

INTRODUCTION
The contact lens that appears like a small wafer is designed to rest on the cornea or sclera usually for correction of refractive errors. The concept of contact lenses was borne as early as in 1500 although it took a few centuries for true contact lenses to be commercially available. The credit for conceiving the idea of contact lenses goes to Leonardo da Vinci (Fig. 1.1). In 1508, he sketched out several ideas for neutralizing the cornea through contact with fluid. He understood that corneal power could be altered by submerging the eye in a glass bowl filled with water (Fig. 1.2). Essentially, he described the principles of a contact lens without describing something we would actually recognize as a contact lens. More than a century later, Rene Descartes (1636) described a glass tube filled with liquid and attached to the eye. This was hardly a contact lens; but again, the principle of corneal neutralization was clear. Thomas Young 1801 is credited with the concept of changing the eye's dioptric power, utilizing the principle of fluid neutralization. He fitted a microscope lens at one end of a glass tube ¼ inch long, filled the tube with water, and then applied this to the eye. His device may be said to be the antecedent of hydrodiascope as well as contact lenses.



EVOLUTION
The first written description of a device approximating a contact lens is believed to date to 1823. Sir John Herschel, an English astronomer, proposed “some transparent animal jelly contained in a spherical capsule of glass applied to the surface of the eye” to correct irregular astigmatism. He also suggested that a mold of the cornea might be taken and impressed on some transparent medium. He thought that it is possible that “a temporary distinct vision” might be obtained through one of these methods, but it is not known whether Herschel ever tried to put his ideas into practice. In the late 1880s, at least three men are thought to have independently invented the first contact lens. Adolf Eugen Fick, a Swiss ophthalmologist, and Eugene Kalt, a French ophthalmologist, devised glass lenses with the goal of correcting corneal abnormalities. Eugen Fick called his contact lens Kontakt Brille. It was a small cap of thin glass made up of a spherical segment with concentric and consequently parallel faces. The space between the lens and the eye was filled with a liquid of the same refractive index as that of the cornea. He made a series of plaster mouldings, first on rabbit's eyes and then on human cadaver eyes; cups of blown glass were then shaped on these mouldings. He discovered that a well chosen shape can adhere to the eyeball. He also investigated a number of solutions to be used between the eye and the lens. He fitted the patients with corneal and scleral lenses, the scleral flange providing better support and distribution of the lens weight than his original corneal lens alone.
E. Kalt, in 1888, treated two patients with keratoconus, with corneal lenses. Unlike Fick's corneal lenses, Kalt's pressed against the cornea instead of arching over the center of the cornea.
3Around the same time, August Muller, a German medical student who wanted to correct his own high myopia, also produced a glass lens. These first contact lenses were crude by modern standards, made of blown glass bubbles or ground and polished glass, and were primarily scleral designs that covered much of the eye. They were heavy and unwieldy and let no oxygen through to the cornea. Patients could tolerate the lenses only briefly and usually suffered from signs and symptoms of corneal hypoxia rather quickly. Nevertheless, the improvement in visual acuity that a piece of glass on the eye could provide was encouraging.
Between 1890 and 1935, there were no developments of any great consequence. Two German companies, Karl Zeiss Optical Works and Mueller Co., as well as small labs in the US and elsewhere, continued to make glass contact lenses but demand was very limited. In 1889, Muller Gladbach of Wishaden corrected his own refractive error of 14D with a type of corneal glass contact lens. However, he could hardly wear the lenses for more than 30 minutes. He recognized that the cause of the intolerance was not the lens on a cornea but the crushing of the conjunctival vessels by the rough edge of the lens. He attempted to solve the difficulty, but finally gave up. Muller was the first to use the term corneal lenses but his lenses would be termed scleral today. In 1887, the German ophthalmologist Eugen Fick constructed and fitted the first successful contact lens. He described fabricating afocal scleral contact shells, which rested on the less sensitive rim of tissue around the cornea, and experimentally fitting them initially on rabbits, then on himself, and lastly on a small group of volunteers. These lenses were made from heavy blown glass and were 18–21 mm in diameter. Fick filled the empty space between cornea and glass with a dextrose solution. Fick's lens was large, unwieldy, and could only be worn for a couple of hours at a time.
The contact lenses so far described had poor optical surfaces and often gave bad visual acuity. Their primary objective was therapeutic. They were individually blown in glass. Sulzer, also of the same period, made scleral lenses by grinding from solid glass in much the same way as glass spectacle lenses were grounded. These scleral lenses, blown either to a shape after the method of Muller or grounded to a two-curve spherical design by Carl Zeiss of Jena, were then used up to beginning of the 20th century.
The twentieth century saw the full refinement of the contact lenses that we enjoy today. Many modern day manufacturing techniques and man-made products (such as plastics and silicone) go towards making contacts that the body can easily tolerate and which are much more comfortable to wear for extended periods.
In 1929, Heine described a method of fitting contact lenses by means of a trial set consisting of a large number of contact lenses, made for him by Zeiss. Glass contact lenses used so far were usually of the scleral type, the weight and irregular surfaces of the corneal type precluding their proper adherence to the cornea, thus restricting their use. In 1929, Joseph Dallos, a Hungarian physician, developed methods of taking molds from living human eyes so that glass lenses could be made to conform more closely to individual sclera. Glass-blown scleral 4lenses remained the only form of contact lens until the 1930s when polymethyl methacrylate (PMMA or Perspex) was developed, allowing plastic scleral lenses to be manufactured for the first time. In 1936, William Feinbloom, a New York optometrist, introduced the use of plastic for contacts. He made a lens having a glass corneal portion and a plastic scleral portion. Its lightness, workability and comfort with ocular tissue were advantageous factors.
Rohm and Hass Company (USA) in 1936 introduced transparent methyl methacrylate. The same year, John Mullen and Theodore Obrig developed techniques for making scleral lenses of the new substance by the much simpler process of turning it on a lathe. These lenses could be shaped and reshaped at low temperatures, scraped, routed drilled or buffed, quickly finished to a high polish and made thinner than was possible with fragile glass. Obrig is also known for introducing the use of fluorescein in ultraviolet light for checking the fitting of contact lenses over the cornea.
Scleral lenses used so far usually led to temporary corneal edema and to clouding just a few hours after lens insertion. In 1943, Bier introduced a minimum clearance fluidless, performed contact lens called the transcurve lens as it included a transitional curve between the scleral and corneal curves. He perforated these lenses to allow ingress and egress of natural tears, thus greatly ameliorating the corneal clouding. In 1946, Nissel in England used a similar wide-angle lens, which differed in having a flat transition between the corneal and scleral porions.
The first corneal plastic contact lens was introduced in 1947 by Kelvin Tuohy. It was approximately 11 mm in diameter and 0.4 mm thick, the back curve being flatter than the corneal curvature by 1.50 diopters. In 1950, an Oregon optometrist, Dr George Butterfield, designed a corneal lens. The inner surface of this lens followed the eye's shape instead of sitting flat, increasing comfort and eye tolerability. This also reduced problems with image and peripheral vision distortion in certain prescription types.
In 1951, Sohnges of Germany, Dickinson of England and Neill of USA simultaneously introduced the micro-corneal contact lenses about 9.5 mm in diameter 0.2 mm thick and fitted 3–4 D flatter than the corneal curvature. The diminished size, thickness, and greater curvature permitted better tear circulation to the cornea. Hence, they were much better tolerated. In 1955 Norman Bier introduced a new principle of fitting the contact lens spoken of as “contouring the cornea”, paralleling the cornea or “corneal alignment”. It implies that the contact lens has multiple inside radii, the lens thus being in contact with the cornea quite uniformly except at the very periphery of the lens. Corneal contact lenses now being constructed were small and thin, and they were either parallel to the cornea or vault its apex in which case they are called apical clearance lenses. They were now fitted as small as 7–8 mm in diameter.
During 1960's in Prague, Czechoslovakia, Otto Wichterle and Drahoslav Lim experimented with contact lenses made of a soft, water-absorbing plastic they had developed. This was the major step leading to the soft and disposable lenses that we have today. The water absorption helped with eye dryness problems that could lead to irritations, eye tiredness and focusing problems. The polymers from 5which soft lenses are manufactured improved over the next 25 years, primarily in terms of increasing the oxygen permeability by varying the ingredients. In 1972, British optometrist Rishi Agarwal was the first to suggest disposable soft contact lenses.
In 1979 Rigid gas permeable (RGP) contact lenses made of co-polymers PMMA and silicone became available for commercial distribution. Many silicone-acrylate lenses became available at this time. Gas permeability allows the eye to maintain its natural moisture and to refresh its surface tear layer without hindrance. The 1980s saw the development of tinted daily wear soft lenses which became available for commercial distribution. This was one of the first soft colored contact lenses in the market. In 1982 bifocal daily wear soft contact lenses became available for commercial distribution.
In 1998, an important development in soft lenses was the launch of the first silicone hydrogels into the market by CIBA VISION in Mexico. These new materials combined the benefits of silicone, which has extremely high oxygen permeability, with the comfort and clinical performance of the conventional hydrogels which had been used for the previous 30 years. These lenses were initially advocated primarily for extended (overnight) wear although more recently, daily (no overnight) wear silicone hydrogels have been launched.
An important development in the history of gas permeable contact lenses started when in 1989, Paul Rose of New Zealand began developing the Rose K keratoconus lenses. After testing 700 lenses and 12 different designs, he produced a set of 26 lenses from which all patients could be fitted. A further two years were spent to perfect the lens design before it was launched in the New Zealand market. In 1995, Rose K lens gained approval from the Federal Drug Administration (FDA) of America. Since then, advances in technology have resulted in the introduction of the Rose K2 lens, the Rose K2 Irregular Cornea (IC) lens, the Rose K2 Post Graft (PG) lens, and the Rose K2 NC lens for nipple cones designed for patients with specific conditions. These conditions include pellucid marginal degeneration, keratoglobus, LASIK-induced ectasia and patients who have undergone penetrating keratoplasty.
APPENDIX
Nomenclature
Contact lens specification can be better understood by the practitioners if a uniform nomenclature is used. The author has used the following in this text.
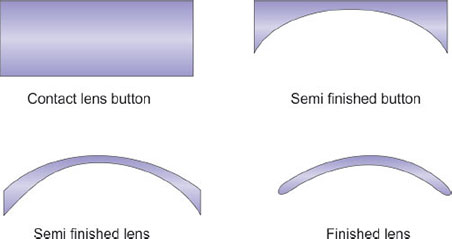
- Contact lens blank: A circular button of plastic 12.55 mm diameter, 7.50 mm thick (Fig. 1.3).
- Semi-finished blank: A blank where base curve has been generated and polished.
- Finished contact lens: A properly edged semi-finished contact lens (Fig. 1.6).
- Diameters
- Overall diameter (OD): The dimension across the physical boundary of the lens, expressed in mm (Fig. 1.6).
- Optic zone (OZ): The dimension of central optic zone of the lens meant to focus the rays on the retina.
- Curves
- Base curve (BC) or central posterior curve (CPC) on the back surface to fit the front surface of cornea.
- Peripheral posterior curves (PPC) are concentric to the BC, and usually two in number, i.e. intermediate posterior curve (IPC) and peripheral posterior curve (PPC). They are meant to serve as reservoirs of tears and to form a ski for lens movements.
- Front curve (FC) or central anterior curve (CAC) is the central zone on the front surface corresponding to the optical zone, and its curvature determines the lens power.
- Peripheral anterior curves (PAC) which are two in number are curves on the front surface. The intermediate anterior curve (IAC) is only fabricated in high minus and high plus lenses. The peripheral anterior curve (PAC) is slope going to the edge of the lens.



NB: The radii of all curves are expressed in mm or diopters.
- Edge is the union of front and back curves at the periphery (Figs 1.7A and B)
- Power is always described as the back vertex power.
- Blend: This is curve to knock off the sharp junction between two curves and has a value between the two surrounding curves.
- Thickness is usually measured in mm at the center of the lens.
- Tint is the color of the lens with each color having light, medium and dark shades.
- Corneal zones: The cornea can be divided keratometrically into three zones:
- Apical zone, centrally located 3–9 mm in diameter (usually), and the most steep and most uniform in curvature.
- Limbal zone, in the peripheral part of cornea where the mires of keratometer appear doubled.
- Transitional zone joining apical and limbal zones.
- Corneal centers (Fig. 1.8): Cornea has three centers:
- Geometric center, the intersection of widest and shortest diameter of the cornea.
- Apical center, the intersection of the widest and the shortest diameter of the apical zone.
- Visual center, the point on the cornea which transmits the visual axis.
- “K” refers to the flatter of the two meridian in keratometry.

