

INTRODUCTION
The reproductive system or genital system is a system of organs working together for the purpose of reproduction. The two important functions of female reproductive system are to produce female gamete and to nourish developing offspring until birth. The male has primary function of generation of male gamete (sperm) and deposition of the same inside the female reproductive tract for the fertilization of female gamete (ovum).
FEMALE REPRODUCTIVE SYSTEM
The female internal genital organs include:
- Ovaries
- Uterine tubes
- Uterus
- Vagina.
Embryology
Origin
From outer part of intermediate mesoderm (Fig. 1).
Development of Internal Reproductive Organs in Females
Paramesonephric ducts persist in females.1 Internal portion of genital cord undergoes fusion and forms uterus and vagina.


4This begins early in 3rd month of fetal life. Medial walls fuse forming septum which undergoes resorption from below upward. Fallopian tubes are formed from parts outside the cord. At about 5th month, uterocervical junction is marked by a ring-like constriction and at 6th month, thickening of uterine walls begins. Future vaginal fornix is formed from ring-like outgrowth at the lower end of uterus. Simultaneously lumen of vagina is formed by the breakage of central epithelial cells. Hymen is formed from remnant of sinus tubercle.
Atrophy in Female
In the female, atrophy of paramesonephric bodies and ducts occurs. Epoophoron and paroophoron represent nonfunctional remains of mesonephric ducts along with rudimentary blind tubules, situated in the mesosalpinx.
Remnants
Lower part of mesonephric duct disappears, while upper part persists as epoophoron called as Gartner's duct. Suspensory ligaments of ovary are remnants of mesonephric duct too.
Gonads
They start development initially from mesothelial layer of peritoneum.
Ovary is covered by the surface layer named as germinal epithelium. Immature ova originate from cells of dorsal endoderm of yolk sac. In ridge they are called oogonia. Layer of connective tissue cells called as pregranulosa cells surround oogonia. Embryological origin of granulosa cells is controversial. As in males, females also have gubernaculum which pulls ovary downward but is not as developed as in males. Later this divides into ovarian and round ligament of uterus (Fig. 2).
Skene's glands in female urethra are homologous to prostatic glands in males. Epithelial lining of urogenital sinus have diverticula which correspond to Bartholin's glands.
Development of External Genitalia
Until about 9th week of period of gestation, both sexes external genitalia looks same because they follow common path of development. Genital tubercle develops with a dorsal membrane which covers urogenital opening. There is a development of labioscrotal fold which forms the labioscrotal swelling. The urogenital fold evolves into labia minora and labioscrotal swelling forms labia majora.

Initially cloacal membrane comprises of endoderm and ectoderm which separates cloaca from exterior. Separation of rectum from dorsal part of cloaca occurs and ventral part of cloacal membrane contributes to urogenital membrane. Primordial phallus is formed from tubercle which is the first rudiment of clitoris.
Corpus cavernosum of clitoris arises from mesodermal tissue in phallus with cavernous vascular tissue in it. Prepuce is formed as ectodermal growth into phallus superficial part; horseshoe shape is seen on coronal section. Ectodermal plate is divided centrally into two lamellae. This results in a cutaneous folding named as prepuce. It forms a hood over the glans. The sides of it grow dorsal and forward as the labioscrotal folds forming labia majora. Labia minora arise from the lips of groove on undersurface of phallus and remaining part of phallus forms clitoral glans.
Anatomy
Ovaries
The almond-shaped ovaries are female gonads in which the germ cells develop. Endocrine function is also carried by female gonads. Support of ovary is mesovarium which is a short peritoneal fold. In prepubertal females, ovary has a capsule called tunica albuginea and surface is covered with single cuboidal layer of germinal epithelium. Surface of ovary is dull, grayish appearance, and is continuous with shiny peritoneal mesovarium. At puberty, repeated follicle rupture and ovulation starts which leads to 5distortion and scarring of ovarian surface. Scarring is less in women on oral contraceptive pills. Lymphatics, vascular branches, and nerves pass through suspensory ligament and cross pelvic brim and continue into mesovarium of broad ligament. Due to lack of peritoneum, oocyte is expelled into peritoneal cavity at ovulation. Fimbriae of infundibulum part of fallopian tube trap the oocyte and peristaltic movement of the tube carries it to ampulla for fertilization.
During the embryonic development, the germ cells are differentiated into oogonia which divide mitotically and enter the first phase of meiotic division and get arrested at diplotene stage of prophase one stage without completing it. During fetal life, the primary oocytes are surrounded by a spindle-shaped single layer of squamous cells—primordial follicle. Before puberty, the cortex contains only primordial follicle. Beginning at puberty under the influence of pituitary hormones [follicle-stimulating hormone (FSH)], the primordial follicles grow and enlarge to become primary, secondary, and the large mature follicles which can occupy the part of medulla also. Postpubertal ovary has follicles in different stages of development. In addition to the follicles, the ovary may contain a large corpus luteum of an ovulated follicle or corpus albicans of a degenerated corpus luteum. At birth, the cortex contains about 1–2 million primordial follicles. Most of the follicles degenerate before puberty by the process of apoptosis (programmed cell death). About 40,000 follicles persist at puberty and exhibit periodic changes during the rest of the reproductive life. Out of these, about 5–10 follicles undergo a process of maturation in each menstrual cycle. Mostly one follicle from any one of the two ovaries fully matures, ruptures, and discharges a secondary oocyte in the peritoneal cavity and subsequently picked up by the respective fimbriae. Thus on an average about 400 follicles attain such maturity during reproductive life of a woman.
Ovary is mainly supplied by the ovarian artery branch of abdominal aorta and partly by uterine artery branches. Veins from pampiniform plexus join to form one vein in suspensory ligament of ovary. The right ovarian vein ascends at an acute angle to drain into inferior vena cava and the left ovarian vein drains almost at the right angle into left renal vein.2
Uterine Tubes
The uterine tubes (formerly called oviducts or fallopian tubes) are the channel through which oocyte is carried from periovarian peritoneal cavity to uterine cavity. The uterine tubes lie in the mesosalpinx, forming the free anterosuperior edges of the broad ligaments. Tubes are in posterolateral location of lateral pelvic walls and arch anterosuperiorly to ovaries. In ‘immotile cilia syndrome’ the transport of ova takes place only by peristalsis if at all carried by the tube to the uterine cavity. When an ovary does ovulate and release the oocyte, it is swept into the lumen of the uterine tube by the fimbriae which is further facilitated by the longitudinal grooves on the inner aspect of these fimbriae, suction created by the ciliary beats of the tube and also by the peristalsis of the tubal musculature. During ovulation, the uterine tubes literally come close to the ovary to pick up the oocyte which may be hormone-regulated. Each tube presents two openings: (1) Uterine ostium which is 1 mm in diameter and opens into the superolateral angle of the uterus and (2) the other, pelvic (abdominal) ostium which is 3 mm in diameter, opens at the bottom of infundibulum near the corresponding ovary. The uterine tubes have four parts from lateral to medial end:
- Infundibulum: The funnel-shaped distal end of the tube, closest to the ovary and about 1 cm long, opens into the peritoneal cavity through the abdominal ostium, the circumference of which is surrounded with the fimbria. One of the fimbriae is longer (ovarian fimbria) than the rest.
- Ampulla: Widest and longest part (5 cm), is thin walled, dilated, and tortuous. Fertilization of the ova usually takes place in the ampulla.
- Isthmus: It is rounded and cord-like because the walls are thicker than the lumen and resembles the spermatic cord in men. It joins the uterine tube to the uterus. Length of the isthmus measures about 3 cm. The exceedingly narrow lumen suggests the existence of anatomical sphincter which prevents the entrance of exogenous microorganisms from vagina to the peritoneal cavity.
- Uterine (interstitial/intramural/parts of uterine tube): About 1 cm long, and traverses the thick musculature of the uterus at the junction of the fundus and the uterus to open into the uterine cavity via the uterine ostium (Fig. 3).
Innervation of Ovaries and Uterine Tubes
Both ovarian and uterine plexus supply. Afferent pain fibers along with descending sympathetic fibers of lumbar splanchnic nerves and ovarian plexus merge into cell bodies in T11–L1 sensory spinal ganglia.6

Inferior hypogastric plexuses and pelvic splanchnic nerves merge to cell bodies in the S2–S4 sensory ganglia.
Uterus
The uterus (womb) has pear shape and thick walls, and is a hollow muscular organ. The nongravid uterus is located in lesser pelvis with cervix between urinary bladder and rectum. The normal position of uterus is that of anteversion and anteflexion. In nongravid uterus size is 7.5 × 5 × 2 cm and weight is about 90 g. Its dimensions change rapidly and dramatically during pregnancy. At birth, the uterus is relatively large and has body: cervix ratio of 2:1 because of maternal hormone influence in intrauterine life. Several weeks after birth, childhood dimensions and proportions are obtained. Body: Cervix ratio becomes 1:1. Because of the small size of the pelvic cavity, it remains in the abdomen and descends down afterward and becomes pelvic organ. Typical angulation between the uterus and vagina is not established. During puberty, the uterus (especially the body) grows rapidly in size thereby again assuming adult proportions because of hormonal exposure.
Axes of Uterus
Normally the adult uterus lies in anteversion and anteflexion.
Anteversion: The angle between the cervices relative to the axis of the vagina, measures about 90°, provided the bladder and the rectum is empty. The anteversion is maintained by the forward pull on the uterine fundus by the traction of the round ligaments of the uterus, backward pull on the cervix by the traction of the uterosacral ligaments, and the intrinsic growth of the uterine musculature. Maintenance of the anteversion angle is an important prerequisite to prevent the prolapse of the uterus (Fig. 4).

Anteflexion: The forward angle between the body and cervix at the isthmus, creating the angle of flexion measuring about 125° so that the main bulk of the uterus rests on the bladder for better support. On empty bladder, uterus is in transverse plane.
Flexion of uterus takes place at transverse plane of internal orifice (os). Normally, the uterus rotates forward around this axis known as anteflexion. When it rotates backward (reverse direction) it is referred as retroflexion. Usually found in the cases of disrupted perineal body or weak pelvic floor muscles and ligaments.
Usually the uterus lies in the median plane and is twisted to the right or left side. Sometimes the fundus is tilted more to the right pelvic wall known as dextrorotation of the fundus. In such situations the right uterine tube comes in more close contact with the lateral pelvic wall, and may be related to the pelvic type of the vermiform appendix. 7Consequently, the cervix is tilted more to the left side known as levorotation of the cervix.
The uterus is divided into body and cervix. The body lies between the layers of the broad ligament and is freely movable. It has two vesical and intestinal surfaces. The body is demarcated from the cervix by the isthmus of the uterus, a constricted segment, 1 cm long. The cervix of the uterus is 2.5 cm in length and cylindrical in adult nonpregnant woman. Part between isthmus and vagina is called supravaginal part and vaginal part protrudes in superior most part of anterior vaginal wall. The rounded vaginal part surrounds the external os of the uterus and is surrounded in turn by a narrow recess, the vaginal fornix. The supravaginal part is separated from the bladder anteriorly by loose connective tissue and from the rectum posteriorly by the rectouterine pouch. The slit-like uterine cavity is 6 cm in length from external os to wall of fundus. The uterine cavity continues inferiorly as the cervical canal. The uterine body has three coats: (1) perimetrium which is outer serous coat of peritoneum with thin layer of connective tissue, (2) myometrium which is middle coat of smooth muscle with main branches of vascular and nerve supply traversing through it, and (3) endometrium which is the innermost coat with firm adherence to myometrium. Endometrium attains different histopathology during all the phases of menstrual cycle. The endometrium or mucous membrane of the body of the uterus consists of surface epithelium and lamina propria of variable thickness depending on the stage of menstrual cycle. Before puberty the surface is lined by the ciliated columnar cells; during reproductive period it is lined by the simple columnar epithelium because cilia cannot grow due to repeated destruction of the superficial part of the endometrium. Functionally, the endometrium consists of outer basal layer and inner functional layer. In a nonpregnant female, the inner functional layer with the uterine glands and blood vessels is sloughed off or shed during menstruation, leaving intact the deeper basalis layer with the basal remnants of the uterine glands—the source of cells for regeneration of new functional layer. The basal layer is supplied by the straight basal arteries, whereas the functional layer is supplied by the spiral arteries which are highly sensitive to the hormonal changes in the blood and undergo vasoconstriction before menstruation with eventual casting of endometrium due to ischemic necrosis followed by the hemorrhage.
Menstruation occurs only in primates and in mankind who possess the spiral arteries of the endometrium.
Fundus and body are developed by the fusion of the intermediate parts of the two paramesonephric (Müllerian) ducts. While cervix is developed from the upper part of the uterovaginal canal which in turn is formed by the fusion of the lower vertical parts of the two paramesonephric ducts, the lower part of the uterovaginal canal forms the major portion of the vagina.
The principal supports of the uterus are both passive and active. Pelvic diaphragm acts as active support. Change in tone is due to changes in intra-abdominal pressure conditions and is transmitted through the surrounding pelvic organs and the endopelvic fascia in which they are embedded. Passive support of the uterus is provided by its position. When intra-abdominal pressure is increased, the uterus is pressed against the bladder. The cervix has least mobility due to condensed endopelvic fascia attached to it.
Arterial and Venous Supply of Uterus
Uterus is supplied by the uterine arteries mainly and collateral supply is through ovarian arteries. Uterine plexus veins drain in internal iliac veins. Lymphatics from fundus drain along ovarian vessels to lumbar (caval/aortic) lymph nodes. Isthmic part of tubes and round ligament attachments drain into superficial inguinal lymph nodes.
Vagina
The vagina is a musculomembranous tube (7–9 cm long), extending from cervix to vaginal orifice. All vestibular glands have their opening in vaginal vestibule. The vagina plays role as a canal for menstrual bleeding, receives the penis and ejaculate during sexual intercourse and communicates superiorly with cervix and inferiorly with vestibule of the vagina. The vagina does not have any glands in its wall. Mucous produced by cells in the cervical glands lubricate the vaginal lumen. In a nulliparous adult, the vagina is H-shaped in section with transverse folds called vaginal rugae which render the vagina highly distensible. Before puberty, rugae are absent. In the elderly, the vagina becomes less elastic and appears pale and smooth due to loss of rugae. Vagina is closely related to many pelvic floor muscles which provide support and act as potential sphincters for the vagina. All these muscles rhythmically contract during the orgasm.3
The vaginal epithelium exhibits minimal changes during the menstrual cycle. During the proliferative (follicular) phase of menstrual cycle, under the influence 8of high estrogen secretion, the vaginal epithelium increases in thickness and stimulates the vaginal cells to synthesize and accumulate increased amount of glycogen as these cells migrate toward the vaginal lumen into which they are shed off. The fermentative action of Doderlein's bacillus on glycogen-rich desquamated cellular debris (glycogen is converted to lactic acid) renders the vaginal fluid acidic which inhibits the growth of microorganisms or pathogenic invasion. Hence, the vaginal infections are more common after menopause as the glycogen content becomes lesser. Arterial supply is from tributaries of uterine artery and internal pudendal artery. Uterovaginal venous plexus drains into the internal iliac veins through the uterine vein. Lymphatic vessels from superior part of the vagina drain to internal and external iliac lymph nodes, middle part to internal iliac nodes and inferior part to sacral and common iliac nodes. External os drains into the superficial lymph nodes.
Innervation of Uterus and Vagina
Somatic supply is present in inferior, one-fifth to a quarter of vagina in the form of deep perineal nerve. Sensations of touch and temperature are present. The upper portion of vagina and uterus has visceral innervation by hypogastric and thoracolumbar spinal ganglia.
Applied Anatomy
- During childbirth, myometrial contractions are mediated by hormones at decreasing length intervals so as to dilate lower segment of uterus. During menses, myometrial contractions are responsible for cramping pain.
- Infections of female genital tract can lead to peritoneal infections due to direct communication and vice versa. Major cause of tubal factor infertility is due to salpingitis.
- Patency of tubes can be checked by hystero-contrast salpingography (HyCoSy), ultrasound, and endoscopy.
- Ligation of uterine tubes is a surgical method of birth control. It can be done by either abdominal or laparoscopic route.
- Ectopic tubal pregnancy is the most common ectopic gestation occurring in approximately 1 of every 250 pregnancies. Late diagnosis can result in rupture of ectopic gestation resulting in severe hemorrhage into the abdominopelvic cavity. It should be differentially diagnosed from appendix pathology and acute abdomen.
- Congenital anomalies like unicornate uterus, bicornate uterus, doubled uterine cavities, and uterus didelphys are seen.
- Persistence of remnants of mesonephric ducts in the form of epoophoron can enlarge and result in cyst formation and torsion.
- Increased intra-abdominal pressure can result in increased flexion and version. Damaged ligaments and weak supports of uterus can cause uterovaginal prolapse and retroversion.
- Infection of greater vestibular glands: Palpable when infected. Occlusion can predispose to bartholinitis and cyst formation. It can lead to vulvar adenocarcinomas.
- Emphasis on prepartum classes (Kegel exercises) should be present to reduce the muscular obstruction to passage for fetus and decrease the chances of perineal muscle damage.
- Levator ani muscles are closely related to the vagina on its lateral side, and any pathology to these muscles is significantly responsible for either the painful intercourse or orgasm. From our clinical experience we have noticed many patients, especially suffering from coccydynia (tail bone pain) in which levator ani muscle is mostly tender on rectal examination and surprisingly the same mechanism is seen in the males as well.
Histology
Ovary has cuboidal germinal epithelium continuous with peritoneal mesothelium. Beneath it is fibrous tunica albuginea capsule. Oviduct has mucosa, muscularis layer, and serosa with connective tissue.4
The uterus has mucosa, endometrium, myometrium, and peritoneal layer serosa. Endometrium consists of simple columnar epithelium (ciliated cells and secretory cells) and an underlying thick connective tissue stroma. Vagina has mucosa, muscularis, and adventitia.
MALE REPRODUCTIVE SYSTEM
Introduction
The male reproductive axis of hormones and organs is well-efficient biological system. It is responsible for reproductive tract formation and development, pubertal maturation, and maintenance of fertility. Understanding the basis of male infertility is becoming a growing trend among the infertility specialists because of progressive decrease in 9semen parameters over recent years. To understand the basic pathophysiology and the cause of male infertility, it is imperative to have knowledge about the anatomy, physiology, development, and hormonal control of the male genital and duct system for effective evaluation and treatment of male infertility.
Embryology
As urinary and genital systems are located closely and overlap each other, development of them is described as the development of urinary and reproductive systems together. Intermediate mesoderm forms the reproductive organs embryonically. These embryonic structures are the mesonephric ducts (Wolffian ducts) in males and the paramesonephric ducts (Müllerian ducts) in females.
Origin
Under ectoderm in outer intermediate mesoderm there is C5–T3 vertebral segment which is a series of short evaginations extending caudally from dorsal growth and fuses successively from before backward to form pronephric duct. It grows caudally to open into ventral part of cloaca to form mesonephric duct which remains after atrophy of pronephros duct.
Development of Internal Reproductive Organs in Male
In males, duct persists to form tube of epididymis, vas deferens, and ejaculatory duct. Seminal vesicles arise during 3rd month of fetal life from hinder part. A large part of head of mesonephros atrophies leaving anterior efferent ducts of testicle and posterior ductuli aberrantes and paradidymis.
Paramesonephric Ducts
After formation of mesonephric ducts, paramesonephric ducts develop. Each arises on lateral aspect of corresponding mesonephric duct as tubular invagination of cells lining abdominal cavity. Ducts pass backward lateral to mesonephric ducts, but toward the posterior end of the embryo they cross medially and lie side to side leading to the formation of common genital cord. The mesonephric ducts end in an epithelial elevation, the sinus tubercle on the ventral part of the cloaca between the orifices of the mesonephric ducts. Sinus tubercle connects paramesonephric ducts with cloaca.
Atrophy in Males
Paramesonephric ducts atrophy and only traces of anterior ends form appendix of testis of male, while terminal fused portions form the prostatic utricle in the floor of the prostatic urethra. This is due to production of anti-Müllerian hormone (AMH) by sertoli cells of testes.
Gonads
They initially develop from the mesothelial layer of peritoneum. Testis periphery is converted into tunica albuginea. Cords of central mass form a network to become rete testis and seminiferous tubules. Via the rete testis, the seminiferous tubules become connected with efferent ducts of the testis. Descent of testes occurs followed by the development of gubernaculum.5 Failure in this process leads to indirect hernia or infantile hydrocele.
Rectum gets separated from dorsal part of cloaca and ventral part becomes primary urogenital sinus. Sinus divides into superficial definitive urogenital sinus and deeper anterior vesicourethral portion. Vesicourethral portion is the deepest portion continuous with allantois. It absorbs ends of mesonephric ducts and associated ends of renal diverticula and gives rise to trigone of urinary bladder and prostatic urethra part. Remainder forms body of the bladder and part of prostatic urethra, its apex is prolonged to umbilicus as narrow canal called as urachus which is obliterated in later life to form the median umbilical ligament in adults.
Prostate
A series of diverticular buds arise from epithelial lining of the urogenital sinus and vesicourethral part of the cloaca, between the 3rd and 4th months. These buds become tubular, and form glandular substance of two lobes which fuse behind urethra and extend onto ventral aspect. Median lobe of prostate is formed as an extension of the lateral lobes between the common ejaculatory ducts and bladder.
Bulbourethral glands also arise as diverticula from epithelial lining of urogenital sinus.
Development of External Genitalia
The urogenital fold evolves into shaft of the penis and labioscrotal swelling evolves into the scrotum. Genital tubercle develops into primordial phallus, the first rudiment of penis. Corpus cavernosum penis and corpus spongiosum penis arise from phallus with the development of cavernous spaces in it later on. The prepuce is formed by the growth 10of a solid plate of ectoderm which is horseshoe-shaped on coronal section. A cutaneous fold of prepuce forms a hood over the glans. Pelvic portion of the cloaca undergoes more development, pushing phallic portion. Labioscrotal folds extend around to form scrotal area. During descent, along with testis, scrotal area is drawn out to form scrotal sacs. The penis is developed from the phallus. Urogenital membrane undergoes absorption, forming a channel on the undersurface of the phallus; this channel extends only as far forward as the corona glandis. Longer urethra is formed by the greater growth of pelvic portion of cloaca. Later, this opening, which is located on the dorsal side of the penis closes from behind forward. Urethral plate of the glans breaks and forms median groove continuous with primitive ostium. Groove closes leaving small pipelike opening in between. Thus, the urogenital opening is shifted forward to the end of glans.6
Anatomy
During the embryonic development, the male genital tract is a straight duct system with the developing testes high up inside the abdomen and the ejaculatory organ (penis) outside the body. Since testes needs 1–2°C temperature lower than normal body temperature to function normally, it descends down in the scrotum normally during birth outside the body forming a loop of duct system. Vasa deferentia run parallel to the urethra but in the opposite direction. The initial secretory part of the duct begins outside the body (scrotum), the middle part intra-abdominal, and the terminal ejaculatory part ends outside.
The male internal genital organs include the testes, epididymides, ductus deferens, seminal glands, ejaculatory ducts, prostate, and bulbourethral glands.7
Testis is suspended in the scrotum by spermatic cord which starts at deep inguinal ring lateral to inferior epigastric vessels, passes in inguinal canal, and comes out of superficial inguinal ring, ending at scrotum. The coverings of the spermatic cord include the following: Internal spermatic fascia, cremasteric fascia and muscle, and external spermatic fascia. It contains vas deferens, testicular artery, cremasteric artery, artery of ductus deferens, pampiniform venous and lymphatic plexus, sympathetic nerve fibers, and processus vaginalis. The cremaster muscle is responsible for the cold reflex which draws testis superiorly. Warm reflex is opposite to it. These occur to regulate temperature of testis for regulating spermatogenesis (1°C below core temperature).

Genital branch of genitofemoral nerve (L1 and L2) innervates cremaster striated muscle, while dartos is a smooth muscle innervated by the autonomic nerves (Fig. 5).
Scrotum
The scrotum is sacular part consisting of two layers—heavily pigmented skin and a fat-free dartos fascial layer along with smooth muscle fibers giving rugose appearance to scrotum. In cold conditions, contraction of dartos muscle causes thickening of integumentary layer as it is attached to the skin, and reduces scrotal surface area overall, thus reducing heat loss.
The scrotum is divided by scrotal raphe. It marks line of fusion for embryonic labioscrotal swellings. Fascia does not contain fat. The arterial supply of scrotum is from the perineal artery (branch of internal pudendal artery), deep external pudendal artery, and cremasteric artery. Scrotal veins accompany arteries. Superficial inguinal lymph nodes drain it. Innervation is by genital branch of the genitofemoral nerve (L1, L2), ilioinguinal nerve (L1), and posterior scrotal branches of pudendal nerve (S2–S4), and perineal branches of the posterior cutaneous nerve of thigh (S2, S3).
Testes
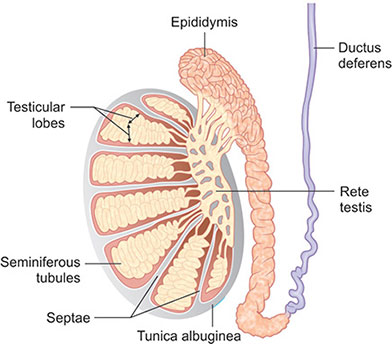
Testes are the male gonads suspended in the scrotum by the spermatic cords, with the left testis inferior to right testis. Each has a volume of 15 mL or more and measures around 5 cm in length. The surface is covered by visceral layer of the tunica vaginalis, except at attachment to epididymis and spermatic cord. Fluid separates visceral and parietal layers for free movement in scrotum. The testes have a 11tough fibrous outer surface, the tunica albuginea that thickens into a ridge on its internal and posterior aspect as the mediastinum of the testis. It has little distensibility, thus any condition leading to edema can cause ischemic damage to the testis. Beneath tunica albuginea is a vascular layer called tunica vasculosa which contains blood vessels containing numerous mast cells.8 A thin connective tissue septum extends from the mediastinum testis anteriorly and subdivides each testis into about 250 incomplete compartments or testicular lobules, each containing 1–4 coiled seminiferous tubules. The mediastinum contains a network of channels known as the rete testis which receives the terminal segments of the seminiferous tubules (straight tubules) in which the sperms are produced.
Each testicular lobule contains tightly packed seminiferous tubules and sparse interstitial connective tissue. Each seminiferous tubule is lined by stratified germinal epithelium, containing proliferative spermatogenic (germ) cells and nonproliferating supporting (sustentacular) or Sertoli cells.9 It is in these seminiferous tubules where spermatogenic cells divide, mature, and are transformed into sperms (Fig. 6).
Surrounding each seminiferous tubules are connective tissue cells, blood vessels, nerves and lymphatic vessels, and steroid-secreting cells, the interstitial cells of Leydig producing testosterone. Seminiferous tubules comprise 95% of testicular volume, and are devoted to the production of spermatozoa. There are approximately 500 tubules per testis. The tubules are divided by fibrous septae, and surrounded by the tough tunica albuginea. Each tubule is 30–70 cm long and 200–300 µm in diameter. Tight convolutions can result in incomplete obstruction. As the tubule reaches the mediastinum, convolutions decrease, and ultimately straightens out to form tubuli recti (straight ducts), which connects to the developmentally different set of network of tubules called rete testes. Sperm produced by the seminiferous tubules passes out of the testis into the ductal system, beginning with the rete testis to epididymis and then to the vas deferens. Sperm in the vas deferens is joined by the seminal vesicle secretions as they pass through the prostate via the ejaculatory ducts into the urethra.
The long testicular arteries arise from abdominal aorta just inferior to the renal arteries. Pampiniform plexus converge, forming right testicular vein which enters inferior vena cava and left testicular vein which enters left renal vein and surrounds the testicular artery in the spermatic cord. It provides thermoregulation. The lymphatics drain into bilateral lumbar and preaortic lymph nodes. The autonomic nerves contain vagal parasympathetic and visceral afferent fibers and sympathetic fibers from T10–T11 segment.
Epididymis
The epididymis is an elongated structure on posterior surface of testis which receives sperms from efferent ductules through rete testis. It has convolutions and appears solid. The epididymis has three parts namely—(1) head which is superior extended part composed of lobules of coiled ends of 12–14 efferent ductules, (2) body which is major part consisting of the tightly convoluted duct of the epididymis, and (3) tail which is tapering continuation with the ductus deferens.10 It is made up of tightly packed convoluted tubules with little supporting loose connective tissue. These efferent ductuli are very fine and lined by highly ciliated columnar epithelium for maximum absorption of water, both to increase the concentration of sperms as well as to transport the sperms from testes to epididymis by creating the suction effect. The walls have myoid cells which undergo frequent contractions to enhance the absorption of fluid as well as mobilization of sperms.
All these minute ductules of the head of epididymis join together and form one single duct which coils on itself called the canal of epididymis or epididymal duct. It forms most of the body and tail of the epididymis and lies alongside the posterolateral border of the testis. The epididymal duct is approximately 6 m in length. The duct is lined by pseudostratified columnar epithelium with nonmotile stereocilia due to absence of axoneme. The passage of sperms 12across the epididymis takes 7–10 days. However, the transit time is dependent on the amount of sperms produced, high the sperm production, less the transit time it takes. From head to tail, it moves by spontaneous peristaltic movements during which sperms attain their maturity, motility, and fertilization capacity. The tail of the epididymis is evolved as the sperm storage organ only in animals forced to wait for female ovulation. Maturation of sperms is dependent on luminal flow of testosterone. Prominent dilatation of epididymal head is known as ‘Bayle's sign’ which is palpable in case of epididymal obstruction or absent vas deferens in men.
Ductus Deferens
The ductus deferens, a primary component of spermatic cord, has thick muscular walls and a minute lumen, giving it a cord-like firmness. It begins in the tail of the epididymis, runs via inguinal canal, and ends by joining the duct of seminal gland to form ejaculatory duct. The relationship of ductus deferens to ureter is similar to that of uterine artery to ureter in the female but is of lesser significance.
In adult, vas measures about 25 cm in length and can be palpated as a 3–5 mm thick string in both sides of the scrotum. The ductus deferens enlarges and forms ampulla of ductus deferens (2 cm in length) before its termination. Ampulla also serves as the storage for the sperms prior to the ejaculation but is controversial because of the temperature issues. Because of the long and complicated course of the duct, absence of the duct or multiple blocks in the duct, surgical retrieval followed by the assisted reproductive technology (ART) is preferred over corrective surgeries.
The vas has three robust layers of smooth muscles, outer and inner longitudinal, and middle circular layers. These muscles are under the sympathetic stimulation and show mass contraction when stimulated which transports spermatozoa from epididymis tail to prostatic urethra within a second.
Artery to ductus deferens supplies ductus deferens. Veins drain into testicular vein including distal pampiniform plexus.
Seminal Glands
Each seminal gland (vesicle) is an elongated structure lying between the fundus of the bladder and rectum, 5 cm long approximately. Seminal glands do not store sperms as believed earlier. They secrete a thick alkaline fluid mixed with fructose and coagulating agent that mixes with sperms as they pass into ejaculatory ducts and urethra. Inferior vesical and middle rectal arteries supply it. Veins accompany it. The secretion of the gland is viscid, yellowish white alkaline fluid, and forms the bulk of the semen which is rich in fructose, prostaglandin, and a coagulating enzyme—vesiculase. The activity of the mucous membrane is regulated by the secretion of the androgen (testosterone). Fructose is believed to serve as an energy source of sperms. The seminal glands contain 40 million times higher concentrations of prostaglandins than the blood. In cases of absent vas deferens, the seminal glands are also absent in most of such cases as they have same developmental origin (Wolffian duct system) (Fig. 7).

Ejaculatory Ducts
The ejaculatory ducts arise by the union of the ducts of the seminal glands with the ductus deferentes approximately 2.5 cm long. The ejaculatory ducts converge to open on seminal colliculus by tiny, slit-like apertures on, or just within the opening of the prostatic utricle. Ducts traverse the glandular prostate but secretions from prostate gland do not join seminal fluid till ejaculatory ducts terminate in the prostatic urethra. Ejaculatory ducts have same blood supply as ductus deferens. The veins join the prostatic and vesical venous plexuses.
Prostate
Prostate is firm and walnut size of approximately 4 × 3 × 2 cm and is the largest accessory gland of the male reproductive 13system surrounding the prostatic urethra. Two-thirds part is glandular and one-third is fibromuscular. Capsule is fibrous and neurovascular, incorporating the prostatic plexuses of veins and nerves.11
The prostatic ducts are 20–30 in number opening chiefly on posterior wall of urethra through sinuses. Prostatic fluid is acidic and milky fluid forming 20% of semen volume and is biochemically very active. Prostatic secretions contain large amount of enzymes which play a role in both semen clotting as well as liquefaction. The enzyme vesiculase induces clotting and a number of proteases, peptidases, and hyaluronidase which cause the breakdown of the clot.
Inorganic elements like zinc, magnesium, and calcium are also present. Zinc is known to provide protection of spermatozoa against spermiophagic cells in the female genital tract and acts as a chelating agent by protecting free sulfhydryl groups present on protamines so as to prevent “super-stabilization” of the condensed chromatin of sperm.
The prostatic arteries are mainly branches of inferior vesical arteries, internal pudendal, and middle rectal arteries. The prostatic venous plexus drains into internal iliac veins. It is continuous with the vesical venous plexus and the internal vertebral venous plexus.
Bulbourethral Glands
Also known as Cowper's glands. They are pea-sized. Ducts open in spongy urethra in bulb of penis. Their mucus-like secretion enters the urethra during sexual arousal.
Innervation of Male Pelvis
The ductus deferens, seminal glands, ejaculatory ducts, and prostate are richly innervated by sympathetic nerve fibers with presynaptic cell bodies in intermediolateral cell column of T12–L2 (or L3) spinal cord segments.
Presynaptic parasympathetic fibers from S2 and S3 spinal cord segments traverse pelvic splanchnic nerves and join the inferior hypogastric or pelvic plexuses. During orgasm, sympathetic system stimulates contraction of the internal urethral sphincter to prevent retrograde ejaculation. Simultaneous stimulation causes rapid peristaltic contractions of ductus and secretion from seminal and prostate glands results in expulsion of semen during ejaculation. Parasympathetic fibers traverse the prostatic nerve plexus to form the cavernous nerves that pass to the erectile bodies of the penis, which are responsible for producing penile erection.
Vascular Supply and Lymphatic Drainage
The arterial supply of scrotum is from the perineal artery (branch of internal pudendal artery), deep external pudendal artery, and cremasteric artery. Scrotal veins accompany the arteries. Lymphatic drainage is by superficial inguinal lymph nodes. The long testicular arteries arise from the abdominal aorta just inferior to the renal arteries. Pampiniform plexus converges into right and left testicular vein. The lymphatics of testis drain into preaortic and lumbar lymph nodes. The artery to ductus deferens is the arterial supply of ductus deferens. Veins drain into the testicular vein, including the distal pampiniform plexus. Inferior vesical and middle rectal arteries supply seminal vesicles. Veins accompany it. The arteries to ductus deferens supply the ejaculatory ducts. The veins follow prostatic and vesical venous plexuses. Prostatic arteries are mainly the branches of inferior vesical arteries, internal pudendal, and middle rectal arteries. Prostatic venous plexus drains into internal iliac veins. It is continuous with the vesical venous plexus and the internal vertebral venous plexus.
Applied Anatomy
- The common method of sterilizing males is vasectomy. Ductus deferens is ligated through incision in superior scrotum. Recently no scalpel vasectomy is done these days. Reversal of vasectomy is successful in young patients of less than 30 years of age and having less than 7 years of postoperative time. An operating microscope-aided reattachment of ends of sectioned ductus is done.
- Seminal gland enlargement and abscesses can be palpated during a rectal examination. For microscopic examination, seminal glands are massaged to release secretions to detect the organism for gonococci infection.
- Prostate hypertrophy is common after middle age affecting urination by distorting the prostatic urethra and causing dysuria, urgency, nocturia, cystitis, and kidney damage. Examination can be done by digital rectal examination.12
- Prostate-specific antigen (PSA) is secreted by prostate, clinically used as a clinical marker in suspected cases of carcinomas.
- Ejaculatory duct obstruction can be suspected in fructose negative cases which can be resected through transurethral resection of duct (TURD).

- Horizontal testes are more prone for torsion injuries.
- Small size testis is indicative of damage to the seminiferous epithelium which forms the major portion of the testicular volume. It can be measured by orchidometer.
- Small and firm testes, usually less than 3 mL in volume are found in Klinefelter syndrome men.
- Patients with hypogonadotropic hypogonadism have small testes but size usually measures between 5 mL and 12 mL.
- Microdeletions in Y chromosome are found in higher rates in infertile men than in fertile controls. Azoospermia factor (AZF) focus at Yq11 has partial deletion of AZFa, AZFb, and AZFc with Sertoli-cell- only syndrome (Fig. 8), maturation arrest (Fig. 9), and occasional spermatogenesis, respectively.
- Anesthesia for sperm retrieval techniques: Local anesthesia in percutaneous epididymal sperm aspiration (PESA) or testicular or epididymal sperm aspiration (TESA) can be achieved by injecting 10 mL of 1% lignocaine solution along sides of vas deferens near external inguinal ring. This is called spermatic cord block. Only in apprehensive patients, intravenous sedation can be given as back up. For microsurgical procedures, general anesthesia is preferred.
Penis
The penis is male copulatory organ and provides common outlet for urine and semen. It consists of glans, body, and root. It is composed of three cylindrical cavernous bodies of erectile tissue: the paired corpora cavernosa and single corpus spongiosum. Penis is in anatomical position when erect and its dorsum is anterior in flaccid condition. The skin of the penis is thin, darkly pigmented relative to adjacent skin, and connected to the tunica albuginea by loose connective tissue. At the neck of the glans, the skin and fascia of the penis are prolonged as a double layer of skin, the prepuce (foreskin) which in uncircumcised males covers the glans penis mostly.

Penis is supplied by dorsal artery of penis, deep artery, and artery of bulb of penis. Cavernous space blood is drained through prostatic venous plexus.
Innervation of Penis
The nerves derive from the S2– S4 spinal cord segments and spinal ganglia, passing through the pelvic splanchnic and pudendal nerves, respectively. Sensory and sympathetic innervation is provided primarily by the dorsal nerve of the penis.
Erection, emission, ejaculation, and remission: When a male is stimulated erotically, arteriovenous anastomoses are closed and smooth muscles relax due to parasympathetic stimulation. This results in increased blood flow to cavernous spaces in corpora of penis. The bulbospongiosus and ischiocavernosus muscles compress veins impeding venous flow return. As a result, engorgement of erectile bodies occurs resulting in erection.
Emission (expression of secretions into the urethra) is a sympathetic response (L1–L2 nerves). During ejaculation, expulsion of semen occurs through external urethral office 15due to closure of internal urethral sphincter (sympathetic) and contraction of urethral and bulbospongiosus muscle (parasympathetic). After ejaculation, penis becomes flaccid due to relaxation of muscles allowing blood to drain from cavernosa to deep dorsal vein.
The first part of the semen comes from the cauda of the epididymis suspended in prostatic fluid. Spermatozoa in zinc-rich prostate fluid preserve motility, vitality, and the stability of their nuclear chromatin. The second part is mainly composed of a fluid from the seminal glands, which is rich in fructose and prostaglandin. The first part of the ejaculate is deposited on to the cervical mucus comprising of spermatozoa in prostatic fluid and the second part of the semen mainly from seminal glands forms the plug to prevent backflow of the first part of the ejaculate. Semen collected in predetermined sequence is known as a ‘split ejaculate’.
Semen
Semen is a grey opalescent fluid. Testes have 5% contribution to ejaculate and seminal vesicles and prostate make up to 90%. The remaining 5% of the ejaculatory volume is formed by the bulbourethral and urethral glands. These volumes are outlined in Table 1. Secretions have important role. Minor changes also in consistency of fluid have profound effect. Reproductive failure can be the result of pathology in one of the accessory glands rather than the result of any abnormality of sperm production.
After ejaculation, mixing of components takes place and thus loss of any part of semen sample during ejaculation can result in a false positive abnormality in semen analysis.
Testicular Contribution
No major contribution is there toward volume so after vasectomy, semen volume does not change. The fluid from testis enters efferent ductules and is known as rete testis fluid. This fluid is rich in testosterone which is bound to androgen-binding protein (ABP) secreted by the Sertoli cells. Rete testis fluid also contains inhibin, ceruloplasmin, and transferrin.
Reduction in their concentration is seen in men with epididymal obstruction and Sertoli cell dysfunction.
Lactate dehydrogenase C4 is an enzyme released when sperms die or break up. Its presence may indicate damage of sperm during passage through epididymal duct. L-carnitine and glycerophosphorylcholine are added through the passage in epididymal duct.
Seminal Vesicles and Their Secretions
Seminal vesicle secretions make 40–60% of total ejaculatory volume. It has major effect on the functions of sperm and physical properties of seminal plasma. It is alkaline, contains fructose, prostaglandins, and fibrinogen-like substrate on which enzyme vesiculase acts to induce clotting. Fructose component is absent in some mammals such as dog and horse. Prostaglandins may act as calcium ionophores.
Prostatic fluid is biologically active and contains enzymes involved in semen clotting and liquefaction. It also contains protease, peptidase, and hyaluronidase. The prostatic secretions also contain the bacteriostatic amine called spermine, acid phosphatase, citrate, calcium, zinc, and magnesium. Crystallization may be seen when a semen sample is left for some time and pH of the seminal plasma is allowed to fall.
Secretions of the bulbourethral and urethral glands have little significance. Immunoglobulin G present in it is responsible for antisperm antibodies.
Endocrinology of the Testis
Leydig cells secrete testosterone and Sertoli cells secrete inhibin and ABP and follistatin in the testis. This is controlled by pituitary gonadotropins—luteinizing hormone (LH) and FSH which in turn are under control of hypothalamic hormone, gonadotropin-releasing hormone (GnRH). LH acts on Leydig cells and FSH acts on Sertoli cells. A concentration gradient for testosterone thus exists between the interstitial tissue and the interior of the Sertoli cell. ABP testosterone complex is formed within the Sertoli cell and provides androgen for spermatogenesis. This ABP testosterone complex enters lumen of the seminiferous tubules by exocytosis. Testosterone has a negative paracrine feedback action for LH on the pituitary–hypothalamic axis. Inhibin acts as negative feedback for FSH secretion. Inhibin is produced in two forms known as b-A and b-B. The subunit b-B is present only in male serum.16

Fig. 10: Hormonal circuit for male reproduction.
(GnRH: gonadotropin-releasing hormone; FSH: follicle-stimulating hormone; LH: luteinizing hormone).
There is an inverse relationship between inhibin B and FSH in male sera but no such relationship exists between inhibin A and FSH levels in the serum of male patients. Damage to the Sertoli cell reduces inhibin B production and therefore will cause an increase in FSH secretion. Activin stimulates FSH production.13
Follistatin also suppresses FSH secretion, but it is much less potent than inhibin. Sertoli cells also produce modulating substance to act on Leydig cells. Thus it is a complex interrelationship between cells and axis (Fig. 10).
Histology
Interstitial tissue is interspersed with convoluted tubules and has tunica vasculosa testis tissue beneath tunica albuginea. Tubules are surrounded by 3–4 layers of smooth muscle cells or myoid cells (Fig. 11).
Primary spermatocytes are visible in cross sections of seminiferous tubules. Incomplete cell divisions result in syncytium of cells with bridges of cytoplasm in between. Spermatids lie in lumina of seminiferous epithelium. They are small with nucleus in eccentric position. During condensation, nucleus becomes smaller and stains darker.
The nucleus of Sertoli cells is ovoid or angular and contains a large nucleolus. Nuclear membrane fold is characteristic for Sertoli cells but not always visible in light microscope. Tight junctions form blood–testis barrier.

Spermatozoa pass through tubuli recti having low columnar epithelium and rete testis having flattened or cuboidal epithelium into a number of ductuli efferentes, containing both absorptive and ciliated cells.
The ductuli efferentes are lined by tall pseudostratified columnar epithelium. Toward the basal lamina are present a number of small nuclei, belonging to basal cells of the ductus epididymidis. These cells regenerate the epithelium.
The vas deferens is lined by pseudostratified columnar epithelium with long stereocilia.
Simple columnar epithelium of prostatic secretory ducts changes into transitional type near openings of ducts. Corpora amylacea in secretory alveoli are characteristic features of prostate with round eosinophilic bodies.
Seminal vesicles mucosa is branched into anastomosing folds of honeycomb-like structure with columnar or pseudostratified lining. Lumen is filled with acidophilic secretion.
KEY NOTES
The human reproductive system is a complex arrangement of specialized organs. These organs function efficiently under influence of neural and hormonal signals together with each other to produce a new life.
REFERENCES
- Moore KL, Persaud TVN. The Developing Human: clinically oriented embryology, 8th edn. Philadelphia: Saunders; 2008.
- Datta AK. Essentials of Human Anatomy (Thorax and abdomen), 8th edn. India, Kolkata: Current Books International; 2008.
- Eroschenko VP. diFiore's Atlas of Histology with Functional Correlations, 11th edn. Philadelphia. Lippincott Williams & Wilkins; 2008.
- Backhouse KM. The gubernaculum testis Hunteri: testicular descent and maldescent. Ann R Coll Surg Engl. 1964;35(1):15–33.
- Differentiation of the urogenital sinus in males: Embryology. ch. Retrieved 2016.
- Moore KL, Dalley AF, Agur AMR. Clinically Oriented Anatomy, 6th edn. Philadelphia. Lippincott Williams & Wilkins. 2010.
- Dym M, Fawcett DW. The blood-testis barrier in the rat and the physiological compartmentation of the seminiferous epithelium. Biol Reprod. 1970;3(3):308–26.
- Clermont Y. The cycle of the seminiferous epithelium in man. Am J Anat. 1963;112(1):35–51.
- Glover TD, Nicander L. Some aspects of structure and function in the mammalian epididymis. J Reprod Fertil Suppl. 1971;13(Suppl 13):39–50.
- Aumuller G. Morphologic and regulatory aspects of prostatic function. Anat Embryol (Berl) 1989;179(6):519–31.
- Myers RP, Cahill DR, Devine RM, et al. Anatomy of radical prostatectomy as defined by magnetic resonance imaging. J Urol. 1998;159(6):2148–58.
- Brooks DE. Epididymal functions and their hormonal regulation. Aust J Biol Sci. 1983;36(3):205–21.