

IMPORTANT ANATOMICAL LANDMARKS
One should have a clear understanding of anatomy of the respiratory system to perform a proper physical examination. Some of the important anatomical landmarks are outlined below.
The upper respiratory tract starts from the mouth or nose and includes all the structures in the mouth, nose, and sinus up to the larynx (the details of which will be discussed later). Lower respiratory tract starts from the lower border of cricoid cartilage which includes the trachea, airways, and lung parenchyma containing alveoli.
Trachea
- Starts from cricoid cartilage (lower border of larynx at the level of 6th cervical vertebra posteriorly) to sternal angle anteriorly (angle of Louis) and T5 spinous process posteriorly, where it divides into left and right main stem bronchi. The inner diameter is 25 mm and the length is about 10–16 cm.
- Trachea has intra- and extrathoracic components. This has important bearing in the understanding of physiology of variable obstruction.
The spinous process is an important landmark because of its prominence and thoracic spines can be counted below it.
Angle of Louis
- Angle of Louis is the angle between the body of sternum and manubrium. Many important landmarks occur at this level:
- 2nd rib articulates with manubrium sterni at this site. The ribs are counted anteriorly starting from this point.
- Carina of trachea is at this level and it branches into right and left bronchi.
- Mediastinum is divided into superior and inferior at this level.
With the help of surface anatomy, the thorax is arbitrarily divided into various spaces and lines. Description of abnormal signs in relation to the ribs, intercostal spaces (areas), and lines help to localize the lesion anatomically (upper lobe, lower lobe, middle lobe, etc.).
It is a significant anatomical landmarks as:
- Ribs are counted from this level to downward. 2nd rib lies at sternal angle.
- It marks the plane of separation of superior and inferior mediastinum.
- Ascending aorta ends, arch of aorta starts and ends, and descending aorta begins at this level.
- Azygos vein arches over the roof of the right lung and opens in superior vena cava (SVC).
- Pulmonary trunk divides into two pulmonary arteries below this level.
- Thoracic duct crosses from right to left side and reaches left side at the level of sternal angle.
- It marks the upper limit of the base of the heart.
- Cardiac plexus are situated at the same level.
Ribs
Anteriorly ribs are counted down starting from 2nd rib. There are 12 ribs and 11 interspaces in each hemithorax. You can also count up from 12th rib. Inferior angle of scapula overlies 7th thoracic rib posteriorly.
Spaces/Areas (Chest Topography)
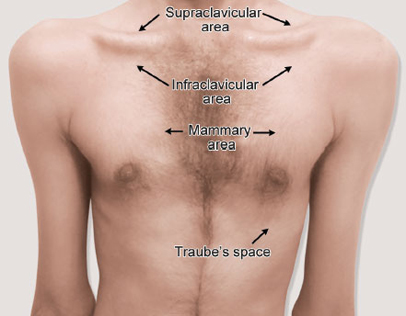
Anteriorly, the spaces are supraclavicular, infraclavicular and mammary, and Traube's space (Fig. 1).
- Supraclavicular: Space above clavicle.
- Infraclavicular: Space below clavicle up to 2nd intercostal space.
- Mammary: Space below infraclavicular area, i.e., 2nd to 6th intercostal space
- Traube's (semilunar) space: It is a crescent-shaped space, encompassed by the lower border of the left lung, the anterior border of the spleen, the left costal margin, and the inferior margin of the left lobe of the liver. Thus, its surface markings are respectively the left 6th rib superiorly, the left anterior axillary line laterally, and the left costal margin inferiorly. In other words, left 6th rib in the midclavicular line to 8th costal cartilage in the parasternal line, then along the left costal margin to the 11th rib in the midaxillary line and then the 9th rib in midaxillary line.4

Laterally, the spaces are axillary and infra-axillary spaces bound in between by two axillary folds. Anterior axillary fold is formed by pectoralis major muscle and posterior axillary fold by latissimus dorsi and teres major muscles.
- Axillary area: Space up to 5th intercostal space in midaxillary line (on the right where the horizontal fissure meets the oblique fissure).
- Infra-axillary area: Below the 5th intercostal space to 7th intercostal space.
Posteriorly, the spaces are suprascapular, interscapular, and infrascapular spaces (Fig. 2).
- Suprascapular area: From the apex to the spine of scapula.
- Infrascapular area: From the angle of scapula to the 11th rib.

Lines
Following are the imaginary vertical lines in the chest: Midsternal, parasternal, midclavicular, anterior axillary, midaxillary, posterior axillary, infrascapular, and vertebral lines (Figs. 3 to 5).
- Midsternal line: A vertical line down the middle of sternum.
- Parasternal line: A vertical line along lateral edges of sternum.
- Midclavicular line: A vertical line from midpoint of clavicle.
- Midaxillary line: A vertical line at midpoint between anterior and posterior axillary line. There is less muscle attachment here, so it is the ideal place for putting intercostal drain and for thoracoscopy incision. This is also called safe triangle because there is less risk of injuring blood vessels like internal mammary artery and damage to muscle and breast tissue.
- Safe triangle: It is bordered by the anterior border of the latissimus dorsi, the lateral border of the pectoralis major muscle, inferiorly by horizontal line from the nipple (5th intercostals space) just above the rib (to avoid neurovascular bundle) and superiorly by the axilla.
- Posterior axillary line: Along posterior axillary fold.
- Scapular line: Starting from the suprascapular area passing down the inferior angle of scapula.



Surface Anatomy of Lungs
Right Lung
With a marking pen, start 3 cm above clavicle in midclavicular line, come down along right parasternal line, to join 6th rib in midclavicular line, to 8th rib in midaxillary line and to 10th rib posteriorly. Posterior marking of lung is from the apex to 10th thoracic vertebra posteriorly.
Left Lung
Start 3 cm above clavicle in midclavicular line and draw a line going downward along the parasternal margin up to 4th costal cartilage. Between 4th and 6th costal cartilage, deviate to left by 4 cm. The lower levels of lung—6th rib in the midclavicular line, 8th rib in the midaxillary line, and 10th rib in the scapular line.
Kronig's Isthmus
It is an area about 5–7 cm in the supraclavicular region. It is bound medially by scalenus muscle, laterally by acromion process of scapula, anteriorly by clavicle, and posteriorly by trapezius muscle.
Clinical Significance
Normal percussion over Kronig's isthmus is resonant. The percussion note becomes hyperresonant in emphysema and impaired in early tuberculosis and apical lung tumors.
Oblique fissure extends on the left from the tip of spinous process of the T3 vertebra that extends down to the level of 6th costochondral junction anteriorly. In taking this route, the approximate path of the 6th rib is followed. The posterior origin of the fissure on the right is slightly inferior—the inferior margin of the T4 vertebra. If the subject keeps his hands on the head, the line drawn from the spinous process of the above vertebrae T4 on the right and T3 on the left along the lower border of the scapula to the level of 6th costochondral junction.9

FIG. 6: Anterior surface markings of the lung lobes.(LLL: left lower lobe; LUL: left upper lobe; RLL: right lower lobe; RML: right middle lobe; RUL: right upper lobe)

FIG. 7: Posterior surface markings of the lung lobes.(LLL: left lower lobe; LUL: left upper lobe; RLL: right lower lobe; RUL: right upper lobe)
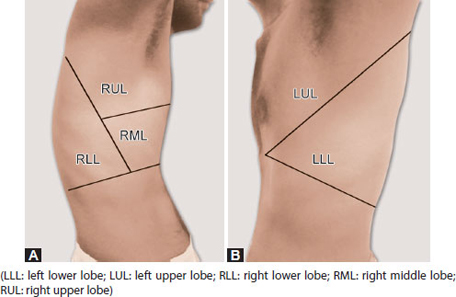
FIGS. 8A AND B: Lateral surface markings of the lung lobes. (A) Right lung; and (B) Left lung.(LLL: left lower lobe; LUL: left upper lobe; RLL: right lower lobe; RML: right middle lobe; RUL: right upper lobe)
Transverse fissure starts from the level of the right 4th costal cartilage horizontally to a junction with the oblique fissure at approximately the midaxillary line in the 5th intercostal space.
Remember there are three lobes on the right side and two lobes on the left side normally.
Once the fissures are drawn, one can easily recognize the surface anatomy of lobes of lungs. One can then appreciate the importance of examining the patient in all anatomical areas mentioned above to identify the lobes. Most of the lower lobe is in back, the upper lobe is in front, and the middle lobe is in front and in the axilla all the three (right) lobes are present.11
Bronchopulmonary Segments
It is a wedge of lung tissue supplied by a single bronchus and corresponding pulmonary artery and vein. There are ten segments in right lung and eight segments in left lung (Table 1).
Muscles of Respiration
There are two types of muscles of respiration—principal and accessory muscles.
Principal muscles are used during normal inspiration while accessory muscles are used during forced breathing (heavy exercise and exacerbations of obstructive airway diseases).
Principal muscles include external intercostals, interchondral part of internal intercostals, and diaphragm.
The width of the thoracic cavity (lateral and anteroposterior diameter) is increased by external and interchondral part of internal intercostals which elevate the ribs. The lateral dimensions of the thorax are increased by the bucket handle movement of the ribs. Diaphragm contracts to increase the vertical dimensions of thoracic cavity and also aids in elevation of lower ribs and abdominal contents are pushed downward. Accessory muscles of inspiration are sternocleidomastoid which elevates the sternum and scalene muscles (anterior, middle, and posterior) elevate the first two ribs.
Remember to look for alae nasi when the patient is in respiratory distress that means a fall in forced expiratory volume in the first second (FEV1) by 30%.
Muscles of expiration: It is passive as no muscle involvement in normal breathing. The process is simply done by elastic recoil of the lungs and the rib cage.
But during active breathing (exercise), the interchondral part of the internal intercostal muscles assists in active expiration by pulling the ribs downward and inward. They also prevent bulging of intercostal spaces during straining such as vigorous coughing and vomiting. The abdominal muscles when contract (rectus abdominis, external oblique, internal oblique, and transversus abdominis), intra-abdominal pressure increases and push the diaphragm upward and force the air out of the lungs.13
Diaphragm (Fig. 9)
The diaphragm is a dome-shaped structure containing muscle and fibrous tissue that separates the thoracic cavity from the abdomen. The dome curves upward. The superior surface of the dome forms the floor of the thoracic cavity and the inferior surface of the dome forms the roof of the abdominal cavity.
As a dome, the diaphragm has peripheral attachments to structures that make up the abdominal and chest walls. The muscle fibers from these attachments converge in a central tendon, which forms the crest of the dome. Its peripheral part consists of muscular fibers that take origin from the circumference of the inferior thoracic aperture and converge to be inserted into a central tendon.
The muscle fibers of the diaphragm emerge from many surrounding structures. Anteriorly, fibers emerge from behind the xiphoid process and the cartilages of the floating ribs (ribs 7–12). Laterally, fibers emerge from the sides of the ribs themselves, including the two false ribs 11 and 12. Posteriorly, fibers emerge from the abdominal wall and lumbar vertebrae. There are two lumbocostal arches, medially and laterally.

Crura and central tendon: The left and right crura are tendinous in structure and blend with the anterior longitudinal ligament of the vertebral column.
The central tendon of the diaphragm is a thin but strong aponeurosis situated near the center of the vault formed by the muscle, but somewhat closer to the front than to the back of the thorax, so that the posterior muscular fibers are the longer. Once the diaphragm has been outlined, you can appreciate that the pleural gutter is deep posteriorly. Fluid, thus, tends to accumulate posteriorly.
Mediastinum (Fig. 10)
Mediastinum is the space between the lungs from inlet to outlet of thorax. Superiorly, by suprasternal notch. Anteriorly, it is in between parasternal lines. Posteriorly, by vertebral line. Inferiorly, it extends to xiphisternum. Mediastinum is narrow posteriorly and widens anteriorly. Since the inlet of thorax is slanted, only posterior mediastinum extends to neck.
Sternal angle separates superior from inferior mediastinum. The inferior mediastinum is divided into anterior, middle, and posterior compartments. The space in front of the heart is anterior mediastinum and behind is posterior mediastinum. Heart itself defines the middle mediastinum. The posterior mediastinum is divided into two, i.e., paravertebral and prevertebral space. Superior mediastinum extends into the neck and is called cervicomediastinal space.
It is important to know the structures in each compartment. It is important to differentiate the masses in the mediastinum in relation to the structures there.15

Pleura and Pleural Sacs
Parietal and visceral pleura covers the surface of the lung. Parietal pleura lines inner surface of rib cage and outer portion of each hemidiaphragm is supplied by intercostal nerves and this is one reason for localized chest pain.
The pleura in the central region of each hemidiaphragm is innervated by fibers that travel with the phrenic nerve (C3–C4). So, in infection involving this area, the pain extends to ipsilateral neck or shoulder even to the abdomen presenting as acute abdomen. Parietal pleura has innervations and is pain sensitive but not the visceral pleura.
The pleural sac extends to 8th, 10th, and 12th rib in the midclavicular line, the midaxillary line, and scapular line, respectively at the lower level. There is a difference in the pleural reflection on the left side because the lung and the pleura from midsternal line lie at a higher level, i.e., at the lower border of the 4th costal cartilage. The superficial cardiac dullness is obtained in this area because the heart is uncovered.16
Hilum
Hilum lies opposite to the spines of 4th, 5th, and 6th thoracic vertebrae. Left hilum is at a higher level.
Costal Angle
Costal angle (subcostal angle) is formed by the 10th rib with costal cartilage on both sides and xiphisternum in the middle. The normal angle is not >90° but more acute in males. Both the sides are symmetrical. Volume changes in each hemithorax will alter this relationship. Hyperinflated lungs will increase the costal angle. In alar chest, anterior–posterior distance is reduced. Diaphragmatic paralysis also alters the symmetry of costal angle.
Spinous Process
The most prominent spinous process is of 7th cervical vertebra. You can count down the thoracic vertebra and the ribs using this landmark.
To conclude, this chapter will throw light on the essentials of anatomy of thorax which will help in locating anatomical lesions with precession.