

SKELETON
Bone is a calcified connective tissue consisting of cells (osteocytes) embedded in a matrix of ground substance and collagen fibers.
- It has a superficial thin layer of compact bone around a central mass of spongy bone, and contain internal soft tissue, the marrow, where blood cells are formed.
- It serve as a reservoir for calcium and phosphorus and act as biomechanical levers on which muscles act to produce the movements permitted by joints.
Long bones have a shaft (diaphysis) and two ends (epiphyses). The metaphysis is a part of the diaphysis adjacent to the epiphyses.
- Diaphysis
- Forms the shaft (central region) and is composed of a thick tube of compact bone that encloses the marrow cavity.
- Metaphysis
- Is a part of the diaphysis, the growth zone between the diaphysis and epiphysis during bone development.
- Epiphyses
- Are expanded articular ends, separated from the shaft by the epiphyseal plate during bone growth and composed of a spongy bone surrounded by a thin layer of compact bone.
OSSIFICATION
- Ossification is the process of laying down new bone material by cells called osteoblasts. It is of two types:
- Membranous ossification is the direct laying down of bone into the mesenchyme (embryonic connective tissue).
- Endochondral ossification involves osteogenesis in a precursor model of cartilage.
- Membrane (dermal) bones ossify in membrane (intramembranous ossification), and are thus derived from mesenchymal condensations. The flat bones of the skull and face, the mandible, and the clavicle develop by intramembranous ossification.
- Cartilaginous bones ossify in cartilage (endochondral ossification), and are thus derived from preformed cartilaginous models. The bones of the extremities (limbs) and those parts of the axial skeleton that bear weight (vertebral column and thoracic cage) develop by endochondral ossification.
- Membrano-cartilaginous bones are initially formed in membrane but later partly in cartilage. Examples: clavicle, mandible, occipital, temporal, sphenoid.
- Cartilaginous ossification involves primary and secondary centers of ossification:
- Primary center of ossification
- In long bones, bone tissue first appears in the diaphysis (middle of shaft).
- Primary centers starts appearing at week 6 of intrauterine life.
- Chondrocytes multiply and form trabeculae and cartilage is progressively eroded and replaced by bone, extending towards the epiphysis.
- A perichondrium layer surrounding the cartilage forms the periosteum, which generates osteogenic cells that make a collar to encircles the exterior of the bone and remodels the medullary cavity on the inside.
- The nutrient artery enters via the nutrient foramen from a small opening in the diaphysis.
- It invades the primary center of ossification, bringing osteogenic cells (osteoblasts on the outside, osteoclasts on the inside.)
- The canal of the nutrient foramen is directed away from more active end of bone when one end grows more than the other.
- When bone grows at same rate at both ends, the nutrient artery is perpendicular to the bone.
- 2Secondary center of ossification
- The secondary centers generally appear at the ends (epiphysis) of long bones.
- Secondary ossification mostly occurs after birth except for secondary centers around knee joint (distal femur and proximal tibia), which appear during last weeks of fetal life (or immediately after birth).
- The epiphyseal arteries and osteogenic cells invade the epiphysis, depositing osteoblasts and osteoclasts which erode the cartilage and build bone. This occurs at both ends of long bones but only one end of digits and ribs.
Ossification centers which appear prenatally (ossified at birth) are: diaphysis of long bones, skull bones, vertebral column, ribs and sternum, few foot bones (talus, calcaneum, cuboid).
Primary center of all carpal and tarsal bones (except talus, calcaneum and cuboid) appear after birth.



Figs. 2A and B: Growth of bone—lengthwise: (A) Four zones of epiphyseal cartilage; (B) Conversion of calcified cartilage into bone
GROWING END
- The growing ends of bones in upper limb are upper end of humerus and lower ends of radius and ulna.
- In lower limb, the lower end of femur and upper end of tibia are the growing ends.
- The nutrient foramen is directed away from the growing end of the bone; their directions are indicated by a memory aid: ‘Towards the elbow I go, from the knee I flee’.



Fig. 5: Arterial supply of a long bone. The upper epiphysis (growing end) has not yet fused with the diaphysis
BLOOD SUPPLY
Nutrient artery enters the diaphysis (shaft) through the nutrient foramen, runs obliquely through the cortex, and divides into ascending and descending branches in the medullary cavity.
- Each branch divides into a number of small parallel channels which terminate in the adult metaphysis by anastomosing with the epiphysial, metaphysial and periosteal arteries.
- It supplies medullary cavity, inner 2/3 of cortex and metaphysis.
- The nutrient foramen is directed away from the growing end of the bone. Memory aid: Towards the elbow I go, from the knee I flee.
SESAMOID BONES
Sesamoid bones develop in certain tendons and reduce friction on the tendon, thus protecting it from excessive wear.
- They are commonly found where tendons cross the ends of long bones in the limbs.
- Sites of sesamoid bones:
- In the ear: The lenticular process of incus is a sesamoid bone and therefore is considered the fourth ossicle of middle ear.
- In the hand: Two sesamoid bones in the distal portions of the first metacarpal bone (within the tendons of adductor pollicis and flexor pollicis brevis).
- In the wrist: The pisiform of the wrist is a sesamoid bone (within the tendon of flexor carpi ulnaris), develops at age 9–12.
- In the knee: The patella (within the quadriceps tendon).
- Fabella in the lateral head of gastrocnemius behind the knee joint.
- Sesamoid bone in the tendon of peroneus longus where it binds around the cuboid bone.
- In the foot: Two sesamoid bones in the distal portions of the first metatarsal bone (within the tendons of flexor hallucis brevis.
PNEUMATIC BONES
- They are generally produced during development by excavation of bone by pneumatic diverticula (air sacs) from an air-filled space such as the nasal cavity.
- E.g., maxilla, frontal, sphenoid, and ethmoid bones and a part of the mastoid part of the temporal bone.
EPIPHYSIS
There are four types of epiphysis:
- Pressure epiphysis are the parts of bone involved in weight transmission (and are intracapsular), e.g. head of humerus and femur and condyles of humerus, femur, tibia, etc.

Figs. 6A to D: Types of epiphyses: (A) Pressure and traction epiphyses; (B) and (D) Atavistic epiphyses; (C) Aberrant epiphysis
- Traction epiphysis are present at the ends of bones and develop due to traction by the attached muscles (and are therefore extracapsular), e.g. greater (and lesser) tubercles in humerus and greater (and lesser) trochanter in femur.
- These epiphyses ossify later than pressure epiphyses.
- Examples of traction epiphyses are tubercles of the humerus (greater tubercle and lesser tubercle), and trochanters of the femur (greater and lesser). Mastoid process is also a traction epiphysis.
- Aberrant (unusual) epiphysis are deviations from the norm and are not always present. E.g., Epiphyses at the head of the first metacarpal and at the base of other metacarpals.
1. Endochondral ossification is/are seen in: (PGIC 2015)
- Long bones
- Clavicle
- Mandible
- Nasal bones
- Flat bones of skull
2. Bones ossified at birth: (PGIC 2015)
- Upper end of humerus
- Lower end of humerus
- Lower end of femur
- Upper end of tibia
- Calcaneum
3. Nutriient artery runs: (NEET Pattern 2012)
- Towards metaphysis
- Away from metaphysis
- Away from epiphysis
- None
4. All of the following statements are true for metaphysis of bone EXCEPT: (AIPG 2003)
- It is the strongest part of bone
- It is the most vascular part of bone
- Growth activity is maximized here
- It is the region favouring hematogenous spread of infection
5. TRUE statement is: (AIPG 2000)
- Osteoblasts give rise to osteocytes
- Growth of bone occurs at diaphysis
- Epiphysis is present between metaphysis and diaphysis
- Interphalangeal joint is a saddle joint
6. Traction epiphysis is/are: (PGIC)
- Head of humerus
- Lesser tubercle
- Deltoid tuberosity
- Coracoid process
- Greater trochanter
7. Which of the following is an aberrant epiphysis: (NEET Pattern 2015)
- Coracoid process
- Greater tubercle of humerus
- Base of 1st metacarpal
- Base of 2nd metacarpal
8. Bones which is/are pneumatic: (PGIC May 2015)
- Maxillary
- Parietal
- Temporal
- Frontal
- Ethmoidal
- a. Long bones; b. Clavicle
- Long bones and medial end of clavicle bone develop by endochondral ossification.
- Flat bones of skull; facial skeleton; mandible and lateral end of clavicle develop by intramembranous ossification.
- c. Lower end of femur; d. Upper end of tibia; e. Calcaneum
- Secondary centers around knee joint (distal femur and proximal tibia) appear during last weeks of intrauterine life (or immediately after birth).
- Primary center of all tarsal bones (except talus, calcaneum and cuboid) appear after birth.
- a. Towards metaphysis
- Nutrient artery enters the shaft (diaphysis) of the bone, divides into ascending and descending branches, which run towards and terminate in the adult metaphysis by anastomosing with the epiphyseal, metaphyseal and periosteal arteries.
- a. It is the strongest part of bone
- The strongest part of bone is diaphysis (not metaphysis).
- During growth of bone maximum activity occurs at growth plate (physis) and the adjacent section of the metaphysis.
- Metaphysis is richly supplied with arteries forming hairpin bends, hence becomes a common site of osteomyelitis in children, as infectious agents are easily trapped in sluggish blood flow in hairpin bends.
- a. Osteoblasts give rise to osteocytes
- Osteoblasts that get trapped in Haversian lamellae become osteocyte and assume the function of bone maintenance. They are no longer involved in bone formation.
- Growth activity is maximum at the growth plate (physis) and adjacent metaphysis.
- Metaphysis is present between diaphysis and epiphysis.
- Interphalangeal joint is a hinge variety of synovial joint.
- b. Lesser tubercle; e. Greater trochanter
- Traction epiphysis are usually present at the ends of bones and develop due to traction by the attached muscles (and are therefore extracapsular), e.g. Greater (and lesser) tubercles in humerus and greater (and lesser) trochanter in femur.
- Pressure epiphysis are involved in weight transmission (and are intracapsular) e.g. head of humerus and femur and condyles of humerus, femur, tibia, etc.
- Coracoid process in scapula is an example of atavistic epiphysis.
- Deltoid tuberosity is not an epiphysis (it is present on the shaft/diaphysis).
- d. Base of 2nd metacarpal
- Aberrant epiphyses are deviations from the normal anatomy and are not always present. For example, the epiphysis at the head of the first metacarpal bone and at the bases of other metacarpals.
- a. Maxillary; c. Temporal; d. Frontal; e. Ethmoidal
- Pneumatic bones have air spaces within them and are present around the nasal cavity.
- Temporal bone is morphologically classified as pneumatic bone because it has an internal air sinus and mastoid air cells.
- Parietal bone is not a pneumatic bone.
JOINTS
Union between bones can be in one of three types: by fibrous tissue; by cartilage; or by synovial joints.
Classification
The structural classification divides joints into fibrous, cartilaginous, and synovial joints depending on the material composing the joint and the presence or absence of a cavity in the joint. The functional classification divides joints into three categories: synarthroses, amphiarthroses, and diarthroses.
Synarthrosis (immovable) | Fibrous joints |
Amphiarthrosis (slight mobile) | Cartilaginous joint |
Diarthrosis (freely mobile) | Synovial joints |
Fibrous joints occur where bones are separated only by connective tissue and movement between them is negligible. Examples of fibrous joints are the sutures that unite the bones of the vault of the skull and the syndesmosis between the lower ends of the tibia and fibula.
Types of fibrous joint | Examples |
|---|---|
Suture | Spheno-vomerine joint (schindylesis) |
Gomphosis | Tooth and socket joints |
Syndesmosis | Middle radioulnar joint Inferior radioulnar joint |
Cartilaginous joints are of two varieties, primary and secondary.
- Primary Cartilaginous Joints (synchondroses) are united by hyaline cartilage and permit no movement but growth in the length.
- A primary cartilaginous joint (synchondrosis) is one where bone and hyaline cartilage meet. Thus, all epiphyses are primary cartilaginous joints, as are the junctions of ribs with their own costal cartilages.
- All primary cartilaginous joints are quite immobile and are very strong. The adjacent bone may fracture, but the bone–cartilage interface will not separate.
- They Includes epiphyseal cartilage plates (the union between the epiphysis and the diaphysis of a growing bone) and spheno-occipital and manubrio-sternal synchondroses.
- Secondary cartilaginous joints (Symphysis) have bones are united by hyaline plus fibrocartilage.
- These joints are usually in the midline and are slightly mobile.
- Include pubis symphysis, midline intervertebral joints.
- Symphysis is a union between bones whose articular surfaces are covered with a thin lamina of hyaline cartilage. The hyaline laminae are united by fibrocartilage.
- There may be a cavity in the fibrocartilage, but it is never lined with synovial membrane and it contains only tissue fluid.
- Examples are the pubic symphysis and the joint of the sternal angle (between the manubrium and the body of the sternum).
- An intervertebral disc is part of a secondary cartilaginous joint, but here the cavity in the fibrocartilage contains a gel.
- A limited amount of movement is possible in secondary cartilaginous joints, depending on the amount of fibrous tissue within them. All symphyses occur in the midline of the body.
Types of cartilaginous joint | Examples |
|---|---|
Synchondrosis | Spheno-occipital joint Epiphysio-diaphyseal joint (growing bone) |
Symphysis | Midline intervertebral joint Sacrococcygeal joint |
- Synovial joints are freely mobile joints.
- Synovial joints are uniaxial: Plane, hinge and pivot; Biaxial: Condylar and ellipsoid; Multiaxial: Saddle, ball and socket.

SYNOVIAL JOINTS
Synovial joints are freely mobile joints. They are uniaxial: Plane, hinge and pivot; Biaxial: Condylar and ellipsoid and Multiaxial: Saddle, ball and socket.7
Types of synovial joint | Examples |
|---|---|
Plane |
|
Hinge |
|
Pivot (Trochoid) |
|
Condylar |
|
Types of synovial joint | Examples |
|---|---|
Ellipsoid |
|
Saddle |
|
Ball and socket |
|
Some authors consider these joints condylar: Atlanto-occipital, wrist (radio-carpal), metacarpo-phalangeal (knuckle).
Some authors consider these joints as modified hinge: Temporo-mandibular, knee joint.

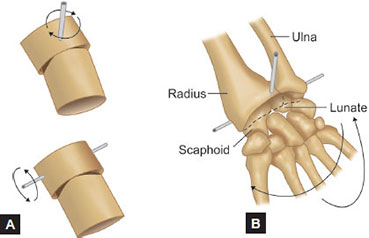
Figs. 9A and B: An ellipsoid joint (A) is shown as analogous to the radiocarpal joint (wrist) (B) The two axes of rotation are shown by the intersecting pins

Figs. 10A and B: A saddle joint (A) is illustrated as analogous to the carpometacarpal joint of the thumb (B). The saddle in A. Represents the trapezium bone. The rider, if present, would represent the base of the thumb's metacarpal. The two axes of rotation are shown in (B)
- Knee joint is a complex joint (involving more than two bones).
- Femoro-tibial joint structurally resembles a hinge joint, but is considered as a condylar type of synovial joint between two condyles of the femur and tibia. In addition, it includes a saddle joint between the femur and the patella.
Hilton's law: A joint is innervated by articular branches of the nerves that supply the muscles acting on the joint and that also supply the skin covering the joint.8
Questions
1. What type of joint is the growth plate? (AIPG 2010)
- Fibrous
- Primary cartilaginous
- Secondary cartilaginous
- Plane joint
2. Atlanto-occipital joint is of synovial variety:
- Trochoid
- Ellipsoid
- Condylar
- Saddle
3. Which of the following is a compound condylar joint? (NEET Pattern 2012)
- Knee
- TM joint
- Wrist
- Elbow
4. Metacarpophalangeal joint is:
- Condylar
- Ellipsoid
- Saddle
- Hinge
5. Which of the following is a synovial joint of the condylar variety? (NEET Pattern 2012)
- First carpometacarpal joint
- Metacarpophalangeal joint
- Interphalangeal joint
- Radiocarpal joint
6. Vomer ala and sphenoidal rostrum junction is: (NEET Pattern 2013)
- Syndesmosis
- Synostosis
- Schindylesis
- Gomphosis
7. Synchondrosis is/are seen in: (AIIMS 2019 Pattern)
- Costo-sternal joints
- Spheno-occipital joint
- Epiphysio-diaphyseal joint
- Manubrio-sternal joint
- Xiphisternal joint
- b. Primary cartilaginous
- Growing bones have epiphyseal (growth) plate between the epiphysis and diaphysis, this epiphyseo-diaphyseal joint is primary cartilaginous (synchondrosis).
- It is found in the growing bone, where the growth plate (hyaline cartilage) connects the epiphysis with the diaphysis, creating a hyaline cartilaginous joint.
- At this site the fate of synchondrosis is synostosis (bony fusion) after the growth plate gets removed and replaced by the bone.
- b. Ellipsoid > c. Condylar
- Functionally it is an ellipsoid synovial joint but structurally it is a condylar synovial joint.
- Head flexion and extension occurs at this joint for the nodding (yes) movement.
- a. Knee
- Knee joint has more than two bones participating (hence compound joint). It is formed by the lateral and medial femorotibial and the femoropatellar joints.
- It is a compound synovial joint incorporating two condylar joints between the condyles of the femur and tibia and one saddle joint between the femur and the patella.
- TM joint is a condylar joint but it involves only 2 bones (not a compound joint).
- Wrist joint is an ellipsoid synovial joint and elbow is a hinge synovial joint.
- b. Ellipsoid > a. Condylar
- Metacarpophalangeal joint has a condyle with elliptical articular surface.
- Structurally it is condylar but functionally ellipsoid synovial joint.
- b. Metacarpophalangeal joint > d. Radiocarpal joint
- This a wrong Questions, since both the joints have condyles with ellipsoid articular surface - are structurally condylar but functionally ellipsoid synovial joints.
- Some authors mention metacarpophalangeal as condylar synovial joint only (hence the answer of first preference).
- c. Schindylesis

- b. Spheno-occipital joint; c. Epiphysio-diaphyseal joint; e. Xiphisternal joint
- Synchondroses are primary cartilaginous unions between bone composed entirely of hyaline cartilage. These joints are immovable and mostly temporary in nature. As the growth ceases they undergo synostosis (i.e. plate of hyaline cartilage is completely replaced by bone).
- Spheno-occipital joint is a synchondrosis joint between the basisphenoid and basiocciput bones, which together when joined from the clivus. When fused, the synchondrosis is often called the spheno-occipital suture- this is a misnomer-as anatomically it is not a suture.
- Epiphysio-diaphyseal joint between the epiphyses and diaphysis of a growing long bone, is a synchondrosis, which later undergoes synostosis.
- Xiphisternal joint is a synchondrosis joint. Some authors mention it as symphysis.
- Costo-sternal joints are plane synovial joints of the costal cartilages of the true ribs with the sternum, with the exception of the first, which is the so called synchondrosis (a misnomer) since the cartilage is directly united with the sternum.
- Manubrio-sternal joint is a secondary cartilaginous (symphysis) joint.
MUSCLES
The orientation of individual skeletal muscle fibers is either parallel or oblique to the line of pull of the whole muscle.
The range of contraction is long with the former arrangement, while the latter provides increased force of contraction. Sartorius is an example of a muscle with parallel fibers.
Muscles with an oblique disposition of fibers fall into several patterns:
- Muscles with parallel fasciculi: These are muscles in which the fasciculi are parallel to the line of pull and have greater degree of movement. These muscles may be:
- Quadrilateral, e.g. thyrohyoid, Pronator quadratus
- Strap-like, e.g. sternohyoid and sartorius
- Strap-like, with tendinous intersections, e.g. rectus abdominis
- Fusiform, e.g. biceps brachii, digastric
- Muscles with oblique fasciculi: When the fasciculi are oblique to the line of pull, the muscle may be triangular, or pennate (feather-like) in the construction. This arrangement makes the muscle more powerful, although the range of movement is reduced. Oblique arrangements are of the following types:
- Convergent fasciculi: The muscle fibers or fasciculi converge at the insertion point to maximize contraction. Such muscles may be: (a) Triangular, e.g. temporalis (b) Fan-shaped, e.g. temporalis.

- Cruciate muscles: In some muscles, fibers or fasciculi are arranged in superficial and deep planes and crossed ‘X’, e.g. sterno-cleidomastoid, masseter, adductor magnus.
- Sphincteric fasciculi: In some muscles, the muscle fibers or fasciculi surround an opening or orifice, thus when they contract the opening is closed or constricted, e.g. orbicularis oculi around the eye and orbicularis oris surrounding the oral orifice.
- Pennate fasciculi: The pennate-fiber muscles resemble the feather, the fleshy fibers correspond to the bars of the feather and the tendon to the shaft, as they are all inserted by tendon. They may be:
- Uni pennate, e.g. flexor pollicis longus, extensor digitorum longus
- Bipennate, e.g. rectus femoris, flexor hallucis longus
- Multipennate, e.g. tibialis anterior, subscapularis, deltoid (acromial fibers).
- Common sites of intramuscular injection
Upper arm (Deltoid) |
|
Gluteal region |
|
Thigh (lateral aspect)(vastus lateralis) |
|
Hybrid (composite) muscles have more than one set of muscles fibers and more than one nerve supply.
- They lie at the boundaries between muscle groups. Usually it incorporates fibers from two adjoining groups and is therefore supplied by two nerves usually.
Muscle |
|
Trapezius |
|
Digastric |
|
Pectoralis major |
|
Subscapularis |
|
Brachialis |
|
Flexor digitorum profundus |
|
Opponens pollicis |
|
Ilio-psoas |
|
Pectineus |
|
Biceps femoris |
|
Adductor magnus |
|
1. All are composite muscles EXCEPT: (AIPG 2009)
- Pectineus
- Flexor carpi ulnaris
- Biceps femoris
- Flexor digitorum profundus
2. Muscle having double nerve supply: (PGIC 2015)
- Digastric muscle
- Omohyoid muscle
- Trapezius
- Thyrohyoid muscle
- Adductor magnus
3. Digastric muscles are the following EXCEPT: (AIPG 2008)
- Occipitofrontalis
- Sternocleidomastoid
- Omohyoid
- Muscular fibers in the ligament of Treitz
4. Which of the following is multipennate muscle: (NEET Pattern 2015)
- Flexor pollicis longus
- Extensor pollicis longus
- Deltoid
- Flexor hallucis longus
- Sartorius
- Rectus abdominis
- Sternohyoid
- Tibialis anterior
6. Which of the following muscle has intracapsular origin: (PGIC 2012)
- Anconeus
- Coracobrachialis
- Long head of biceps femoris
- Popliteus
- Peroneus longus
7. Identify the type of muscle shown in the image (NEET Pattern 2018)
- Cruciate
- Spiral
- Multipennate
- Convergent

- b. Flexor carpi ulnaris
- Flexor carpi ulnaris is supplied by a single nerve and is not a composite/hybrid muscle.
- Composite/hybrid muscles have more than one set of fibers and are supplied usually by different nerves for different set of fibers.
- Pectineus has anterior set of fibers supplied by the femoral nerve, whereas, posterior set of fibers may be supplied by the obturator nerve.
- Long head of biceps femoris is supplied by the tibial part of sciatic nerve, and the short head is supplied by the common peroneal nerve. This reflects the composite derivation from the flexor and extensor musculature.
- Radial half of flexor digitorum profundus is supplied by the median nerve and the ulnar half is supplied by the ulnar nerve.
- a. Digastric muscle; c. Trapezius; e. Adductor magnus
- Anterior belly of digastric is supplied by trigeminal nerve and posterior belly by facial nerve.
- Spinal accessory nerve gives motor fibers to trapezius muscle, whereas ventral rami of C3,C4 are proprioceptive.
- Adductor magnus ischial part is supplied by tibial part of sciatic nerve and adductor part by obturator nerve.
- Inferior belly of the omohyoid is innervated by C1-C3 and the superior belly C1 fibers of ansa cervicalis.
- Thyrohyoid muscle is innervated by C1 fibers traveling with the hypoglossal nerve.
- b. Sternocleidomastoid
- Sternocleidomastoid is a muscle with two heads and one belly, like the biceps brachii.
- Digastric muscles have two bellies.
- Occipitofrontalis muscle has two bellies: Occipital belly and frontal belly.
- Omohyoid: Superior and inferior belly.
- Ligament of Treitz is a digastric muscle with a skeletal muscle belly, which arises from the left crus of diaphragm and a smooth muscle belly which arises from the duodeno-jejunal junction. It has an intermediate tendon attaching to the connective tissue around the celiac trunk of aorta.
- c. Deltoid
- Multipennate muscle has the fiber bundles converge to several tendons.
- d. Tibialis anterior
- The individual fibers of a muscle are arranged either parallel or oblique to the long axis of the muscle.
- Tibialis anterior muscle is a multipennate muscle with oblique fibers.
- Muscles with parallel fasciculi: These are muscles in which the fasciculi are parallel to the line of pull and have greater degree of movement. Few examples are:
- Strap-like, e.g. sternohyoid and sartorius
- Strap-like with tendinous intersections, e.g. rectus abdominis
- d. Popliteus
- Long head of biceps brachii and the popliteus muscle has intracapsular origin.
- Ans. b. Spiral> d. Convergent
- Muscles may exhibit a spiral or twisted arrangement (e.g. sternocostal fibres of pectoralis major or latissimus dorsi, which undergo a 180°-twist between their medial and lateral attachments).
- Some authors consider it as a muscle with convergent fibres as well. The muscle fibers or fasciculi converge at the insertion point to maximize contraction.
- Muscles may spiral around a bone (e.g. supinator, which winds obliquely around the proximal radial shaft), or contain two or more planes of fibres arranged in differing directions, a type of spiral sometimes referred to as cruciate (sternocleidomastoid, masseter and adductor magnus are all partially spiral and cruciate).
PORTAL VENOUS CIRCULATION
- Portal circulation is a capillary network that lies between two veins. Blood supplying the organ thus passes through two sets of capillaries before it returns to the heart.
- In hepatic portal system blood supplying the abdominal organs passes through two sets of capillaries before it returns to the heart.
- A portal circulation also connects the median eminence and infundibulum of the hypothalamus with the adenohypophysis.
- In the renal glomeruli. The glomerular capillary bed lies between afferent and efferent arterioles and may be considered as a portal circulation, but most of the authors do not mention so (including Gray's anatomy).
MISCELLANEOUS
Questions
1. In the following nutrient arteries to bones, choose the WRONG pair:
- Humerus: Profunda brachii
- Radius: Anterior interosseous
- Fibula: Peroneal
- Tibia: Anterior tibial
2. All are Valveless EXCEPT:
- Dural venous sinus
- Hepatic veins
- Inferior vena cava
- Femoral vein
- d. Tibia: Anterior tibial
- Nutrient artery to tibia is a branch of posterior tibial artery.
- d. Femoral vein
- Femoral veins contain between one and six valves, and popliteal veins contain between zero and four valves.
- Deep vein valves are consistently located in the common femoral vein (within 5 cm of the inguinal ligament), the femoral vein (within 3 cm of the deep femoral vein tributary) and in the popliteal vein near the adductor hiatus.