 7/e p26, 9/e p53)
30.
Ans. (b) Ischemic necrosis of the brain
(Ref: Robbins 7/e p21-22, 9/e p43)
31.
Ans. (c) Inflammation
(Ref: Robbin 7/e p27, 9/e p56)
32.
Ans. (b) CNS
(Ref: Robbins 8/e p15, 7/e p22, 9/e p43)
33.
Ans. (b) Brain
(Ref: Robbins 8/e p15, 7/e p22, 9/e p43)
34.
Ans. (a) Deposition of Ca++ in mitochondria
(Ref: Robbins 8/e p13-14; 7/e p11, 9/e p47)
35.
Ans. (b) Type of cell injury
(Ref: Robbins 8/e p25; 7/e p26-28, 9/e p52)
37.
Ans. (a) The death receptors induce apoptosis when it engaged by
fas
ligand system
(Ref: Robbins 8/e p29; 7/e p30, 9/e p56)
38.
Ans. (b) Programmed cell death
(Ref: Robbins 8/e p25, 9/e p52)
39.
Ans. (a) Decreased oxidative phosphorylation in mitochondria
(Ref: Robbins 8/e p18-19, 7/e p15, 9/e p45)
40.
Ans. (c) Councilman bodies is a type of apoptosis
(Ref: Robbins 8/e p25; 7/e 26, 9/e p823)
41.
Ans. (b) Scrotal skin
42.
Ans. (c) Liver
(Ref: Robbins 7/e p21, 8/e p15; 9/e p43)
43.
Ans. (b) Cell membrane rupture
(Ref: Robbins 8/e p23, 9/e p49-50)
The symptoms and the medical reports of the patient are suggestive of liver cell injury. Out of the options provided, rupture of the cell membrane is the only cellular change suggestive of irreversible cell injury. All others may be seen in reversible cell injury as well.
44.
Ans. (b) Dystrophic fat necrosis
(Ref: Robbins 8/e p16-17, 9/e p65)
The situation described above is a typical description of a traumatic fat necrosis. This condition needs to be distinguished from enzymatic fat necrosis. The hint is in the stem of the question which describes the presence of amorphous basophilic material. This is suggestive of calcification and such pattern of calcification of previous damaged tissue is termed dystrophic calcification.
45.
Ans. (c) p53
(Ref: Robbins 8/e p30,292, 9/e p53-55)
When anti-cancer drugs are administered, they induce the death of the tumor cells by activating p53 gene and increasing apoptosis. Tumor cells may show resistance to these drugs if there is a mutation in the p53 gene thereby preventing apoptosis. Bcl-2 promotes the cell growth by inhibiting apoptosis. Granzyme and perforin also increase apoptosis but in case of cytotoxic T cells. Cytochrome P450 is not associated with apoptosis.
46.
Ans. (c) Bcl-2
(Ref: Robbins 8/e p28, 9/e p55)
The process being described in the stem of the question is apoptosis. Fas and Bax are genes which promote apoptosis. Bcl-2 is inhibitory for apoptosis. So, a Bcl-2 mutation is associated with an increase in apoptosis. Myc is involved in development of cancer and not directly associated with apoptosis.
47.
Ans. (d) Stimulation of anaerobic glycolysis and glycogenolysis
(Ref: Robbins 8/e p18, 9/e p46)
The hypoxic cell damage results in decrease in oxidative phosphorylation followed by ATP depletion and increase in AMP and ADP. Increased phosphofructokinase and phosphorylase activities respectively stimulate anaerobic glycolysis and glycogenolysis. This results in decrease in intracellular pH and depletion of cellular glycogen stores. Decrease availability of ATP also results in failure of the Na+ -K+- ATPase pump, which then leads to increased cell Na+ and water and decreased cell K+.
48.
Ans. (c) Lactic acid
(Ref: Robbins 8/e p18, 9/e p45)
Anaerobic glycolysis results in accumulation of cellular lactic acid in almost every organ having reduced perfusion. Lactate accumulation also causes reduced pH. Carbon dioxide and creatinine would increase in involvement of the lung and the kidneys respectively. But these are not common for every organ involvement.
49.
Ans. (c) Mitochondrial vacuolization
(Ref: Robbins 8/e p19, 9/e p46)
The appearance of vacuoles and phospholipid-containing amorphous densities within mitochondria generally signifies irreversible injury, and implies a permanent inability to generate further ATP via oxidative phosphorylation. When the mitochondria are injured irreversibly, the cell cannot recover.
-
Irreversible cellular injury is characterized by severe damage to mitochondria (vacuole formation), extensive damage to plasma membranes and nuclei, and rupture of lysosomes.
-
Severe damage to mitochondria is characterized by the influx of calcium ions into the mitochondria and the subsequent formation of large, flocculent densities within the mitochondria. These flocculent densities are characteristically seen in irreversibly injured myocardial cells that undergo reperfusion soon after injury.
51.
Ans. (c) i.e. FADD stimulates caspase – 8
(Ref: Robbins 7/e p26-32, , 9/e p56)
-
Apoptosis has two basic phases: an initiation phase, during which caspases are activated, and an execution phase, during which cell death occurs.
-
The initiation phase has two distinct pathways: the extrinsic (receptor mediated) pathway and the intrinsic (or mitochondrial) pathway.
-
The extrinsic pathway is mediated by cell surface death receptors, two example of death receptors are type I TNF receptor (TNFR1) and Fas (CD95).
-
Fas ligand (FasL), which is produced by immune cells, stimulates apoptosis by binding to Fas, which activates the cytoplasmic Fas-associated death domain protein (FADD), which in turn activates the caspase cascade via the activation of caspase 8.
-
In contrast to the extrinsic pathway, the intrinsic pathway does not involve death receptors and instead results from increased permeability of mitochondria.
52.1.
Ans. (a) Apaf 1
(Ref: Robbins 8/e p29, 9/e p55)
On being released in the cytosol,cytochromecbinds to a protein called Apaf-1 (apoptosis-activating factor-1 which is responsible for formation of a complex called apoptosome. This complex binds to caspase-9 which is a critical initiator caspase of the mitochondrial pathway of apoptosis.
NEET POINTS about APOPTOSIS
|
|
|
|
|
|
52.2.
Ans. (b) Neurons
(Ref: Robbins 8/e p11-2)
-
The neurons are the most sensitive cells in the body to get injured because of hypoxia.
-
So, Purkinje cells of the cerebellum and neurons of the hippocampus are the most susceptible cells which get affected in hypoxic ischemic encephalopathy.
52.3.
Ans. (b) Cell membrane
(Ref: Robbins 8/e p23, 9/e p50-51)
Dead cells may be replaced by large, whorled phospholipid masses called myelin figures that are derived from damaged cell membranes. These phospholipid precipitates are then either phagocytosed by other cells or further degraded into fatty acids.
52.4.
Ans. (a) Mitochondrial densities
(Ref: Robbins 8/e p23-4, 9/e p50)
The two key features of irreversible injury are:
- Inability to reverse mitochondrial dysfunctionQ and
- Development of profound disturbances in the membrane functionQ.
52.5.
Ans. (b) CNS
(Ref: Robbins 8/e p15, 7/e p22, 9/e p43)
As discussed in text, central nervous system is characterized by the presence of liquefactive necrosisQ during ischemic injury.
52.6.
Ans. (b) Brain
(Ref: Robbins 8/e p15, 7/e p22, 9/e p43)
As discussed earlier, CNS shows liquefactive necrosis.
52.7.
Ans. (c) Mitochondria
(Ref: Robbins 8/e p28, 7/e p29, 9/e p15, 53)
Mitochondrion must be recognized not only as an organelle with vital roles in intermediary metabolism and oxidative phosphorylation, but also as a central regulatory structure of apoptosis.
52.8.
Ans. (a) Mitochondria
(Ref: Robbins 8/e p19, 9/e p65-66)
Direct quote.. “Initiation of intracellular calcification occurs in the mitochondria of dead or dying cells that accumulate calcium”.
Glucocorticoids induce apoptosis while sex steroids inhibit apoptosis… Underwood Pathology
Inducers of apoptosis
|
Inhibitors of apoptosis
|
|---|---|
|
|
52.10.
Ans. (c) Inflammation
(Ref: Robbin 8/e p26-7)
Inflammation is not seen in apoptosis.
Chromatin condensation is the most characteristic feature of apoptosis. Other findings like cell membrane shrinkage and DNA fragmentation are also associated with apoptosis.
52.11.
Ans (a) Bcl-2
(Ref: Robbin 9th/ 8thed: pg606)
We need to identify a gene which should be able to inhibit apoptosis. The answer therefore is bcl-2. It is seen to result in the development of follicular lymphoma.
52.12.
Ans (b) Both may be pathological
(Ref: Robbin 9th/40)
53.
Ans. (a) Follicular carcinoma of Thyroid
(Ref: Robbins 8/e p38, 9/e p65)
Tumors (MOST for PG)
-
M – Meningioma
-
O – Papillary carcinoma of Ovary (serous ovarian cystadenoma)
-
S – Papillary carcinoma of Salivary gland
-
T – Papillary carcinoma of Thyroid
-
Prolactinoma, Papillary type of renal cell carcinoma
-
Glucagonoma
(Psammoma bodies are seen in papillary thyroid cancer and not follicular thyroid cancer)
54.
Ans. (d) Mitochondria involved earliest
(Ref: Robbins 8/e p38, Robbins 7/e p41-42, 9/e p65)
-
When the calcium deposition occurs locally in dying tissues despite normal serum levels of calcium, it is known as dystrophic calcification. It is seen in atherosclerosis, tuberculous lymph node and aging or damaged heart valves.
-
The deposition of calcium salts in otherwise normal tissues almost always results from hypercalcemia and is known as metastatic calcification.
Friends, Robbins 7th edn page 41-42 mentions that initiation of intracellular calcification occurs in the mitochondria of dead or dying cells that accumulate calcium. Nothing is mentioned regarding the involvement of mitochondria in metastatic calcification in either 8th or 7th edition of Robbins. However, we got an article on Medscape which states that “Within the cell it is the mitochondria that serves as the nidus for metastatic calcification”.
55.
Ans. (b) Uterus during pregnancy
(Ref: Robbins 8/e p6-8, 9/e p36)
-
Hypertrophy refers to an increase in the size of cells, resulting in an increase in the size of the organ. The increased size of the cells is due the synthesis of more structural components.
-
The massive physiologic growth of the uterus during pregnancy is a good example of hormone-induced increase in the size of an organ that results from both hypertrophy and hyperplasia
-
Regarding the ‘a’ choice, Breast enlargement during lactation; it is written in Robbins that prolactin and estrogen cause hypertrophy of the breasts during lactation. Hormonal hyperplasia is best exemplified by the proliferation of the glandular epithelium of the female breast at puberty and during pregnancy.
56.
Ans. (c) Parathyroid
(Ref: Robbins 7/e p42, 9/e p65)
-
Metastatic calcification may occur widely throughout the body but principally affects:
-
The common feature of all these sites, which makes them prone to calcification is that can loose acid and therefore they have an internal alkaline component favorable for metastatic calcification.
-
Often a cause of organ dysfunction.
57.
Ans. (c) Dystrophic calcification
(Ref: Robbins 7/e p41, 8/e p38, 9/e p65)
58.
Ans. (b) Lipochrome
(Ref: Robbins 7/e p39, 9/e p64)
Regarding other options
-
Hemosiderin: It is a pigment deposited in conditions of excess iron.
-
Anthracotic pigment: It is pigment seen in the lung of coal
59.
Ans. (c) Atheromatous plaque
(Ref: Robbins 7/e p41, 9/e p65)
-
Atheromatous plaque would have dead cells, so, there is presence of dystrophic calcification.
-
Mnemonic: D for Dead and D for Dystrophic.
60.
Ans. (c) Ferrous ions are converted to ferric ions
(Ref: Robbins’ 7/e p16, 9/e p48)
-
Free radicals are generated through Fenton's reaction which is (H2O2+ Fe2+→ Fe3++ OH++ OH–)
-
In this reaction iron is converted from its ferrous to ferric form and a radical is generated.
-
The other options are also examples of free radical injury but the questions specifically about Fenton reaction.
-
The effects of these reactive species relevant to cell injury include: Lipid peroxidation of membranes, oxidative modification of proteins and lesions in DNA.
61.
Ans. (a) Alcoholic liver disease; (b) Hepatocellular carcinoma; (c) Wilson's disease; (d) I.C.C. (Indian childhood cirrhosis); (e) Biliary cirrhosis
(Ref: Robbins’ 7/e p905)
Mallory bodies: Scattered hepatocytes accumulate tangled skeins of cytokeratin intermediate filaments and other proteins, visible as eosinophilic cytoplasmic inclusions in degenerating hepatocytes. See details in chapter on ‘Liver’.
62.
Ans. (a) Ankylosing spondylitis; (c) Forrestier's disease
(Ref: Robbins’ 7/e p41-2; Harrison17/e p1952)
Pathologic calcification (Heterotopic calcification) is the abnormal tissue deposition of calcium salts together with small amounts of iron, manganese and other mineral salts. It may be of two types: Dystrophic calcification or Metastatic calcification
63.
Ans. None
(Ref: Harsh Mohan 5th/735; Robbins 7/e p39, 910, 914)
Pigmentation in liver is caused by:
-
Lipofuscin: It is an insoluble pigment known as lipochrome and ‘wear and tear’ pigment. It is seen in cells undergoing low, regressive changes and is particularly prominent in liver and heart of ageing patient or patients with severe malnutrition and cancer cachexia.
-
Pseudomelanin: After death, a dark greenish or blackish discoloration of the surface of the abdominal viscera results from the action of sulfated hydrogen upon the iron of disintegrated hemoglobin. Liver is also pigmented.
-
Wilson's disease: Copper is usually deposited in periportal hepatocytes in the form of reddish granules in cytoplasm or reddish cytoplasmic coloration stained by rubeanic acid or rhodamine stain for copper or orcein stain for copper associated protein. Copper also gets deposited in chronic obstructive cholestasis.
-
Malarial pigment: Liver colour varies from dark chocolate red to slate-grey even black depending upon the stage of congestion.
-
In biliary cirrhosis liver is enlarged and greenish-yellow in colour due to cholestasis. So liver is pigmented due to bile.
64.
Ans. (a) Lipochrome
(Ref: Robbins 7/e p39, 9/e p64)
65.
Ans. (d) Crigler-Najjar syndrome
(Ref: Robbins 8/e p858; 7/e p905, Harsh Mohan 6/e p621-622)
66.
Ans. (b) Immunoglobulins
(Ref: Robbins 8/e p610; 7/e p680-681, 9/e p63)
67.
Ans. (a) Atheroma
(Ref: Robbins 8/e p38, 7/e p41-42, 9/e p65)
68.
Ans. (c) Lipofuscin
(Ref: Robbins 8/e p10,532; 7/e 10, 9/e p64)
69.
Ans. (a) Medulloblastoma
(Ref: Robbins 8/e p38, 1122; 7/e 41,1178,1407, 9/e p65)
71.
Ans. (c) Irreversible
(Ref: Robbins 8/e p265; 7/e 10), 9/e p37-38
72.
Ans. (b) ↑ Size of affected cell
(Ref: Robbins 8/e p8-9, 7/e p7 , 9/e p35)
73.
Ans. (b) Uterus during pregnancy
(Ref: Robbins 8/e p6, 7/e p7-8 , 9/e p34-36)
74.
Ans. (b) Atheroma
(Ref: Robbins 8/e p38; 7/e p41, 9/e p65)
75.
Ans. (a) Calcification in dead tissue
(Ref: Robbins 8/e p38, 7/e p41, 9/e p65)
76.
Ans. (c) Hypertrophy
(Ref: Robbins 8/e p6-7, 9/e p36)
The patient is most likely suffering from benign hyperplasia of the prostate. The question however asks about the change in bladder which would be hypertrophy. This is secondary to the obstruction in the urine outflow following the smooth muscle in the bladder undergoes hypertrophy.
77.
Ans. (c) Triceps in body builders
(Ref: Robbins 8/e p6-7, 9/e p34)
The enlargement of the triceps is an example of skeletal muscle hypertrophy (not smooth muscle hypertrophy).
78.
Ans. (b) There is presence of dystrophic calcification
(Ref: Robbins 8/e p38, 9/e p65)
In sarcoidosis, there is presence of metastatic calcification because of the presence of increased concentration of calcitriol (most active form of vitamin D). Both the patterns of calcification begin in mitochondria.
79.
Ans. (e) Triglyceride
(Ref: Robbins 7/e p35-37, 41-42; Chandrasoma, 3/8-10, 9/e p62)
-
Substance that can form clear spaces in the cytoplasm of cells as seen with a routine H&E stain include glycogen, lipid, and water. In the liver, clear spaces within hepatocytes are most likely to be lipid, this change being called fatty change or steatosis.
-
Increased formation of triglycerides can result from alcohol use, as alcohol causes excess NADH formation (high NADH/NAD ratio), increases fatty acid synthesis, and decreases fatty acid oxidation.
-
In contrast to lipid, calcium appears as a dark blue-purple color with routine H&E stains, while hemosiderin, which is formed from the breakdown of ferritin, appears as yellow-brown granules.
-
Lipofuscin also appears as fine, granular, golden –brown intracytoplasmic pigment. It is an insoluble “wear and tear” (ageing) pigment found in neurons, cardiac myocytes, or hepatocytes.
80.
Ans. (b) Dystrophic calcification
(Ref: Robbins 7/e p41-42; Henry/195-196, 9/e p65)
-
Dystrophic calcification is characterized by calcification in abnormal (dystrophic) tissue, while metastatic calcification is characterized by calcification in normal tissue.
-
Examples of dystrophic calcification of damaged or abnormal heart valves, and calcification within tumors
-
Small (microscopic) laminated calcifications within tumors are called Psammoma bodies and are due to single- cell necrosis. Psammoma bodies are characteristically found in papillary tumors, such as papillary carcinomas of the thyroid and papillary tumors of the ovary (especially papillary serous cystadenocarcinoma), but they can also be found in meningiomas or mesotheliomas.
-
With dystrophic calcification the serum calcium levels are normal, while with metastatic calcification the serum calcium levels are elevated (hypercalcemia).
81.
Ans. (d) i.e. Non-keratinized, stratified, squamous epithelium
(Ref: Robbins 8/e p770, 9/e p37)
The esophagus is covered by non-keratinized, stratified, squamous epithelium for its entire length. Heartburn is usually a sign of gastric regurgitation of the acidic contents in the lower esophagus (acid reflux disease).
82.1.
Ans. (d) Seen in teratoma
(Ref: Robbins 8/e p38, 9/e p65)
The progressive acquisition of outer layers may create lamellated configurations, called psammoma bodies because of their resemblance to grains of sand. Some common cancers associated with psammoma bodies are:
-
M – Meningioma, Mesothelioma
-
O – Papillary carcinoma of Ovary (serous ovarian cystadenoma)
-
S – Papillary carcinoma of Salivary gland
-
T – Papillary carcinoma of Thyroid
-
Prolactinoma
-
Glucagonoma
26
82.2.
Ans. (b) Lungs
(Ref: Dail and Hammar's Pulmonary Pathology: Non-neoplastic lung disease, Springer 3/e p777)
Direct quote…‘Lung are the most frequent involved of all organs.’
Ours is the only and the first book to give you an authentic reference for this one friends. This is in sharp contrast to all our competitors who give name and page number of books where this info is just not there. Try that yourself. You would find many such questions and answers in other chapters of this edition. Happy reading!
82.3.
Ans. (d) Plasma cells
(Ref: Robbins 8/e p35, 7/e p37, 9/e p63)
Russell bodies are homogenous eosinophilic inclusions that result from hugely distended endoplasmic reticulum.
82.4.
Ans. (b) Dystrophic
(Ref: Robbins 8/e p38, 7/e p41 , 9/e p65)
Direct quote… “On occasion single necrotic cells may constitute seed crystals that become encrusted by the mineral deposits. The progressive acquisition of outer layers may create lamellated configurations, called psammoma bodies.”
82.5.
Ans. (b) Ca++
(Ref: Harsh Mohan 6/e p106-107, Robbins 7/e p705)
In chronic venous congestion of spleen, some of the hemorrhages overlying fibrous tissue get deposits of hemosiderin and calcium, these are called as Gamma Gandy bodies or siderofibrotic nodules.
82.6.
Ans. (c) Mitochondria
(Ref: Robbins 8/e p35, 7/e p37 , 9/e p53)
Oncocytes are epithelial cells stuffed with mitochondria, which impart the granular appearance to the cytoplasm.
83.
Ans. (a) Glutaraldehyde
(Ref: Bancroft 6/e p53, Ackerman 9th/27)
84.
Ans. (a) 10% buffered neutral formalin
(Ref: Bancroft 6/e p53, Ackerman 9th/27)
-
Commonest fixative used for light microscopic examination: 10% buffered neutral formalin
-
Commonest fixative used for electron microscopic examination: Glutaraldehyde
85.
Ans. (b) Formaldehyde
(Ref: Bancroft 6/e p53)
-
Formaldehyde is the most commonly used fixative in histopathological specimens. See text for details.
86.
Ans. (c) Oil Red O
(Ref: Bancroft histology 6/e p53)
87.
Ans. (a) Laminin
(Ref: Robbins 7/e p105, Harrison 17/e p2462 , 9/e p24)
Laminin is the most abundant glycoprotein in basement membranes. Type IV collagen, laminin and nidogen are present in basement membranes.
88.
Ans. (b) Superoxide dismutase
(Ref: Robbins 7/e p17, Harrison's 17/e p2572 , 9/e p48)
-
Antioxidant enzymes include glutathione peroxidase, SOD and catalase.
-
Deficiency of SOD 1 gene may result in motor neuron disorder. This finding strengthens the view that SOD protects brain from free radial injury.
89.
Ans. (a) Telomerase reactivation
(Ref: Robbins 8/e p296-297 , 9/e p67)
90.
Ans. (b) Congo red
(Ref: Bancroft's histopathology 5th/204)
Congo red is used for staining amyloid and not lipids
Stains for Lipids
|
|
|
|
|
|
-
Acridine orange is a nucleic acid selective fluorescent cationic dye useful for cell cycle determination.
-
It is cell-permeable, and interacts with DNA and RNA by intercalation or electrostatic attractions respectively and emits green and red right respectively.
-
Acridine orange can be used in conjunction with ethidium bromide to differentiate between live and apoptotic cells.
92.
Ans. (b) Lipids
(Ref: Bancroft's histopathology 5th/204)
PAS (periodic acid-Schiff) stain is versatile and has been used to stain many structures including glycogen, mucin, mucoprotein, glycoprotein, as well as fungi. PAS is useful for outlining tissue structures, basement membranes, glomeruli, blood vessels and glycogen in the liver.
93.
Ans. (d) Rhodopsin
(Ref: Robbins 7/e p103, 9/e p24)
Basement membrane is Periodic Acid Schiff (PAS) positive amorphous structures that lie underneath epithelia of different organs and endothelial cells. It consists of
|
|
|
|
|
|
|
94.
Ans. (a) Lipofuscin
(Ref: Robbins 7/e p39 , 9/e p64)
Important points about Lipochrome or Lipofuscin.
95.
Ans. (c) Lipofuscin accumulation
(Ref: Robbins 8/e p36, 39 – 41, 9/e p64)
96.
Ans. (b) Myeloperoxidase; (e) Cathepsin G
(Ref: Robbins 7/e p73)
Granules of Neutrophils
| |
|---|---|
Specific granules
|
Azurophil granules
|
|
|
97.
Ans. (d) All of the above
(Ref: Robbins 7/e p17 , 9/e p48)
-
Catalase is present in peroxisomes and decomposes H2O2 into O2 and H2O.
-
Superoxide dismutase is found in many cell types and converts superoxide ions to H2O2. This group includes both manganese-superoxide dismutase, which is localized in mitochondria, and copper-zinc-superoxide dismutase, which is found in the cytosol.
-
Glutathione peroxidase also protects against injury by catalyzing free radical breakdown.
98.
Ans. (b) Basophil cells of the pituitary gland in Cushing's syndrome
(Ref: Robbins 8/e p1149)
99.
Ans. (c) Prussian blue stain
(Ref: Robbins 7/e p39- 42, 9/e p64)
100.
Ans. (c) i.e. Methenamine silver
(Ref: Harsh Mohan 6/e p474)
The appropriate stain is methenamine silver. The routine hematoxylin and eosin does not adequately demonstrate the organisms. The cysts, when stained with methenamine silver, have a characteristic cup or boat shape; the trophozoites are difficult to demonstrate without electron microscopy.
101.
Ans. (c) Opsonisation
(Ref: Robbins 8/e p52-53, 7/e p59 , 9/e p78)
102.
Ans. (a) Defect in the enzyme NADPH oxidase
(Ref: Robbins 7/e p61-62, 243-244 , 9/e p79)
Patients with chronic granulomatous disease have defective functioning of phagocytic neutrophils and monocytes.
-
The most common cause of chronic granulomatous disease is defective NADPH oxidase, which is an enzyme on the membrane of lysosomes that converts O2 to superoxide and stimulates oxygen burst. This deficiency results in recurrent infections with catalase-positive organisms, such as S. aureus. Key findings in chronic granulomatous disease include lymphadenitis, hepatosplenomegaly, eczematoid dermatitis, pulmonary infiltrates.
-
A defect in the enzyme adenosine deaminase (ADA) is seen in the autosomal recessive (Swiss) form of severe combined immunodeficiency disease (SCID), while a defect in the IL-2 receptor is seen in the X-linked recessive form of SCID.
-
A developmental defect at the pre-B stage is seen in X-linked agammaglobulinemia of Bruton, while developmental failure of pharyngeal pouches 3 and 4 is characteristic of DiGeorge's syndrome.
102.1.
Ans. (c) Nigrosin
102.2.
Ans. (c) Masson fontana stain
(Ref: Histopathology p150)
Stain
|
Substance
|
|---|---|
Masson Fontana | Melanin |
Oil red O | Neutral lipids and fatty acids |
PAS | Glycogen, mucin, mucoprotein, glycoprotein and fungi |
Gomori methamine silver stain | Fungi (like Cryptococcus, Coccidiodes and Pneumocystis jiroveci (carinii) |
-
Other stains for melanin are Schmorl's method and enzyme histochemical method called DOPA-oxidase (most specific method).
102.3.
Ans. (b) Causes carcinogenesis
(Ref: Robbins 8/e p40, 9/e p67)
-
Telomerase is a specialized RNA-protein complex that uses its own RNA as a template for adding nucleotides to the ends of chromosomes.
-
Regulatory protein sense the telomere length and they restrict the activity of telomerase to prevent unnecessary elongation.
-
Telomerase activity is highest in germ cells and present at lower levels in stem cells, but it is usually undetectable in most somatic tissues
Decreased activity of telomerase is associated with ageing whereas its excessive activity is associated with cancers.29
GOLDEN POINTS FOR QUICK REVISION (CELL INJURY)
-
Hypoxia is the most common cause of cell injury.
-
Neurons are the most sensitive cell to hypoxic injury in the brain.
-
Coagulative necrosis is associated with “tombstone appearance”. It is seen with ischemic injury to all tissues except central nervous system.
-
Best example of coexistence of hypertrophy and hyperplasia is uterus during pregnancy(gravid uterus).
-
Most common metaplasia is squamous metaplasia in the lungs of smokers.
-
CD 95 plays a role in apoptosis.
-
Mitochondria plays a pivotal role on apoptosis
-
Marker for apoptosis (programmed cell death) is annexin V
-
Most important stimulatory gene for apoptosis is p53 gene and most important inhibitory gene for apoptosis is bcl family (bcl-2) of genes.
-
Key words associated with apoptosis: caspases, cytochrome C and embryogenesis
-
‘Chromatin condensation’ is the hallmark feature of apoptosis.
-
“Step ladder pattern” on gel electrophoresis is a feature of apoptosis. Stepladder fever is seen in typhoid/enteric fever.
-
Lipofuscin is also known by several other names like ‘lipochrome’, ‘wear and tear’ pigment, pigment of aging and “indicator of free radical injury”. It gets deposited mostly in heart and liver.
-
The endogenous brown-black pigments include melanin (present in skin) and homogentisic acid (the black pigment in patients with alkaptonuria)
-
Dystrophic calcification: normal serum calcium levels and in dead tissues (areas of necrosis).
-
Metastatic calcification: increased serum calcium levels and in living tissues.
-
“Lungs” are the commonest site for metastatic calcification. Other sites include stomach, pulmonary vein, systemic artery and kidneys.
-
Psammoma bodies: meningioma, papillary thyroid carcinoma, prolactinoma, glucagonoma and serous cystadenoma of the ovary.
-
Gandy gamma body is seen in congestive splenomegaly. It contains hemosiderin and calcium.
-
Oncocytes are formed with modified mitochondria.
-
Germ cells have the capacity for self renewal because of telomerase activation.
-
Cancer cells have the phenomenon of ‘telomerase reactivation’.
-
Germ cells have the maximum telomerase activity amongst all the cells of the body.
-
Cell cannibalization required for self survival is called autophagy.
-
Necroptosis is a caspase independent process which resembles necrosis morphologically and apoptosis mechanistically as a form of programmed cell death.
-
Pyroptosis is a programmed cell death is accompanied by the release of fever inducing cytokine IL-1. It also involves caspases 1 and 11.
-
Commonest fixative used for light microscopic examination: 10% buffered neutral formalin
-
Commonest fixative used for electron microscopic examination: glutaraldehyde
UPDATED INFORMATION FROM 9TH EDITION OF ROBBINS
Necroptosis and Pyroptosis
Autophagy