

Learning is not attained by chance. It must be sought for with ardor and attended with diligence.
Abigail Adams
A teacher can never truly teach, unless he is still learning himself.
Rabindranath Tagore
Educationists now lay more emphasis on “teaching–learning,” as compared to the greater importance previously given to “teaching” alone. We are now more interested in understanding what and how students learn, why some of them do not learn, and when do they learn better. Learning, especially in medicine, has a direct relevance to the health needs of the society. Application of knowledge depends on the context in which the students have learnt. Hence, the attention is more focused on learning and the learner. Let us look at these terms in little more detail.
Teaching aims to facilitate learning and helps the learners to learn more effectively. The purpose of teaching is not merely dispensing information, but to also develop skills, good communication, attitudes, and values.
It is wrong to presume that all the information transmitted to the students is always learnt, or since that does not happen, a lot more 2information should be transmitted so that something will be learnt! It is also wrong to presume that students are immature and irresponsible. The students tend to behave in a manner similar to what they are considered to be. If they are considered to be responsible, they will behave in a responsible manner.
TEACHING
The role of a teacher is not of bossing around and being authoritarian. The role of a teacher is to be a considerate and a friendly person, who creates an appropriate atmosphere for effective learning, so that learning is an enjoyable and a pleasurable process.
Are we, as teachers, able to create such an atmosphere in our institutions? Let us consider in this context, learning in more detail.
LEARNING
Learning is a process resulting in some changes or modifications in the learner's way of thinking, feeling, and doing as a result of practice. The change may be temporary or permanent. The more effective the learning experience, better is the learning. Provision of effective learning experiences depends on the teacher. Depending on the ability of teacher to provide a meaningful learning experience, the quality of learning would vary.
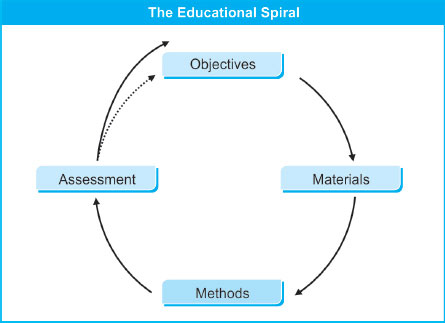
Learning is a cyclical process; however, it can also be considered as an uprising spiral motion where with time, there is a change in the level of attainment. It is this sequence that can be referred to as learning spiral and makes learning a dynamic process.

When and where one gets the new experiences and how often these are repeated are referred to as learning opportunities. A new experience or a new piece of information may be first heard or seen during a lecture 3and may be accepted and analyzed as something relevant and important. On reflection, it may seem to be significant for some purpose. On recall, it may be spoken aloud or written/drawn on a paper, analyzed to be incompletely recalled, may be read further in the library or may be discussed with peers, and ultimately may become a part of the permanent memory. This is how learning occurs. Learning is to progress from one step to another.
Learning is individual: We all learn different things at different rates. Hypothetically anybody can learn almost anything, given sufficient time and resources. However, at a practical level, our learning is limited. We all learn different things attaining different levels of achievement.
The scope and magnitude of learning depends to a large extent on the individual. For example, those who prefer “sensing” would learn better about those things which they can see, hear, or touch, whereas those who prefer “intuition” would like subjects that allow to create abstract ideas. Ideas and hypotheses would fascinate them. However, this is not to “brand” the learners into one or more types—rather it allows the teacher to deliver a “bouquet” from which the learners can learn by not only their own style but also challenge themselves to adopt a different learning approach.
How we Learn: Let us try to have a look at the psychology of learning. We presume that most of you are aware of how computers work and this provides a good representation of how people learn. Broadly, any new information is first put in the working memory (equivalent to the RAM of computers, which is lost if you do not save it and switch off the computer). Working memory can hold only 4–5 bits of new information, for about 10–15 seconds. If this information is considered worthwhile, it is transferred to short-term memory. As the name indicates, this can retain the information from few minutes to few hours. The information will be lost if it is not transferred to long-term memory (equivalent to hard disk of the computer). Information stored in the long-term memory is relatively permanent and can be retrieved if stored properly (just like saving a word file at the proper place, so that you know where you have stored it). However, like hard disk, long-term memory can also get corrupted and may need to be written over many times for it to become long lasting. It is interesting to note that there is no “delete” function in human brain—so what you have apparently forgotten has not gone anywhere. Rather it is buried under new information and with effort and practice, can be retrieved. Many of us can recall even minor but pleasant events of our childhood. This depends on the perceived importance of the information and its link with other sets of information.
PSYCHOLOGY OF LEARNING
You have guessed it right. The simplest way to improve the retention of information is to transfer it to short-term and then long-term memory. 4As teachers, you can try some simple interventions to improve the process. These include:
IMPROVING RETENTION
- Encouraging students to shift the information from working memory to long-term memory. This can be done by planned repetitions (you must be remembering Baa, Baa, Black Sheep still because your teachers made you repeat this many times even after you learnt it by heart), or telling about the utility of new information (e.g., role of basic sciences information in clinical work). Similarly, teaching someone else requires recall of information and its interplay with new information. This is the reason for the phrase to teach is to learn twice. Peer learning or team learning makes use of this principle.
- Encouraging students to recall what they already know so that connections with new knowledge can be formed. This also helps in easy understanding by making it a part of habit to recall earlier knowledge.
- Working memory can be managed by increasing the number of channels through which information is being transmitted. Using words and diagrams, for example, increases the capacity of working memory. We will discuss more about practical application of this in Chapter 12. Mnemonics, flowcharts, concept maps, etc., are common tools to manage working memory and prevent the information from getting lost. Interestingly, co-curricular activities, such as music and theater tend to improve learning by training the students to better manage their working memory.
- Reducing the cognitive load by reducing the demands on working memory. For example, while teaching interpretation of an arterial blood gas (ABG) report, a quick revision of acid–base balance will markedly reduce the cognitive load.
MANAGING MEMORY
Principles of Learning
Now let us consider some basic principles of learning:
- Relevance: Learning is better with subject matter of immediate relevance. When the relevance is remote or obscure and the student has to learn with a belief that the knowledge perhaps might be of use someday, learning is difficult. However, a student can be motivated to learn effectively by explaining the importance of subject matter with reference to his ultimate goal, e.g., the future clinical practice in the community. This could mean that some of the basic principles are relevant and important to be learnt now and some finer details could be learnt later.
- Sequential learning: We learn by progressing from simple to complex matters. A suitable example or interesting anecdote may attract the learner's attention and through it some facts and principles can be communicated.5Learning is better, when it progresses from an observation to reasoning, from a particular point to generalization, and from a particular experience to an abstract concept. However, sequence is a matter of commonsense, and it is not essential to adhere to any rigid order or sequence while teaching a subject matter. Depending on the topic to be explained or taught and depending on the learning atmosphere and opportunity, the learning sequence can be altered and adjusted accordingly. When integrating subject matter across disciplines, teachers may have to move away from traditional sequencing to incorporate other disciplines or to have their subject incorporated in the ongoing teaching–learning activities.
- Cumulative learning: We learn by building on what we already know. An implication of this is that prior knowledge needs to be activated to build new learning. If prior knowledge is not there or is not activated, then it will become very difficult to build new knowledge. As an example, if we do not use the existing knowledge of anatomy before teaching pathology, we will never be able to complete pathology within the given time frame. Of the three principles stated here, this seems to be the most important, not only in theory but also from practical point of view. It reduces time and resources needed to learn. Failure to use it is one of the commonest causes of learning difficulties faced by the students. As discussed later in this chapter, cumulative learning is considered the most important aspect of adult learning.
Improving Learning
PROCESS OF LEARNING
Let us now have a look at some of the factors, which promote learning:
- Active involvement: Learning is more effective with an active involvement of the learner in the process, e.g., a small group discussion would be more effective for learning than a lecture. Active involvement allows the learner to interact with the subject matter, peers, and teachers, thereby increasing learning, assimilation, and retention.
- Formative assessment and feedback: Learning, being a process of acquiring new knowledge and skills, enables the students to do something that they could not do before. Providing feedback on their performance helps the students to learn better. Feedback has been shown to have the single most important influence on learning. Feedback, to be authentic, has to be based on a system of ongoing assessment. This helps not only the students by making them aware of their deficiencies but also helps the teachers to modify their teaching styles. You will learn more about it in Chapter 13.6
- Driving effect of assessment: The system and process of assessment has a direct effect on learning and learners. Students are generally blamed to be examination oriented. Given the fact that students learn for the sake of examinations, assessment can be utilized for better learning. For example, if more questions are asked regarding the common health problems faced by the community, students would work more for those topics and would learn more about them. Given a choice to choose between what is taught and what is asked, students will always prefer what is asked. As a teacher, you can always use this driving force to channelize students’ learning in a particular direction.
- Social and cultural ethos: The degradation of social and cultural values is affecting education also. Medical education is no exception. An observation that non-deserving candidates may score better does affect the learning behavior in a negative manner. Maintaining a positive atmosphere in the educational institutions is the joint responsibility of all teachers and students. The educational environment within an institution also affects teaching–learning to a significant extent.
ADULT LEARNING
It may be interesting to look at the characteristics of adult learners as identified by Knowles. Students do not come to us like a blank slate—they have their prior knowledge (right or wrong), they have their own beliefs about learning, and they work toward certain goals (e.g., a career in research, community-based practice, or super-specialization). Unlike school children, they do not learn for the sake of learning—they will always look for the practical utility of that knowledge and they will not learn simply because we tell them to learn something that is “important.” As teachers, you have to keep this in mind. This may, in fact, be one of the reasons why we prefer to call teachers as “facilitators” of learning rather than information providers. The salient characteristics of adult learners are summarized in the box below. Many of these are liberally used in designing instruction for adult learners (e.g., medical students).
Learning Strategies
Let us also introduce you to the concept of types of learning. It is possible to identify three distinct types of learning strategies adopted by the students. These are described below:
TYPES OF LEARNING
- Surface learning: This refers to a superficial approach to learning with the purpose of being able to recall information. Knowledge is stored in bits and pieces, and generally, there is no connection between these pieces. Knowledge acquired this way is short lived. Rote learning is a typical example of surface-learning approach. Certain instruction and assessment methods, e.g., asking only recall type of questions, will direct the students toward superficial learning.
- Deep learning: This implies learning with the purpose of understanding. It is a slower process during which the learner tries to form connections between his prior knowledge and the new knowledge as well as between different pieces of knowledge. The purpose is to be able to apply this knowledge. This type of learning promotes retention, recall, and application. This requires spaced practice over a period of time. Certain teaching methods, such as problem-based or case-based learning and certain assessment methods, such as asking contextual or problem-solving questions will promote deep learning.
- Strategic learning: This is the strategy used by students to do well in an examination. Learners try to categorize information by its utility for scoring good marks. Categorization of topics as “important” is an example of strategic learning. This also promotes short-term knowledge, which is often forgotten after the examinations. However, you can give a direction to such learning by “forcing” students to recall and activate their prior knowledge during teaching and assessment.
Teaching
Some teachers have an inborn gift of the art and skills of teaching, but most of us learn and develop the skills as we progress in our career. Teaching is an interaction between the teacher and student under the former's guidance in order to bring about expected changes in the latter's behavior.
What is the Purpose of Teaching?
The purpose of teaching is to facilitate learning. Meaningful and effective teaching should help the student to:
- Develop proper lifelong learning habits and attitudes
- Acquire, retain, and apply the knowledge
- Achieve appropriate skills and use them with confidence.
Most teachers are interested in teaching effectively and some may work for an improvement in their methods. The technique of microteaching should be useful for such teachers. Later in the book, you will find a discussion on this simple technique for improving your teaching skills.
Effective Teaching
Often, teachers find themselves confronted with a large number of students, a vast body of knowledge to be comprehended, a rapidly changing field of information in many areas, and a limited time available for teaching in which students are expected to achieve a maximum level of understanding. Therefore, the teacher may have to consider what experiences will motivate the students and enable them to learn; how the information can be structured for a given group; which sequence and form of presentation would be most effective; and how the individual differences amongst the students can be taken care of.
QUALITIES OF A TEACHER
You may find it interesting to look at the traits that students look for in their teachers. One such example is given in the box below. You will appreciate that though teaching style and your communication skills are important, they are not a replacement for your subject expertise. Subject expertise gives you the confidence to teach. Putting these two together, it is imperative that faculty development should focus not only on developing your teaching and managerial skills but also on improving your subject knowledge.
9
What to Teach?
CATEGORIZATION OF CONTENT
To learn everything in the field of medicine is impossible even in a lifetime. Some form of selection is therefore essential. A type of stratification is also necessary. You can categorize the subject matter into three, viz. must know, should know, and nice to know. Another type of classification is to divide the subject matter into core and non-core. Broadly, core coincides with the must-know area. Since time is limited, the major aim of your teaching should be to teach the vital and most of the essentials. The desirables could only be mentioned or suggested for self-study.
Making this type of stratification also helps you to design the assessments properly by including all the must-know or core areas in certifying examinations.

How to Teach?
We usually teach the way we were taught, unless there are reasons for a change. How we teach also depends on how much we care for the students, for the subject, and for our reputation as a teacher; how much we respect ourselves, our students, our subject, and our institution; and how much concern we have for the welfare of the students, community, and the institution. If we do care, respect, and have reasonable concern, it does not matter how we teach—it would automatically be effective and interesting. Perhaps, there is nothing like the way of teaching.
Teaching–learning process is therefore a complex phenomenon. It should an open-ended spiral movement as compared to the linear model of conventional teaching. Considering the dynamic status of medical knowledge today, a medical teacher has to be a lifelong learner himself to keep up-to-date and be well-informed about recent advances in different fields.
Although we will discuss more about it in the next chapter, we must introduce you at this point to the systems approach. A system refers to a collection of components, which are interdependent. Pancreas, 10adrenals, liver, and brain are part of a system responsible for maintaining blood sugar levels. The key feature of this relationship is the ability to influence the functioning of others as well as get influenced in the process of attaining the desired outcome (i.e., maintaining blood sugar). In educational settings, objectives, materials, methods, and assessment are all part of a system, as are the students, teachers, society, and educational institutions. In its most simple form, an educational system can be represented by an input–process–output model. We have lectures and practical, the student processes this information in his mind and then is able to do something, which he could not do earlier (i.e., has learnt). This is called an educational system and can be diagrammatically represented as follows:
SYSTEMS APPROACH

The output in this model has no influence on the input or process. However, when we add a component of feedback, i.e., assessment data being used to modify teaching methods or teaching materials, then the system can self-correct the inputs as well as processes to produce optimal output.

The key concept of systems approach is that each of the components influences and in turn gets influenced by them. For example, any change in objectives demands a parallel change in examinations and any change in examinations also demands a corresponding change in teaching methodology. This concept of systems thinking is crucial, especially when we are contemplating any change. Changing only one component and ignoring the others is likely to fail and sometimes even disrupt productivity.
The present book is an attempt to induct medical teachers into the teaching–learning process. On the basis of what has been discussed in 11the preceding pages, it is possible to identify three distinct components of this process. These include:
- Learning objectives
- Subject matter and teaching methodology
- Assessment
In the chapters that follow, we have tried to retain this basic format for our discussion. Let us emphasize here that all these components are inter-dependent and any of them cannot be sustained without adequate support from the others.
Happy reading!!
True teachers are those who use themselves as bridges over which they invite their students to cross; then, having facilitated their crossing, joyfully collapse, encouraging them to create their own.
Nikos Kazantzakis