

CHAPTER OUTLINE
- • Dyspnea
- • Chest Pain
- • Syncope
- • Functional Classifications used in Cardiology
Four symptoms need to be covered in the history and they are as follows:
- Dyspnea
- Chest pain
- Syncope
- Palpitations
DYSPNEA
Definition
Dyspnea is defined as an “abnormally uncomfortable awareness of breathing.” The word dyspnea is derived from Greek, meaning dys-difficult and pnoia – breathing.
The American Thoracic Society has defined Dyspnea as “subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity.”
Chronic dyspnea is defined as dyspnea lasting longer than one month.
Qualitative descriptors
- Chest tightness: Bronchospasm, interstitial edema, myocardial ischemia
- Increased work of breathing: COPD
- Air Hunger: CHF, Pulmonary embolism
- Cannot get deep breath: Hyperinflation
- Heavy breathing: Deconditioning.
Mechanism of Dyspnea (Chest 2010; 138: 1196 – 1201)
Hypothetical Model (Gillette and Schwartstein)
- Afferents reach the sensory cortex
- When the feedforward and feedback do not match, an error signal is generated and the intensity of dyspnea increases.
Signals for the Sensation of Dyspnea
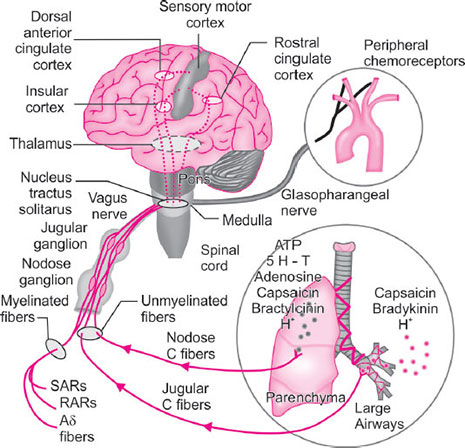
Afferent information from reflex stimulation of the peripheral sensors (chemoreceptors or vagal C fibers) is processed in the Limbic system and sensorimotor cortex and increased neural output to respiratory muscles. A perturbation in the ventilatory response due to increased mechanical load or weakness or paralysis generates afferent information from vagal receptors in the lungs and possibly mechanoreceptors in the respiratory muscles to the sensorimotor cortex and results in the sensation of dyspnea.
It has been shown that vagal C fibers from the jugular ganglion (jugular C fibers) are associated with larger airways. Deeper C fibers in the lungs are associated with nodose ganglia (nodose C fibers). Nodose fibers are stimulated by adenosine. Experiments have shown that IV adenosine can cause dyspnea but no cough and this can be blocked by theophylline and also by inhaled lidocaine (Fig. 1).
Orthopnea
- Dyspnea in supine posture, relieved by sitting up.
- This is due to increased venous return in supine posture leads to more pulmonary congestion
- Causes of orthopnea:
- Left heart failure
- COPD
- Large ascites
- Bilateral diaphragmatic paralysis
- Any severe right heart failure.

Paroxysmal Nocturnal Dyspnea (PND)
- In this form of dyspnea, breathing difficulty occurs 2–6 hours after sleep, especially in the early morning hours.
- This is due to interstitial edema of the lung
- The suggested mechanism is that, there is decreased sympathetic drive during sleep decreases the functional capacity after ventricle. In addition increased absorption of edema fluid results in overfilling of the lungs
- Conditions that can mimic PND are:
- Bronchial Asthma
- Sleep apnea with arousal
- Postnasal discharge with cough
- Nocturnal angina with dyspnea equivalent.
Platypnea
This type of dyspnea occurs in sitting posture. This can occur in left atrial myxoma or with ball valve thrombus of left atrium.
Platypnoea-orthodeoxia is an uncommon syndrome of dyspnea induced by upright posture, with associated arterial hypoxemia, which is subsequently relieved by recumbency. The syndrome occurs when there is right to left shunting of blood, usually via an interatrial communication, in the presence of normal pulmonary artery pressure. This is an unusual situation given that most cases of significant right to left intracardiac shunting of blood are associated with increased right-sided cardiac pressures.
Various theories have been advanced to explain why patients with a patent foramen ovale may develop this syndrome.
- Preferential blood flow directed towards the atrial septum, which can be accentuated by altered intracardiac anatomical relations.
- Unequal diastolic compliance between the right and left sides of the heart, and transient right to left pressure gradients associated with respiratory maneuvers, all of which can result in significant right to left shunting in the upright position.
Trepopnea
This type of dyspnea occurs in lateral decubitus. The causes are pleural effusion or large mass lesions of lung.
Orthostatic Dyspnea
Orthostatic dyspnea is thought to reflect ventilation-perfusion mismatch due to inadequate perfusion of ventilated lung apices. It can even be orthostatic angina (attributed to impaired myocardial perfusion even with normal coronary arteries.
Bendopnea (JACC heart failure Feb 2014)
Definition
Shortness of breath, specifically when bending forward, such as when putting on their shoes or socks.
Mechanism
During bending, increased intrathoracic pressure leads to a further increase in ventricular filling pressures, and subjects with bendopnea (who start with higher filling pressures) are more likely to reach a threshold pressure necessary to induce shortness of breath. It is likely caused by elevation in the left-sided filling pressure, or pulmonary capillary wedge pressure (PCWP), as has been demonstrated with other manifestations of shortness of breath in patients with heart failure.
Causes of Dyspnea (Table 1)
Dyspnea can be classified into acute dyspnea at rest or chronic breathlessness on exertion (BOE).
Severity of Dyspnea Assessment
For practical purposes, we follow the New York Heart Association (NYHA), functional classification for grading the severity of dyspnea which is given in the Table 2A and B.
|
|
There are others, such as specific activity scale American Thoracic Society (ATS) and Medical Research Council (MRC) as well.
The limitations of NYHA classification:
- Subjective
|
Hence a good way of precisely quantifying the severity of dyspnea has been put forward in the specific activity scale which is given Table 3.
The original NYHA classification includes five components, but we use only the functional component.
Indicators for Heart Failure as a Cause
- Third heart sound – Likelihood ratio – 24
- Displaced apical impulse – LR 16.5
- Jugular venous distension – LR 8.5
- If all three are there, it is virtually diagnostic of heart failure.
Dyspnea and Valvular Heart Disease
- Mitral Stenosis: This is the main symptom of MS. It is due to pulmonary venous hypertension. As a rule, if patient has dyspnea + PND for more than 5 years, then MS is most likely underlying condition. The severity of dyspnea also correlates well with 10 year survival. NYHA class 2 persons survival for 10 years is only 50% whereas if class 4, it is only 20% from studies done in the prevalvotomy era.
- Mitral Regurgitation: Dyspnea is a late symptom of MR except in acute MR. It is due to pulmonary venous hypertension. The reasons for PVH are:
- Left ventricle failure
- MR with noncompliant left atrium
- Associated mitral stenosis
- Arrhythmias’ with fast heart rate, such as atrial fibrillation
- Aortic Stenosis: Dyspnea is a late symptom and survival is only about 1.5 year after the onset of this symptom. If the duration of dyspnea is more than 5 years with aortic stenosis, then suspect associated mitral valve disease. The reasons for dyspnea in AS is multifactorial:
- LV systolic dysfunction
- LV diastolic dysfunction due to LVH
- Associated mitral valve disease
- Aortic Regurgitation: Dyspnea occurs very late in the course of AR. It is also slow to progress in AR. Some patients with AR feel better on walking and this is due to the fact that on walking the heart rate increases, the duration of diastole comes down and the volume of regurgitation decreases. Exercise-induced peripheral vasodilatation may also contribute to the reduction of AR.
CHEST PAIN
Chest pain can be classified into acute, severe on going chest pain and episodic chest pain. The later form is further classified into three types, based on three features.
- Typical chest pain
- Atypical chest pain
- Noncardiac chest pain.
Typical chest pain (PQR)
- Precipitated by exertion or emotional stress
- Quality: Pressure/Heaviness
- Relieved by rest or nitroglycerin.
Atypical
Meets only two of the three above characteristics.
Noncardiac chest pain
|
| |||||||||||||||
Angina ‘Equivalents’
- Dyspnea
- Jaw or neck discomfort
- Shoulder or elbow pain
- Epigastric discomfort
- Interscapular discomfort
Blockpnea (Chevalier, American Heart Journal 1961; 73: 579 – 581)
This term was put forward by Gallavardin in the year 1933, for the feeling of blocked respiration or suffocation while walking. This is actually the dyspnea equivalent.
CCS Functional Classification for Angina
- Class 1: Ordinary physical activity, such as walking or climbing stairs does not cause angina. Angina occurs at strenuous or rapid or prolonged exertion at work or recreation.
- Class 3: Walking one or 2 blocks and climbing more than one flight of ordinary stairs in normal conditions
- Class 4: Inability to carry on any physical activity without discomfort – anginal syndrome may be present at rest.
SYNCOPE
(Greek word: syn = with; koptein = to cut or to interrupt)
Definition
Syncope is a transient loss of consciousness (T-LOC) due to transient global cerebral hypoperfusion characterized by rapid onset, short duration, and spontaneous recovery
Near syncope is defined as transient loss of postural tone. The underlying mechanism of syncope is transient global cerebral hypoperfusion.
Usual duration of syncope is not more than 20 seconds on an average (Table 5).
History taking: The following five points need to be taken in history.
- Preceding events: From the history, you must ask whether syncope happened after prolonged standing or seeing some unusual sight, such as an accident, or turning the head, etc.
Table 5 Differentiating features of seizure versus syncope SeizureSyncope1Preceding eventsNoneStanding for a long time Seeing blood2Type of onsetSuddenGradual3Position at onsetAnyStanding may be (Can occur supine)4Aura+−5Facial – Cyanosis+−6Tongue biting+−7Incontinence of Urine++/−8Duration of tonic and clonic movements> 30 secLess than 15 seconds9Post ictal amnesia+10Post ictal confusionLess than 30 secondsLonger11Post ictal headache+12Rapid recoveryMinutes to hoursLess than 5 min - Position at onset: This history is important because arrhythmia can happen in any position. However, vasovagal syncope occurs on standing for a long time.
- Postsyncopal clearing: Clearing of consciousness is gradual and takes a long time in seizures where as it is very brief in cardiac reasons.
- Associated events: Tongue biting, urinary incontinence are common with seizures.
- The single most powerful factor is postictal confusion as observed by an eyewitness. Reorientation is usually immediate in syncope and does not exceed 30 seconds even after extended attacks. (Annals of Internal Medicine, 1988; 108: 791- 796).
- Incontinence and head injury are common in both conditions. (Jour of Royal Society of Med July 1996)
Diagnostic Approach to Syncope
- Is it vertigo?
- Is it loss of balance?
- Light headed? To Transient Loss of Consciousness – T-LOC
- Seizure?
Scoring Systems for Syncope
There are many scoring systems for syncope. One of them is EGSYS score.(A. Del Roso, Heart 2008; 94: 1620) six variables are included and point weightage score is given. A score of 3 or more needs a cardiologist evaluation. This calculation application is available in the smart phone systems.
- Palpitations preceding syncope – 4
- Heart disease or abnormal ECG – 3
- Syncope during effort – 3
- Syncope while supine – 2
- Precipitating factors – minus 1
- Autonomic prodromes – minus 1.
Palpitations
Palpitations can be defined as uncomfortable awareness of heart beats.
History should include the following:
- Character of the palpitations
- Onset and offset
- Precipitating factors
- Associated symptoms
Character of the Palpitations (Lancet May 1993; 1254)
- Rapid, regular and frog positive: AV nodal tachycardia
- Rapid regular and frog negative: AVRT or AT or VT
- Rapid and irregular – AFib
- Slow and regular and frog positive: VPC
- Slow, regular and frog negative: Any VPC.
During AV nodal re-entrant tachycardia, atria and ventricles contract simultaneously, causing pronounced reflux of blood into the superior vena cava and the feeling of neck pulsations. Because of this patient may look like frog under these circumstances and this is called as frog positive by Brugada. This is also called as pounding in the neck.
Role of ECG for Clue to Diagnosis (NEJM May 1998: 338: 1369)
- Short PR: Pre-excitation
- P mitrale or frequent APC: AFib
- VPC's, LBBB with positive axis: RVOT ventricular tachycardia
- VPC's with RBBB with negative axis: Idiopathic VT – LV type
- Q waves: Old MI
- Complete AV block
- Long QT: polymorphic VT
- Inverted T in v1 and Epsilon wave: ARVD
FUNCTIONAL CLASSIFICATIONS USED IN CARDIOLOGY
- NYHA for Dyspnea
- CCS for Angina
- WHO classification in Pulmonary Hypertension
- EHRA for AFib